Health
National pharmacare – might it be a pig in a poke?

From the Macdonald Laurier Institute
By Nigel Rawson and John Adams for Inside Policy
No Canadian should have to choose between paying for medicines and paying for rent or food. National pharmacare has been proposed as a remedy to this situation.
“When will Canada have national pharmacare?” asks the author of a recent article in the British Medical Journal (BMJ). Better questions are: will Canadian pharmacare be the system many Canadians hope for? Or, might it turn out to be skimpy coverage akin to minimum wage laws?
In its 2024 budget document, the federal government proposed providing $1.5 billion over five years to support the launch of national pharmacare for “universal, single-payer coverage for a number of contraception and diabetes medications.” This has been hailed as a “big day for pharmacare” by some labour unions, patients and others, including the author of the BMJ article who said that national pharmacare should be expanded to cover all medication needs beginning with the most commonly-prescribed, clinically-important “essential medicines.”
In its budget, the government stated “coverage of contraceptives will mean that nine million women in Canada will have better access to contraception” and “improving access to diabetes medications will help improve the health of 3.7 million Canadians with diabetes.” Why not salute such affable, motherhood and apple pie, sentiments? The devil is in the details.
The plan does not cover new drugs for diabetes, such as Ozempic, Rybelsus, Wegovy, Mounjaro or Zepbound, all based on innovative GLP-1 agonists, where evidence is building for cardiovascular and weight loss benefits. This limited rollout seems based on cheap, older medicines, which can be less effective for some with diabetes.
The federal government has also consistently under-estimated the cost of national proposals such as pharmacare – not to mention other promises. In their 2019 election platform, the Liberals promised $6 billion for national pharmacare (the NDP promised $10 billion). Keen analysis shows that even these expansive amounts would be woefully inadequate to fund a full national pharmacare plan. This makes the $300 million a year actually proposed by the Liberals’ look like the skimpy window-dressing that it is.
National pharmacare, based on the most comprehensive existing public drug plan (Quebec’s), would cost much more. In 2017, using optimistic assumptions, the Parliamentary Budget Officer (PBO) estimated the cost for a national plan based on Quebec’s experience to be $19.3 billion a year. With more appropriate assumptions, the Canadian Health Policy Institute estimated $26.2 billion. In June 2019, the federal government’s own Advisory Council on the Implementation of National Pharmacare put the cost at $40 billion, while a few months later, the tax consulting company RSM Canada projected $48.3 to $52.5 billion per year. Five years later, costs no doubt have soared.
Even with these staggering cost a program based on matching Quebec’s drug plan at the national level would fail to provide anywhere near the level of coverage already provided to the almost two-thirds of Canadians who have private drug insurance, including many in unionized jobs. Are they willing to sacrifice their superior coverage, especially of innovative brand-name medicines, for a program covering only “essential medicines”? Put another way, are Canadians and their unions prepared to settle for the equivalent of a minimum wage or minimum benefits?
The PBO has estimated the cost of coverage of a range of contraceptives and diabetes medicines as $1.9 billion over five years, which is more than the $1.5 billion provided in the budget. However, this figure is based on an assumption that the new program would only cover Canadians who currently do not have public or private drug plan insurance, those who currently do not fill their prescriptions due to cost related reasons, and the out-of-pocket part of prescription costs for Canadians who have public or private drug plan coverage. This is major guesswork because existing public and private drug plans may see the new federal program as an opportunity to reduce their costs by requiring their beneficiaries to use the new program. If this occurs, the national pharmacare costs to the federal government, even for the limited role out of diabetes and contraceptives, would soar to an estimated $5.7 billion, according to the PBO.
Our governments are not known for accurate estimates of the costs of new programs. One has only to remember the Phoenix pay system and the ArriveCAN costs. In 2017, the Government of Ontario estimated $465 million per year to extend drug coverage to every resident under the age of 25 years. What happened? Introduced in 2018, prescriptions rose by 290% and drug expenditure increased to $839 million – almost double the guesstimate. In 2019, the provincial government back peddled and modified the program to cover only people not already insured by a private plan.
Although we believe governments should facilitate access to necessary medicines for Canadians who cannot afford their medicines, this does not require national pharmacare and a growing bureaucracy. Exempting lower-income Canadians from copayments and premiums required by provincial programs, as British Columbia has done, and removing the requirement to pay for all drugs up to a deductible would allow these Canadians access sooner, more simply, and more effectively.
Moreover, it isn’t just lower-income Canadians who want help with unmet medicine needs. Canadians who need access to drugs for diseases that are difficult to treat and can cost hundreds of thousands of dollars per year also require assistance. Few Canadians whether they have low, medium or high incomes can afford these prices without government or private insurance. Private insurers often refuse to cover these drugs.
The Liberals provided a separate $1.5 billion over three years for drugs for rare disorders, but no province or territory has signed a bilateral agreement with the federal government for these drugs and no patient has received benefit through this program. Even if they did, the $500 million per year would not go far towards the actual costs. There is at least a zero missing in the federal contribution, as the projected cost of public spending on rare disease medicines by 2025 is more than threefold what Ottawa has budgeted.
Expensive drugs for cancer and rare disorders are just as essential as basic medicines for cardiovascular diseases, diabetes, birth control, and many other common conditions. If a costly medicine will allow a person with a life-shortening disease to live longer or one with a disorder that will be severely disabling left untreated to have an improved quality of life and be a productive taxpayer, it too should be regarded as essential.
The Liberals and NDP are working to stampede the bill to introduce the pharmacare program (Bill C-64) through the legislative process. This includes inviting witnesses over the first long weekend of summer, when many Canadians are away, to appear before the parliamentary Standing Committee on Health three days later.
Too much is unknown about what will be covered (will newer drugs be covered or only older, cheaper medicines?), who will be eligible for coverage (all appropriate Canadians regardless of existing coverage or only those with no present coverage?), and what the real cost will be, including whether a new program focusing on older, cheaper drugs will deter drug developers from launching novel medicines for unmet needs in Canada.
This Bill as it stands is such a power grab that, if passed, the federal Health Minister never has to come back to Parliament for review, oversight or another tranche of legal authority, it would empower the Cabinet to make rules and regulations without parliamentary scrutiny.
A lot is at stake for Canadians, especially for patients and their doctors. Prescription medicines are of critical importance to treating many diseases. National pharmacare must not only allow low-income residents to access purported “essential medicines” but also ensure that patients who need specialized drugs, especially higher-cost innovative cell and genetic therapies that may be the only effective treatment for their disorder, are not ignored. Canadians should be careful what they wish for. They may receive less than they anticipate, and, in fact, many Canadians may be worse off despite the increase in public spending. Time to look under the hood and kick the tires.
Nigel Rawson is a senior fellow with the Macdonald-Laurier Institute.
John Adams is co-founder and CEO of Canadian PKU and Allied Disorders Inc., a senior fellow with the Macdonald-Laurier Institute and volunteer board chair of Best Medicines Coalition.

From LifeSiteNews
Pfizer and Moderna’s mRNA COVID shots must now include warnings that they cause ‘extremely high risk’ of heart inflammation and irreversible damage in males up to age 24.
The Trump administration’s Food and Drug Administration (FDA) announced it will now require updated safety warnings on mRNA COVID-19 shots to include the “extremely high risk” of myocarditis/pericarditis and the likelihood of long-term, irreversible heart damage for teen boys and young men up to age 24.
The required safety updates apply to Comirnaty, the mRNA COVID shot manufactured by Pfizer Inc., and Spikevax, the mRNA COVID shot manufactured ModernaTX, Inc.
According to a press release, the FDA now requires each of those manufacturers to update the warning about the risks of myocarditis and pericarditis to include information about:
- the estimated unadjusted incidence of myocarditis and/or pericarditis following administration of the 2023-2024 Formula of mRNA COVID-19 shots and
- the results of a study that collected information on cardiac magnetic resonance imaging (cardiac MRI) in people who developed myocarditis after receiving an mRNA COVID-19 injection.
The FDA has also required the manufacturers to describe the new safety information in the adverse reactions section of the prescribing information and in the information for recipients and caregivers.
Additionally, the fact sheets for healthcare providers and for recipients and caregivers for Moderna COVID-19 shot and Pfizer-BioNTech COVID-19 shot, which are authorized for emergency use in individuals 6 months through 11 years of age, have also been updated to include the new safety information in alignment with the Comirnaty and Spikevax prescribing information and information for recipients and caregivers.
In a video published on social media, Dr. Vinay Prasad, director of the Center for Biologics Evaluation & Research Chief Medical and Scientific Officer, explained the alarming reasons for the warning updates.
While heart problems arose in approximately 8 out of 1 million persons ages 6 months to 64 years following reception of the cited shots, that number more than triples to 27 per million for males ages 12 to 24.
Prasad noted that multiple studies have arrived at similar findings.

From LifeSiteNews
By Matt Lamb
They got rid of all the older children essentially and just had younger children who were too young to be diagnosed and they stratified that, stratified the data
The Centers for Disease Control and Prevention (CDC) found newborn babies who received the Hepatitis B vaccine had 1,135-percent higher autism rates than those who did not or received it later in life, Robert F. Kennedy Jr. told Tucker Carlson recently. However, the CDC practiced “trickery” in its studies on autism so as not to implicate vaccines, Kennedy said.
RFK Jr., who is the current Secretary of Health and Human Services, said the CDC buried the results by manipulating the data. Kennedy has pledged to find the causes of autism, with a particular focus on the role vaccines may play in the rise in rates in the past decades.
The Hepatitis B shot is required by nearly every state in the U.S. for children to attend school, day care, or both. The CDC recommends the jab for all babies at birth, regardless of whether their mother has Hep B, which is easily diagnosable and commonly spread through sexual activity, piercings, and tattoos.
“They kept the study secret and then they manipulated it through five different iterations to try to bury the link and we know how they did it – they got rid of all the older children essentially and just had younger children who were too young to be diagnosed and they stratified that, stratified the data,” Kennedy told Carlson for an episode of the commentator’s podcast. “And they did a lot of other tricks and all of those studies were the subject of those kind of that kind of trickery.”
But now, Kennedy said, the CDC will be conducting real and honest scientific research that follows the highest standards of evidence.
“We’re going to do real science,” Kennedy said. “We’re going to make the databases public for the first time.”
He said the CDC will be compiling records from variety of sources to allow researchers to do better studies on vaccines.
“We’re going to make this data available for independent scientists so everybody can look at it,” the HHS secretary said.
— Matt Lamb (@MattLamb22) July 1, 2025
Health and Human Services also said it has put out grant requests for scientists who want to study the issue further.
Kennedy reiterated that by September there will be some initial insights and further information will come within the next six months.
Carlson asked if the answers would “differ from status quo kind of thinking.”
“I think they will,” Kennedy said. He continued on to say that people “need to stop trusting the experts.”
“We were told at the beginning of COVID ‘don’t look at any data yourself, don’t do any investigation yourself, just trust the experts,”‘ he said.
In a democracy, Kennedy said, we have the “obligation” to “do our own research.”
“That’s the way it should be done,” Kennedy said.
He also reiterated that HHS will return to “gold standard science” and publish the results so everyone can review them.

RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued
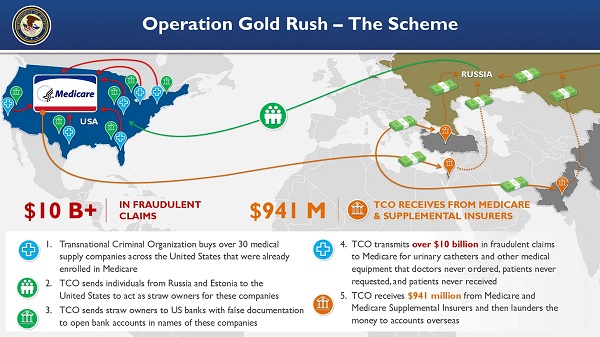
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump

-
Business2 days ago
RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate
-
 Business1 day ago
Business1 day agoWhy it’s time to repeal the oil tanker ban on B.C.’s north coast
-
 Alberta1 day ago
Alberta1 day agoAlberta Provincial Police – New chief of Independent Agency Police Service
-
 Energy1 day ago
Energy1 day agoIf Canada Wants to be the World’s Energy Partner, We Need to Act Like It
-
 Alberta1 day ago
Alberta1 day agoPierre Poilievre – Per Capita, Hardisty, Alberta Is the Most Important Little Town In Canada
-
 International2 days ago
International2 days agoCBS settles with Trump over doctored 60 Minutes Harris interview
-
 Aristotle Foundation2 days ago
Aristotle Foundation2 days agoHow Vimy Ridge Shaped Canada
-
 Alberta1 day ago
Alberta1 day agoAlberta uncorks new rules for liquor and cannabis