Health
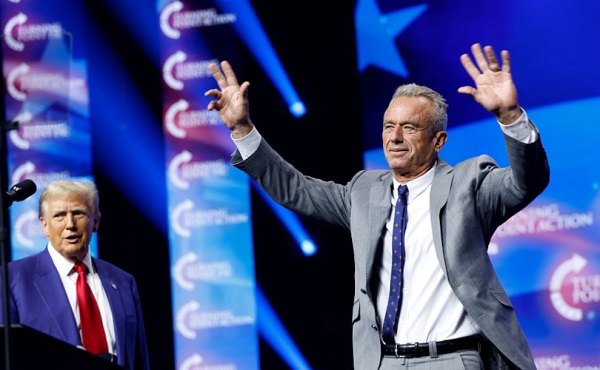
How the Trump-RFK Jr. coalition could realign US politics against Big Pharma and Big Food


From LifeSiteNews
By Jay Richards
If the unlikely coalition of Donald Trump and Robert F. Kennedy Jr. outlives the 2024 presidential election, it could reorder our political categories and leave to our children and grandchildren a quite different future.
When Robert F. Kennedy, Jr. endorsed Donald Trump on Aug. 23, the corporate press and conventional Washington, D.C., analysts mostly missed the real story: It was the moment that a disparate, diverse, and potentially disruptive throng of average Americans became a coalition.
Although RFK, Jr. is famous – or infamous, depending on your view – for his criticisms of vaccines, that wasn’t the theme of his lengthy speech. He spoke instead about an unholy alliance – a cartel – of industries, corporate media, government regulatory agencies, and even nonprofit “charities” that is making us fat and sick. This problem doesn’t fit the simple taxonomy of “public” and “private” or “left” and “right” that served us well during the Cold War.
Kennedy has been a voice in the wilderness warning about this cartel for years. Most Americans first became aware of it during the 2020 pandemic. Here’s the basic story: COVID-19 itself was likely the product of dangerous gain-of-function research conducted by the Wuhan Institute of Virology in China. That’s bad enough. But Communist China didn’t act alone. This work was funded, at least in part, by the U.S. government’s National Institutes of Health and laundered through the nonprofit EcoHealth Alliance.
Once the virus was out, the absurd and counterproductive lockdowns and hygiene theater were pushed by global entities such as the World Health Organization. Domestically, Francis Collins, then-head of the NIH, and Anthony Fauci, then-head of the National Institute of Allergy and Infectious Diseases, worked to undermine independent experts who criticized the federal bureaucrats’ favored policies.
Collins and Fauci even orchestrated the publication of a deceptive article in Nature that claimed the virus had a natural origin. The Centers for Disease Control and Prevention and other federal entities, including the Biden White House, pressured social media platforms to censor even the best-credentialed dissenters.
Attentive Americans soon learned that public health, as a field, focuses on nudging whole populations, rather than seeking the health of individual patients.
Certain pharmaceutical companies – which pay royalties to many NIH staff, including Collins and Fauci – enjoyed a suspiciously fast and less than rigorous approval process for their mRNA “vaccines.” Vaccine mandates then created a massive artificial market for the drugs. And drug companies’ immunity from legal liability allowed them to enjoy the financial benefits of these policies without facing the downside risks from any long-term harm to those who took the vaccines.
Then, during the lockdowns, the growing awareness of the “gender-industrial complex” – media, medical professionals, pharmaceutical companies, politicians, and others who push ghoulish “gender-affirming” interventions on people distressed about their sexed bodies – further reinforced the lack of credibility of private and public health authorities.
An American epidemic of chronic diseases
For some, much of this may now seem obvious. What may be less obvious is that blame for the massive spike in many chronic “diseases of civilization” should go to the same cartel. It involves Big Government, Big Food, Big Pharma, Big Media that rely on pharmaceutical industry ad dollars, and medical lobbying outfits such as the American Academy of Pediatrics pretending to be sound science crusaders.
In his speech, Kennedy devoted many paragraphs to the “chronic disease epidemic” – including ever higher rates, even among children, of Type II diabetes and obesity, and of Alzheimer’s, which some now refer to as “Type III diabetes.” He spoke of “the insidious corruption at the FDA and the NIH, the HHS and the USDA that has caused the epidemic,” referring to the Food and Drug Administration, the Department of Health and Human Services, and the U.S. Department of Agriculture, along with the NIH.
But he didn’t stop there. He spoke of “an explosion of neurological illnesses that I never saw as a kid,” including:
ADD, ADHD, speech delay, language delay, Tourette’s Syndrome, narcolepsy, ASD, Asperger’s, autism. In the year 2000, the Autism rate was one in 1500. Now, autism rates in kids are one in 36, according to CDC; nationally, nobody’s talking about this.
He also spoke of the massive spikes in the use of antidepressants and anti-anxiety drugs. Of course, first ladies and surgeons general have launched “healthy lifestyle” campaigns, but these always parrot the conventional wisdom of the cartel. In contrast, Kennedy blamed the cartel itself, not a gluttonous public, for the chronic disease crisis. It was this cartel that gave us the war on healthy dietary fats and the ridiculous food pyramid – heavy on unhealthy ultrarefined carbohydrates and light on fat – which helped make Americans far fatter and sicker than we were before.
His speech hit a nerve, especially among parents who recognize this problem but lack a credible and effective way to fight it. They may engage in private acts of defiance – refusing the COVID-19 or Hepatitis B vaccines for their young children, or disregarding USDA warnings about the consumption of animal fat. So far, however, neither political party has taken up this topic. The Left has tended to give the administrative state the benefit of the doubt. The Right has tended to do the same for corporations.
Trump has promised that Kennedy will have a leading role in fighting America’s health crisis. That will mean taking on the cartel. But the devil is in the details. A sustained effort to “make America healthy again,” or MAHA – to complement MAGA – must be free of government interests on the one hand and industry funding and lobbyists on the other.
Maybe that’s impossible, but Kennedy as MAHA czar could mean a serious exploration of the role the cartel has played in the following:
- Restricting medical freedom
- The origin of the COVID-19 virus
- The effects of the pandemic lockdowns
- The lack of safety and effectiveness of mRNA vaccines
- The rise in childhood and adult obesity
- The rise in childhood and adult Type II diabetes
- The rise in Alzheimer’s
- The rise in allergies, food sensitivities, and asthma
- Rising rates of depression and anxiety disorders
- Rising rates of neurological disorders such as autism
- The explosion of cases of childhood gender dysphoria
- The collusion between the World Professional Association of Transgender Health and HHS officials such as transgender activist and Assistant Secretary for Health Rachel Levine
- The political agenda of transnational public health bureaucracies such as the World Health Organization
- The medicalization of the treatment for gender dysphoria with “gender-affirming care” (rather than taking a mental health approach)
- The capitulation of NIH, CDC, FDA, and HHS to gender ideology over sound science
- The lack of value and safety of the ever-growing childhood vaccine schedule
- The medical focus on symptoms rather than underlying causes and cures of diseases
- The artificial restriction of medical and therapeutic credentialing of professionals to control supply and competition
- The decline in average testosterone in males
- The rise in infertility
- The rise in opioid addiction and overdose deaths
- Unethical research sponsored by the NIH
- The incompetence of the USDA in dispensing nutrition advice
- The effect of agricultural subsidies on our health
- Environmentalist dogmas masquerading as health and nutrition advice
If Trump appoints Kennedy as the MAHA czar, it would be akin to his COVID-19 Operation Warp Speed during his first administration but without the industry taint.
Of course, that appointment could come to nothing – except that there is already a coalition forming of millions of parents across, and even orthogonal to, the political spectrum, who – as Kennedy has put it – love their children more than they hate each other. It would take both the political will in Washington and a popular constituency of average Americans to fight the biomedical security state and the cartel that fuels it.
We’re getting a glimpse of this motley resistance in the unlikely unity ticket of Trump and Kennedy and the many strange bedfellows supporting them. If this coalition outlives the 2024 presidential election, it could reorder our political categories and leave to our children and grandchildren a quite different future.

From LifeSiteNews
Research found that men who underwent a ‘gender transition’ using hormones have a 51% higher mortality rate than the general population and a ‘threefold’ greater risk of cardiovascular deaths.
A newly published study has found that males’ use of estrogen to present as “female” triples their risk of cardiovascular disease, while also heightening the risk of stroke, blood clots, depression, and cognitive impairment.
The journal Discover Mental Health on June 12 released a variety of findings regarding the negative impacts of estrogen use in males attempting to transition to “female.” One of the most significant was that current estrogen use “was associated with a threefold increased risk of death from cardiovascular events.”
In fact, a study of 966 “female transitioned” males were found to have a mortality rate 51 percent higher than that of the general population. Their main causes of death included cardiovascular disease (21 percent), cancer (32 percent), suicide (7.5 percent), and infection-related disease (five percent).
Estrogen use by males amplified other cardiovascular risks, especially with prolonged use. One meta-analysis found a 30 percent higher rate of stroke among gender-confused men who took estrogen compared with men who did not.
A review also found “strong evidence” that estrogen use by men increases their risk for vein blood clots “over fivefold.”
Estrogen use was also found to have a detrimental cognitive impact on men. For example, so-called “female transitioned” males were found to have lower scores than both their other male counterparts and women in “information-processing speed and episodic memory.”
In addition, elevated symptoms of depression were “associated with increased serum levels of estradiol” for men under the age of 60.
This recent study confirms 2023 study that found that all gender-confused individuals, whether men attempting to present themselves as women or women attempting to present themselves as men, were at significantly increased risk for a range of deadly cardiovascular conditions, including strokes, heart attacks, high blood pressure, and elevated cholesterol levels.
A 2019 study published by the National Institutes of Health (NIH) National Library of Medicine also found:
Cardiovascular disease (CVD) is the leading disease-specific cause of death for [so-called] transgender people undergoing [transgender procedures], with only suicide claiming more lives as the leader of all cause mortality.
However, for [gender-confused males], the risk of death from CVD is 3-fold higher than for all other groups.
Research reported by both the British Heart Association and the American Heart Association that same year arrived at similar findings:
“We already know sex hormones are important to cardiovascular health, and now we have people being exposed to high levels of sex hormones they normally would not have, which could be associated with cardiovascular benefit or risk,” said Dr. Christian Delles, a professor at the Institute of Cardiovascular and Medical Sciences at the University of Glasgow.

From the Brownstone Institute
The US Food and Drug Administration (FDA) has approved hundreds of drugs without proof that they work—and in some cases, despite evidence that they cause harm.
That’s the finding of a blistering two-year investigation by medical journalists Jeanne Lenzer and Shannon Brownlee, published by The Lever.
Reviewing more than 400 drug approvals between 2013 and 2022, the authors found the agency repeatedly ignored its own scientific standards.
One expert put it bluntly—the FDA’s threshold for evidence “can’t go any lower because it’s already in the dirt.”
A System Built on Weak Evidence
The findings were damning—73% of drugs approved by the FDA during the study period failed to meet all four basic criteria for demonstrating “substantial evidence” of effectiveness.
Those four criteria—presence of a control group, replication in two well-conducted trials, blinding of participants and investigators, and the use of clinical endpoints like symptom relief or extended survival—are supposed to be the bedrock of drug evaluation.
Yet only 28% of drugs met all four criteria—40 drugs met none.
These aren’t obscure technicalities—they are the most basic safeguards to protect patients from ineffective or dangerous treatments.
But under political and industry pressure, the FDA has increasingly abandoned them in favour of speed and so-called “regulatory flexibility.”
Since the early 1990s, the agency has relied heavily on expedited pathways that fast-track drugs to market.
In theory, this balances urgency with scientific rigour. In practice, it has flipped the process. Companies can now get drugs approved before proving that they work, with the promise of follow-up trials later.
But, as Lenzer and Brownlee revealed, “Nearly half of the required follow-up studies are never completed—and those that are often fail to show the drugs work, even while they remain on the market.”
“This represents a seismic shift in FDA regulation that has been quietly accomplished with virtually no awareness by doctors or the public,” they added.
More than half the approvals examined relied on preliminary data—not solid evidence that patients lived longer, felt better, or functioned more effectively.
And even when follow-up studies are conducted, many rely on the same flawed surrogate measures rather than hard clinical outcomes.
The result: a regulatory system where the FDA no longer acts as a gatekeeper—but as a passive observer.
Cancer Drugs: High Stakes, Low Standards
Nowhere is this failure more visible than in oncology.
Only 3 out of 123 cancer drugs approved between 2013 and 2022 met all four of the FDA’s basic scientific standards.
Most—81%—were approved based on surrogate endpoints like tumour shrinkage, without any evidence that they improved survival or quality of life.
Take Copiktra, for example—a drug approved in 2018 for blood cancers. The FDA gave it the green light based on improved “progression-free survival,” a measure of how long a tumour stays stable.
But a review of post-marketing data showed that patients taking Copiktra died 11 months earlier than those on a comparator drug.
It took six years after those studies showed the drug reduced patients’ survival for the FDA to warn the public that Copiktra should not be used as a first- or second-line treatment for certain types of leukaemia and lymphoma, citing “an increased risk of treatment-related mortality.”
Elmiron: Ineffective, Dangerous—And Still on the Market
Another striking case is Elmiron, approved in 1996 for interstitial cystitis—a painful bladder condition.
The FDA authorized it based on “close to zero data,” on the condition that the company conduct a follow-up study to determine whether it actually worked.
That study wasn’t completed for 18 years—and when it was, it showed Elmiron was no better than placebo.
In the meantime, hundreds of patients suffered vision loss or blindness. Others were hospitalized with colitis. Some died.
Yet Elmiron is still on the market today. Doctors continue to prescribe it.
“Hundreds of thousands of patients have been exposed to the drug, and the American Urological Association lists it as the only FDA-approved medication for interstitial cystitis,” Lenzer and Brownlee reported.
“Dangling Approvals” and Regulatory Paralysis
The FDA even has a term—”dangling approvals”—for drugs that remain on the market despite failed or missing follow-up trials.
One notorious case is Avastin, approved in 2008 for metastatic breast cancer.
It was fast-tracked, again, based on ‘progression-free survival.’ But after five clinical trials showed no improvement in overall survival—and raised serious safety concerns—the FDA moved to revoke its approval for metastatic breast cancer.
The backlash was intense.
Drug companies and patient advocacy groups launched a campaign to keep Avastin on the market. FDA staff received violent threats. Police were posted outside the agency’s building.
The fallout was so severe that for more than two decades afterwards, the FDA did not initiate another involuntary drug withdrawal in the face of industry opposition.
Billions Wasted, Thousands Harmed
Between 2018 and 2021, US taxpayers—through Medicare and Medicaid—paid $18 billion for drugs approved under the condition that follow-up studies would be conducted. Many never were.
The cost in lives is even higher.
A 2015 study found that 86% of cancer drugs approved between 2008 and 2012 based on surrogate outcomes showed no evidence that they helped patients live longer.
An estimated 128,000 Americans die each year from the effects of properly prescribed medications—excluding opioid overdoses. That’s more than all deaths from illegal drugs combined.
A 2024 analysis by Danish physician Peter Gøtzsche found that adverse effects from prescription medicines now rank among the top three causes of death globally.
Doctors Misled by the Drug Labels
Despite the scale of the problem, most patients—and most doctors—have no idea.
A 2016 survey published in JAMA asked practising physicians a simple question—what does FDA approval actually mean?
Only 6% got it right.
The rest assumed that it meant the drug had shown clear, clinically meaningful benefits—such as helping patients live longer or feel better—and that the data was statistically sound.
But the FDA requires none of that.
Drugs can be approved based on a single small study, a surrogate endpoint, or marginal statistical findings. Labels are often based on limited data, yet many doctors take them at face value.
Harvard researcher Aaron Kesselheim, who led the survey, said the results were “disappointing, but not entirely surprising,” noting that few doctors are taught about how the FDA’s regulatory process actually works.
Instead, physicians often rely on labels, marketing, or assumptions—believing that if the FDA has authorized a drug, it must be both safe and effective.
But as The Lever investigation shows, that is not a safe assumption.
And without that knowledge, even well-meaning physicians may prescribe drugs that do little good—and cause real harm.
Who Is the FDA Working for?
In interviews with more than 100 experts, patients, and former regulators, Lenzer and Brownlee found widespread concern that the FDA has lost its way.
Many pointed to the agency’s dependence on industry money. A BMJ investigation in 2022 found that user fees now fund two-thirds of the FDA’s drug review budget—raising serious questions about independence.

Yale physician and regulatory expert Reshma Ramachandran said the system is in urgent need of reform.
“We need an agency that’s independent from the industry it regulates and that uses high-quality science to assess the safety and efficacy of new drugs,” she told The Lever. “Without that, we might as well go back to the days of snake oil and patent medicines.”
For now, patients remain unwitting participants in a vast, unspoken experiment—taking drugs that may never have been properly tested, trusting a regulator that too often fails to protect them.
And as Lenzer and Brownlee conclude, that trust is increasingly misplaced.
- Investigative report by Jeanne Lenzer and Shannon Brownlee at The Lever [link]
- Searchable public drug approval database [link]
- See my talk: Failure of Drug Regulation: Declining standards and institutional corruption
Republished from the author’s Substack
Author



What Connor Should Say To Oilers: It’s Not You. It’s Me.

The Passage of Bill C-5 Leaves the Conventional Energy Sector With as Many Questions as Answers

Ontario man launches new challenge against province’s latest attempt to ban free expression on roadside billboards

Federal fiscal anchor gives appearance of prudence, fails to back it up
-
COVID-198 hours ago
Ontario man launches new challenge against province’s latest attempt to ban free expression on roadside billboards
-
 Business1 day ago
Business1 day agoWhile China Hacks Canada, B.C. Sends Them a Billion-Dollar Ship Building Contract
-
 Energy16 hours ago
Energy16 hours agoThis Canada Day, Celebrate Energy Renewal
-
 Alberta1 day ago
Alberta1 day agoSo Alberta, what’s next?
-
 Alberta7 hours ago
Alberta7 hours agoAlberta Next Takes A Look At Alberta Provincial Police Force
-
 Bjorn Lomborg1 day ago
Bjorn Lomborg1 day agoThe Physics Behind The Spanish Blackout
-
 International10 hours ago
International10 hours agoPresident Xi Skips Key Summit, Adding Fuel to Ebbing Power Theories
-
 Alberta9 hours ago
Alberta9 hours agoCanadian Oil Sands Production Expected to Reach All-time Highs this Year Despite Lower Oil Prices