COVID-19
You don’t have to be afraid but you have to stay at home – From the front line in Italy

Dr. Daniele Maccini is a doctor on the front line of Italy’s fight against coronavirus
This is from his Facebook post from late February which is just as COVID-19 began to devastate Italy’s health care system. It has been translated from Italian.
Good morning everyone. For various reasons it’s been a lot since I posted on Facebook. But today I think it is useful to spend a page to share and ask you to share the words of a fellow common sense reanimator who in my opinion has been able to summarize a message that I would like to be transposed by everyone, regarding what is happening about the epidemic from Coronavirus Covid 19.
Therefore I quote:
” Coronavirus: we explain why you don’t have to be afraid but you have to stay at home.
I’m a CPR doctor and this is why I allow myself to explain why the State is making such drastic decisions.
The problem with Coronavirus is not its gravity, since it is only 10, or maybe 20 times more serious than the flu. Why is it more serious than flu?
It’s different, so we’re not very used to it;
Elders are not vaccinated.
So who is more at risk? The elders. As usual. Children much less, no serious paediatric cases are reported for the time being.
So why do we worry so much? Because it is MUCH MORE INFECTIVE than the flu, that means it is transmitted with enormous ease.
At this point let’s do some calculations so we can better understand what the problem is.
The Influence
As a rule, flu hits over a season, let’s assume in 5 months, about 10 % of the population. So it hits around 5 million Italians in the span of 30*5 = 150 days. Mortality is 0,1 %, so we have about 5000 deaths (almost all elderly) every year in 150 days. For each dead, we suppose we have about 4-5 patients in CPR, to keep us wide, and everyone should be put into ICU. We then put 25.000 people in ICU in 150 days, with an average inpatient of 7 days, which means 1000-2000 patients a day in ICU in Italy during the winter.
Let’s summarize:
Infectivity: 10 % potential (real data) = 50 million * 10 % = 5 million infected, many of them unaware.
Mortality: 0,1 % estimated = 5000 people in 150 days.
Critics: 5*0,1 % = 25.000 people in 150 days. so about 1000-2000 people in ICU a day due to flu.
The beds in ICU are for the province of Venice, where I live, about 60 out of 1 million inhabitants, so it could be about 4000 across Italy. This means that at worst case scenario patients with flu and its complications, i.e. pneumonia, occupy between 25 % and 50 % at maximum intensive therapies in Italy at peak.
The Coronavirus
Let’s see now what can happen with the Coronavirus. Let’s remember that the big difference is that Coronavirus is extremely more infectious and could infect us, instead of in 150 days, in 30-60 days. Suppose 60 days. Let’s remember that it can affect up to 60 % of the population, estimated data, so let’s do some calculations:
Infectivity: 60 % potential (estimated data) = 50 million * 60 % = 30 million infected, of which the vast majority unaware.
mortality: 1-2 % estimated = between 500.000 and 1.000.000 million people.
Critics: 5 % = 1.500.000 people in 60 days. so about 300.000 people in ICU.
But we only have 4000 beds! How can we put 300.000 people in ICU when we only have 4000 beds?
NOW YOU UNDERSTAND WHY YOU NEED TO BE HOME?
If you stay home, people get infected little by bit. Many don’t notice. The others, especially the elderly, but also some young people, we doctors and nurses take them, put them in ICU, treat them and return them to you. A little bit at a time.
If everyone leaves the house, the risk is that they will all get infected together and that we cannot manage them, with an important increase in mortality.
YOU DON ‘ T HAVE TO PANIC BUT TAKE IT SERIOUSLY. STAY HOME.
And above all, let me add, don’t come to the ER for futile reasons. We always say it but this time it’s even more important.”
So don’t be scared: each of you who will read this message has a very low probability of having big trouble from this infection, but try to behave so as to safeguard everyone’s good because there are many people (maybe even your acquaintances) who can instead risk a lot.
My endless date with self-isolation has led to some sobering realizations

From LifeSiteNews
Pfizer and Moderna’s mRNA COVID shots must now include warnings that they cause ‘extremely high risk’ of heart inflammation and irreversible damage in males up to age 24.
The Trump administration’s Food and Drug Administration (FDA) announced it will now require updated safety warnings on mRNA COVID-19 shots to include the “extremely high risk” of myocarditis/pericarditis and the likelihood of long-term, irreversible heart damage for teen boys and young men up to age 24.
The required safety updates apply to Comirnaty, the mRNA COVID shot manufactured by Pfizer Inc., and Spikevax, the mRNA COVID shot manufactured ModernaTX, Inc.
According to a press release, the FDA now requires each of those manufacturers to update the warning about the risks of myocarditis and pericarditis to include information about:
- the estimated unadjusted incidence of myocarditis and/or pericarditis following administration of the 2023-2024 Formula of mRNA COVID-19 shots and
- the results of a study that collected information on cardiac magnetic resonance imaging (cardiac MRI) in people who developed myocarditis after receiving an mRNA COVID-19 injection.
The FDA has also required the manufacturers to describe the new safety information in the adverse reactions section of the prescribing information and in the information for recipients and caregivers.
Additionally, the fact sheets for healthcare providers and for recipients and caregivers for Moderna COVID-19 shot and Pfizer-BioNTech COVID-19 shot, which are authorized for emergency use in individuals 6 months through 11 years of age, have also been updated to include the new safety information in alignment with the Comirnaty and Spikevax prescribing information and information for recipients and caregivers.
In a video published on social media, Dr. Vinay Prasad, director of the Center for Biologics Evaluation & Research Chief Medical and Scientific Officer, explained the alarming reasons for the warning updates.
While heart problems arose in approximately 8 out of 1 million persons ages 6 months to 64 years following reception of the cited shots, that number more than triples to 27 per million for males ages 12 to 24.
Prasad noted that multiple studies have arrived at similar findings.
COVID-19
Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

![]()
The Justice Centre for Constitutional Freedoms announces that a judge of the Ontario Court of Justice has ordered the RCMP and TD Bank to produce records relating to the freezing of Mr. Evan Blackman’s bank accounts during the 2022 Freedom Convoy protest.
Mr. Blackman was arrested in downtown Ottawa on February 18, 2022, during the federal government’s unprecedented use of the Emergencies Act. He was charged with mischief and obstruction, but he was acquitted of these charges at trial in October 2023.
However, the Crown appealed Mr. Blackman’s acquittal in 2024, and a new trial is scheduled to begin on August 14, 2025.
Mr. Blackman is seeking the records concerning the freezing of his bank accounts to support an application under the Charter at his upcoming retrial.
His lawyers plan to argue that the freezing of his bank accounts was a serious violation of his rights, and are asking the court to stay the case accordingly.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” says constitutional lawyer Chris Fleury.
“These records will hopefully reveal exactly how and why Mr. Blackman’s accounts were frozen,” he says.
Mr. Blackman agreed, saying, “I’m delighted that we will finally get records that may reveal why my bank accounts were frozen.”
This ruling marks a significant step in what is believed to be the first criminal case in Canada involving a proposed Charter application based on the freezing of personal bank accounts under the Emergencies Act.


RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
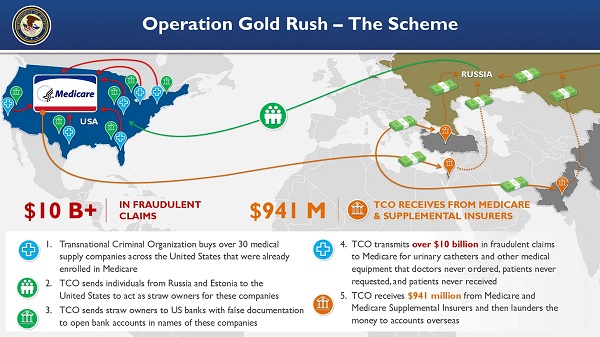
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud

-
 Alberta2 days ago
Alberta2 days agoAlberta Provincial Police – New chief of Independent Agency Police Service
-
 Business2 days ago
Business2 days agoWhy it’s time to repeal the oil tanker ban on B.C.’s north coast
-
 International2 days ago
International2 days agoCBS settles with Trump over doctored 60 Minutes Harris interview
-
 Energy2 days ago
Energy2 days agoIf Canada Wants to be the World’s Energy Partner, We Need to Act Like It
-
 Alberta2 days ago
Alberta2 days agoPierre Poilievre – Per Capita, Hardisty, Alberta Is the Most Important Little Town In Canada
-
 Aristotle Foundation2 days ago
Aristotle Foundation2 days agoHow Vimy Ridge Shaped Canada
-
 Alberta1 day ago
Alberta1 day agoAlberta uncorks new rules for liquor and cannabis
-
 Canadian Energy Centre1 day ago
Canadian Energy Centre1 day agoAlberta oil sands legacy tailings down 40 per cent since 2015