Opinion
Medicine Hat, population 63,260 has 5 pools and a man made swimming lake. Red Deer should do better.

The City of Medicine Hat recorded a population of 63,260 in 2016
The City of Medicine Hat has many options for residents and visitors for the community when it comes to swimming.
2 Indoor pools= Kinsmen Aquatic Park (FLC) and the Crestwood Pool (no 50m pools)
3 Outdoor pools= Strathcona Pool, Heights Pool and the Hill Pool
Medicine Hat has a swimming lake= Echo Dale
Echo Dale, the largest of Medicine Hat’s parks, is located a short distance west of Medicine Hat along the South Saskatchewan River. The park has two man-made lakes: one for swimming and one for paddle boating and fishing.
Echo Dale Regional Park is an oasis for people and wildlife and has more than 110,000 visitors each year. Patrons range from sun-loving swimmers to those who enjoy sitting around a fire at night, to the regulars who walk the trails each day throughout the year, no matter how bad the weather!
From the historic farm site on the west side of the park to the day use area on the far east side of the park and all the others areas in between, the pristine condition of Echo Dale Regional Park is a favorite. Claim your favorite spot around the Swim Lake or set up for a family picnic at the boat lake which is stocked with rainbow trout for those wanting to fish.
New playground equipment in the shape of a pirate ship sits on the beach at the swim lake and new playground equipment at the boat lake, all add up to summertime fun!
Red Deer has a greater opportunity in having a real natural lake. Will Red Deer build a park? NO, they will likely plan on houses, and apartment buildings that may never get built, unless we go into a boom portion of the boom-bust cycle. This is the simplistic, easiest and safest plan with a low return on investment. It ignores the high-profile location and possibilities of the lake, but it has less risk. A wall will be built to hide the lake from Hwy 2.
Remember, Hazlett Lake is a natural lake that covers a surface area of 0.45 km2 (0.17 mi2), has an average depth of 3 meters (10 feet). Hazlett Lake has a total shore line of 4 kilometers (2 miles). It is 108.8 acres in size. Located in the north-west sector of Red Deer.
So, please, the next time you drive north on Hwy 2, as you pass the Hwy 11A turnoff, look out the passenger window and check out Hazlett Lake.
That lake is part of the City of Red Deer, and is a portion of a Major Area Structure Plan north of Hwy 11A previously mentioned. So as you drive by, think of what you would like to see done with your lake.
One scenario that could compliment the lake and address the desire for a regional aquatic centre and a 50-metre pool is turning the proposed community centre on the northeast corner of the lake into a Collicutt Centre type of complex.
What is more natural than having an aquatic centre on the lake? You could have your 50-metre pool inside, a lake for scuba diving, kayaking, canoeing, paddle boating, swimming, under-water photography, fishing, sun tanning, races, to name but a few.
The winter could see skating, hockey, to complement the indoor ice rink, as well as ice-fishing and ice sculptures and sleigh rides, again, to name but a few. This would all be visible to the traffic on Hwy 2.
Would a regional aquatic centre built on Hazlett Lake kick-start development in Red Deer’s north at a time of a slowdown in the energy sector? Would a Hazlett Lake regional aquatic centre, visible from Hwy 2, create a tourism trade that would bolster Red Deer’s hospitality industry? Would a Hazlett Lake regional aquatic centre enhance our position as a sports destination? Would a Hazlett Lake regional aquatic centre ensure that everyone would have an opportunity to enjoy the lake? I hope so.
I think the Hazlett Lake is worth preserving, and I hope that when my grandchildren drive north on Hwy 2 just past the Hwy 11A turnoff, that they will be able to look out the passenger side window and see Hazlett Lake.
Perhaps they will be able to tan on a beach, watch a naturescape in action, paddle a canoe, swim, skate, maybe have a bonfire on a beach and roast a marshmallow. We do need to act now, before the plans get too entrenched in the least desired direction.
Please contact the city before it is too late.
Alberta
‘Far too serious for such uninformed, careless journalism’: Complaint filed against Globe and Mail article challenging Alberta’s gender surgery law
![]()
Macdonald Laurier Institute challenges Globe article on gender medicine
The complaint, now endorsed by 41 physicians, was filed in response to an article about Alberta’s law restricting gender surgery and hormones for minors.
On June 9, the Macdonald-Laurier Institute submitted a formal complaint to The Globe and Mail regarding its May 29 Morning Update by Danielle Groen, which reported on the Canadian Medical Association’s legal challenge to Alberta’s Bill 26.
Written by MLI Senior Fellow Mia Hughes and signed by 34 Canadian medical professionals at the time of submission to the Globe, the complaint stated that the Morning Update was misleading, ideologically slanted, and in violation the Globe’s own editorial standards of accuracy, fairness, and balance. It objected to the article’s repetition of discredited claims—that puberty blockers are reversible, that they “buy time to think,” and that denying access could lead to suicide—all assertions that have been thoroughly debunked in recent years.
Given the article’s reliance on the World Professional Association for Transgender Health (WPATH), the complaint detailed the collapse of WPATH’s credibility, citing unsealed discovery documents from an Alabama court case and the Cass Review’s conclusion that WPATH’s guidelines—and those based on them—lack developmental rigour. It also noted the newsletter’s failure to mention the growing international shift away from paediatric medical transition in countries such as the UK, Sweden, and Finland. MLI called for the article to be corrected and urged the Globe to uphold its commitment to balanced, evidence-based journalism on this critical issue.
On June 18, Globe and Mail Standards Editor Sandra Martin responded, defending the article as a brief summary that provided a variety of links to offer further context. However, the three Globe and Mail news stories linked to in the article likewise lacked the necessary balance and context. Martin also pointed to a Canadian Paediatric Society (CPS) statement linked to in the newsletter. She argued it provided “sufficient context and qualification”—despite the fact that the CPS itself relies on WPATH’s discredited guidelines. Notwithstanding, Martin claimed the article met editorial standards and that brevity justified the lack of balance.
MLI responded that brevity does not excuse misinformation, particularly on a matter as serious as paediatric medical care, and reiterated the need for the Globe to address the scientific inaccuracies directly. MLI again called for the article to be corrected and for the unsupported suicide claim to be removed. As of this writing, the Globe has not responded.
Letter of complaint
June 9, 2025
To: The Globe and Mail
Attn: Sandra Martin, standards editor
CC: Caroline Alphonso, health editor; Mark Iype, deputy national editor and Alberta bureau chief
To the editors;
Your May 29 Morning Update: The Politics of Care by Danielle Groen, covering the Canadian Medical Association’s legal challenge to Alberta’s Bill 26, was misleading and ideologically slanted. It is journalistically irresponsible to report on contested medical claims as undisputed fact.
This issue is far too serious for such uninformed, careless journalism lacking vital perspectives and scientific context. At stake is the health and future of vulnerable children, and your reporting risks misleading parents into consenting to irreversible interventions based on misinformation.
According to The Globe and Mail’s own Journalistic Principles outlined in its Editorial Code of Conduct, the credibility of your reporting rests on “solid research, clear, intelligent writing, and maintaining a reputation for honesty, accuracy, fairness, balance and transparency.” Moreover, your principles go on to state that The Globe will “seek to provide reasonable accounts of competing views in any controversy.” The May 29 update violated these principles. There is, as I will show, a widely available body of scientific information that directly contests the claims and perspectives presented in your article. Yet this information is completely absent from your reporting.
The collapse of WPATH’s credibility
The article’s claim that Alberta’s law “falls well outside established medical practice” and could pose the “greatest threat” to transgender youth is both false and inflammatory. There is no global medical consensus on how to treat gender-distressed young people. In fact, in North America, guidelines are based on the Standards of Care developed by the World Professional Association for Transgender Health (WPATH)—an organization now indisputably shown to place ideology above evidence.
{kind=link}
For example, in a U.S. legal case over Alabama’s youth transition ban, WPATH was forced to disclose over two million internal emails. These revealed the organization commissioned independent evidence reviews for its latest Standards of Care (SOC8)—then suppressed those reviews when they found overwhelmingly low-quality evidence. Yet WPATH proceeded to publish the SOC8 as if it were evidence-based. This is not science. It is fraudulent and unethical conduct.
These emails also showed Admiral Rachel Levine—then-assistant secretary for Health in the Biden administration—pressured WPATH to remove all lower age recommendations from the guidelines—not on scientific grounds, but to avoid undermining ongoing legal cases at the state level. This is politics, not sound medical practice.
The U.K.’s Cass Review, a major multi-year investigation, included a systematic review of the guidelines in gender medicine. A systematic review is considered the gold standard because it assesses and synthesizes all the available research in a field, thereby reducing bias and providing a large comprehensive set of data upon which to reach findings. The systematic review of gender medicine guidelines concluded that WPATH’s standards of care “lack developmental rigour” and should not be used as a basis for clinical practice. The Cass Review also exposed citation laundering where medical associations endlessly recycled weak evidence across interlocking guidelines to fabricate a false consensus. This led Cass to suggest that “the circularity of this approach may explain why there has been an apparent consensus on key areas of practice despite the evidence being poor.”
Countries like Sweden, Finland, and the U.K. have now abandoned WPATH and limited or halted medicalized youth transitions in favour of a therapy-first approach. In Norway, UKOM, an independent government health agency, has made similar recommendations. This shows the direction of global practice is moving away from WPATH’s medicalized approach—not toward it. As part of any serious effort to “provide reasonable accounts of competing views,” your reporting should acknowledge these developments.
Any journalist who cites WPATH as a credible authority on paediatric gender medicine—especially in the absence of contextualizing or competing views—signals a lack of due diligence and a fundamental misunderstanding of the field. It demonstrates that either no independent research was undertaken, or it was ignored despite your editorial standards.
Puberty blockers don’t ‘buy time’ and are not reversible
Your article repeats a widely debunked claim: that puberty blockers are a harmless pause to allow young people time to explore their identity. In fact, studies have consistently shown that between 98 per cent and 100 per cent of children placed on puberty blockers go on to take cross-sex hormones. Before puberty blockers, most children desisted and reconciled with their birth sex during or after puberty. Now, virtually none do.
This strongly suggests that blocking puberty in fact prevents the natural resolution of gender distress. Therefore, the most accurate and up-to-date understanding is that puberty blockers function not as a pause, but as the first step in a treatment continuum involving irreversible cross-sex hormones. Indeed, a 2022 paper found that while puberty suppression had been “justified by claims that it was reversible … these claims are increasingly implausible.” Again, adherence to the Globe’s own editorial guidelines would require, at minimum, the acknowledgement of the above findings alongside the claims your May 29 article makes.
Moreover, it is categorically false to describe puberty blockers as “completely reversible.” Besides locking youth into a pathway of further medicalization, puberty blockers pose serious physical risks: loss of bone density, impaired sexual development, stunted fertility, and psychosocial harm from being developmentally out of sync with peers. There are no long-term safety studies. These drugs are being prescribed to children despite glaring gaps in our understanding of their long-term effects.
Given the Globe’s stated editorial commitment to principles such as “accuracy,” the crucial information from the studies linked above should be provided in any article discussing puberty blockers. At a bare minimum, in adherence to the Globe’s commitment to “balance,” this information should be included alongside the contentious and disputed claims the article makes that these treatments are reversible.
No proof of suicide prevention
The most irresponsible and dangerous claim in your article is that denying access to puberty blockers could lead to “depression, self-harm and suicide.” There is no robust evidence supporting this transition-or-suicide narrative, and in fact, the findings of the highest-quality study conducted to date found no evidence that puberty suppression reduces suicide risk.
Suicide is complex and attributing it to a single cause is not only false—it violates all established suicide reporting guidelines. Sensationalized claims like this risk creating contagion effects and fuelling panic. In the public interest, reporting on the topic of suicide must be held to the most rigorous standards, and provide the most high-quality and accurate information.
Euphemism hides medical harm
Your use of euphemistic language obscures the extreme nature of the medical interventions being performed in gender clinics. Calling double mastectomies for teenage girls “paediatric breast surgeries for gender-affirming reasons” sanitizes the medically unnecessary removal of a child’s healthy organs. Referring to phalloplasty and vaginoplasty as “gender-affirming surgeries on lower body parts” conceals the fact that these are extreme operations involving permanent disfigurement, high complication rates, and often requiring multiple revisions.
Honest journalism should not hide these facts behind comforting language. Your reporting denies youth, their parents, and the general public the necessary information to understand the nature of these interventions. Members of the general public rely greatly on the news media to equip them with such information, and your own editorial standards claim you will fulfill this core responsibility.
Your responsibility to the public
As a flagship Canadian news outlet, your responsibility is not to amplify activist messaging, but to report the truth with integrity. On a subject as medically and ethically fraught as paediatric gender medicine, accuracy is not optional. The public depends on you to scrutinize claims, not echo ideology. Parents may make irreversible decisions on behalf of their children based on the narratives you promote. When reporting is false or ideologically distorted, the cost is measured in real-world harm to some of our society’s most vulnerable young people.
I encourage the Globe and Mail to publish an updated version on this article in order to correct the public record with the relevant information discussed above, and to modify your reporting practices on this matter going forward—by meeting your own journalistic standards—so that the public receives balanced, correct, and reliable information on this vital topic.
Trustworthy journalism is a cornerstone of public health—and on the issue of paediatric gender medicine, the stakes could not be higher.
Sincerely,
Mia Hughes
Senior Fellow, Macdonald-Laurier Institute
Author of The WPATH Files
The following 41 physicians have signed to endorse this letter:
Dr. Mike Ackermann, MD
Dr. Duncan Veasey, Psy MD
Dr. Rick Gibson, MD
Dr. Benjamin Turner, MD, FRCSC
Dr. J.N. Mahy, MD, FRCSC, FACS
Dr. Khai T. Phan, MD, CCFP
Dr. Martha Fulford, MD
Dr. J. Edward Les, MD, FRCPC
Dr. Darrell Palmer, MD, FRCPC
Dr. Jane Cassie, MD, FRCPC
Dr. David Lowen, MD, FCFP
Dr. Shawn Whatley, MD, FCFP (EM)
Dr. David Zitner, MD
Dr. Leonora Regenstreif, MD, CCFP(AM), FCFP
Dr. Gregory Chan, MD
Dr. Alanna Fitzpatrick, MD, FRCSC
Dr. Chris Millburn, MD, CCFP
Dr. Julie Curwin, MD, FRCPC
Dr. Roy Eappen, MD, MDCM, FRCP (c)
Dr. York N. Hsiang, MD, FRCSC
Dr. Dion Davidson, MD, FRCSC, FACS
Dr. Kevin Sclater, MD, CCFP (PC)
Dr. Theresa Szezepaniak, MB, ChB, DRCOG
Dr. Sofia Bayfield, MD, CCFP
Dr. Elizabeth Henry, MD, CCFP
Dr. Stephen Malthouse, MD
Dr. Darrell Hamm, MD, CCFP
Dr. Dale Classen, MD, FRCSC
Dr. Adam T. Gorner, MD, CCFP
Dr. Wesley B. Steed, MD
Dr. Timothy Ehmann, MD, FRCPC
Dr. Ryan Torrie, MD
Dr. Zachary Heinricks, MD, CCFP
Dr. Jessica Shintani, MD, CCFP
Dr. Mark D’Souza, MD, CCFP(EM), FCFP*
Dr. Joanne Sinai, MD, FRCPC*
Dr. Jane Batt, MD*
Dr. Brent McGrath, MD, FRCPC*
Dr. Leslie MacMillan MD FRCPC (emeritus)*
Dr. Ian Mitchell, MD, FRCPC*
Dr. John Cunnington, MD
*Indicates physician who signed following the letter’s June 9 submission to the Globe and Mail, but in advance of this letter being published on the MLI website.

From the Fraser Institute
Two recent events exemplify the fundamental irrationality that is Canada’s electric vehicle (EV) policy.
First, the Carney government re-committed to Justin Trudeau’s EV transition mandate that by 2035 all (that’s 100 per cent) of new car sales in Canada consist of “zero emission vehicles” including battery EVs, plug-in hybrid EVs and fuel-cell powered vehicles (which are virtually non-existent in today’s market). This policy has been a foolish idea since inception. The mass of car-buyers in Canada showed little desire to buy them in 2022, when the government announced the plan, and they still don’t want them.
Second, President Trump’s “Big Beautiful” budget bill has slashed taxpayer subsidies for buying new and used EVs, ended federal support for EV charging stations, and limited the ability of states to use fuel standards to force EVs onto the sales lot. Of course, Canada should not craft policy to simply match U.S. policy, but in light of policy changes south of the border Canadian policymakers would be wise to give their own EV policies a rethink.
And in this case, a rethink—that is, scrapping Ottawa’s mandate—would only benefit most Canadians. Indeed, most Canadians disapprove of the mandate; most do not want to buy EVs; most can’t afford to buy EVs (which are more expensive than traditional internal combustion vehicles and more expensive to insure and repair); and if they do manage to swing the cost of an EV, most will likely find it difficult to find public charging stations.
Also, consider this. Globally, the mining sector likely lacks the ability to keep up with the supply of metals needed to produce EVs and satisfy government mandates like we have in Canada, potentially further driving up production costs and ultimately sticker prices.
Finally, if you’re worried about losing the climate and environmental benefits of an EV transition, you should, well, not worry that much. The benefits of vehicle electrification for climate/environmental risk reduction have been oversold. In some circumstances EVs can help reduce GHG emissions—in others, they can make them worse. It depends on the fuel used to generate electricity used to charge them. And EVs have environmental negatives of their own—their fancy tires cause a lot of fine particulate pollution, one of the more harmful types of air pollution that can affect our health. And when they burst into flames (which they do with disturbing regularity) they spew toxic metals and plastics into the air with abandon.
So, to sum up in point form. Prime Minister Carney’s government has re-upped its commitment to the Trudeau-era 2035 EV mandate even while Canadians have shown for years that most don’t want to buy them. EVs don’t provide meaningful environmental benefits. They represent the worst of public policy (picking winning or losing technologies in mass markets). They are unjust (tax-robbing people who can’t afford them to subsidize those who can). And taxpayer-funded “investments” in EVs and EV-battery technology will likely be wasted in light of the diminishing U.S. market for Canadian EV tech.
If ever there was a policy so justifiably axed on its failed merits, it’s Ottawa’s EV mandate. Hopefully, the pragmatists we’ve heard much about since Carney’s election victory will acknowledge EV reality.

Kenneth P. Green
Senior Fellow, Fraser Institute



RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
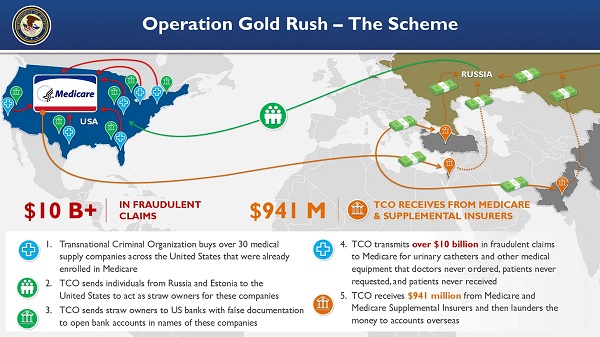
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Crime2 days ago
Crime2 days agoEyebrows Raise as Karoline Leavitt Answers Tough Questions About Epstein
-
 Alberta2 days ago
Alberta2 days agoCOWBOY UP! Pierre Poilievre Promises to Fight for Oil and Gas, a Stronger Military and the Interests of Western Canada
-
 Alberta2 days ago
Alberta2 days agoAlberta and Ontario sign agreements to drive oil and gas pipelines, energy corridors, and repeal investment blocking federal policies
-
 Crime1 day ago
Crime1 day ago“This is a total fucking disaster”
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Fraser Institute1 day ago
Fraser Institute1 day agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
 Daily Caller2 days ago
Daily Caller2 days agoBlackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
 MAiD1 day ago
MAiD1 day agoCanada’s euthanasia regime is already killing the disabled. It’s about to get worse