Health
RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump


The Vigilant Fox
This conversation with startle you, infuriate you—then lift your spirits
It’s not every day an active HHS Secretary sits down for 90 minutes straight with Tucker Carlson.
But that’s exactly what happened, and Kennedy instantly seized Carlson’s attention with a chilling story of CDC corruption.
He revealed that the health agency buried a 1999 internal study led by researcher Thomas Verstraten, which showed an alarming 1135% increase in autism risk from the hepatitis B vaccine.
Kennedy said the researchers were “shocked” by the findings.
So what did they do? They covered it up, according to Kennedy.
“They got rid of all the older children essentially and just had younger children who are too young to be diagnosed [with autism].”
RFK Jr. then explained the real reason why your pediatrician will kick you out of their practice for refusing vaccines.
“There’s a published article out there now that says that 50% of revenues to most pediatricians come from vaccines.”
It’s all about the money. The higher the vaccination rate, the bigger the bonus.
“And that’s why your pediatrician, if you say I want to go slow on the vaccines… will throw you out of his practice because you’re now jeopardizing that bonus structure.”
To the claim that the vaccine–autism link has been “debunked,” Kennedy had a message for Anderson Cooper, Jake Tapper, and everyone who smugly insists on it.
“None of the vaccines given to children in the first six months of life have ever been studied for autism.”
Let that sink in.
He went further, revealing that the CDC actually did find a link when they studied the DTaP vaccine.
But they dismissed it. Kennedy said they claimed it “didn’t count” because the data came from VAERS—the very system they use to track vaccine injuries.
So when the evidence pointed to harm, they simply claimed their own system wasn’t reliable enough and took no steps to fix it.
The vaccine corruption didn’t end there. Kennedy attested that the CDC killed off a vaccine injury reporting system that actually worked—because it worked too well.
It showed that 1 in 37 vaccines caused an injury.
Tucker was stunned.
“Of all vaccines?” he asked.
“Yeah,” Kennedy confirmed.
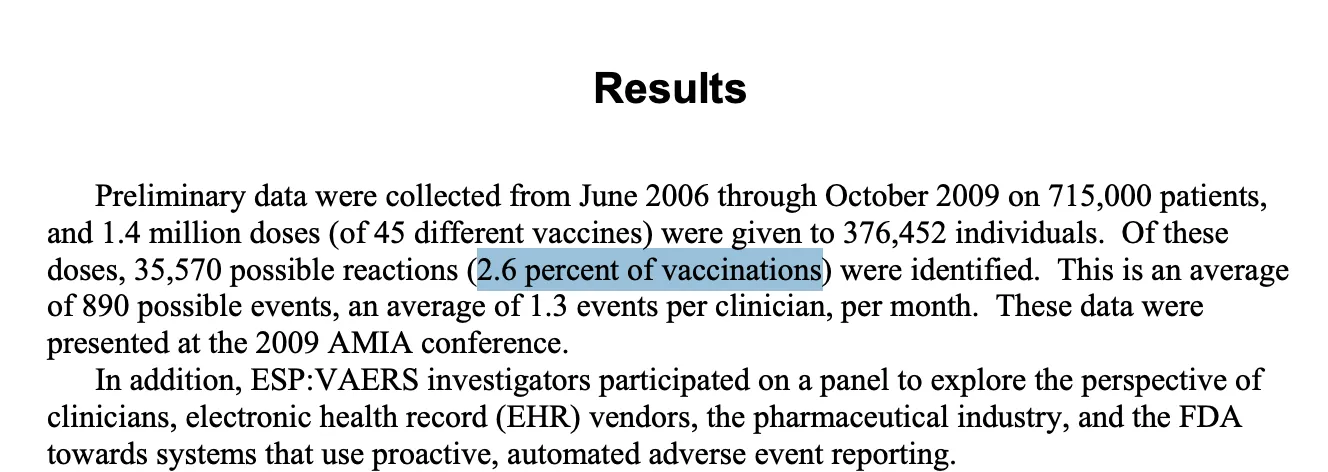
RFK Jr. explained that the CDC funded a study led by researcher Ross Lazarus. It compared a sophisticated machine-counting system to VAERS.
What did they find? VAERS was failing to catch over 99% of vaccine injuries.
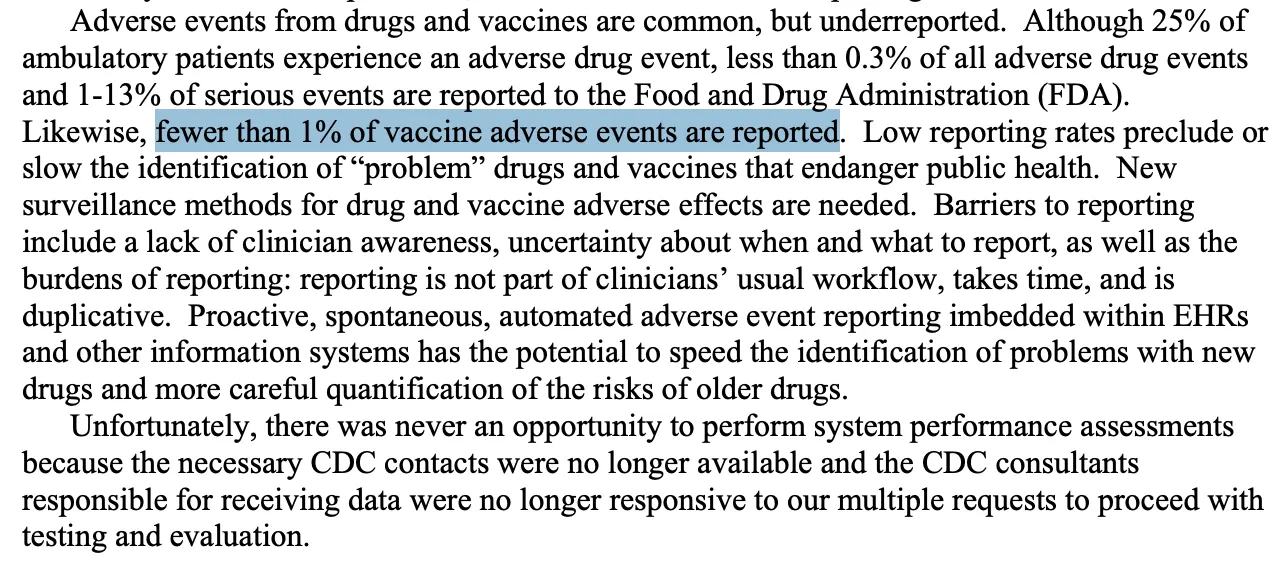
The new system also revealed that 2.6% of all vaccinations resulted in an injury.
So what did the CDC do? They shut it down in 2010. And they’re still using VAERS today—even though it’s a completely inadequate system.
But Kennedy didn’t stop at old vaccine scandals. He also broke down Pfizer’s own COVID vaccine trial data. That trial showed a 23% higher death rate in the vaccinated group.
• Pfizer gave 21,720 people the vaccine and 21,728 the placebo.
• One vaccinated person died of COVID. Two placebo recipients died. They used this tiny difference to claim “100% effective” based on relative risk reduction.
• But in absolute terms, it took 22,000 vaccinations to save one life.
• Over six months, 21 vaccinated participants died of all causes, compared to 17 in the placebo group—a 23.5% higher death rate.
And then there’s vaccine spokesperson Paul Offit, often seen on CNN and other mainstream networks.
Kennedy shared an infuriating story about how he literally “voted himself rich” on the rotavirus vaccine.
While serving on the CDC’s ACIP committee, Offit voted to add rotavirus vaccination to the childhood schedule—even as he was developing his own competing vaccine. He guaranteed demand for his product.
The first approved rotavirus vaccine, RotaShield, was yanked from the market for causing dangerous intussusception. Offit’s vaccine, RotaTeq, eventually replaced it.
He and his partners later sold their rights to Merck for $186 million. As RFK Jr. said, Offit literally “voted himself rich.”
When Carlson mentioned Fauci, Kennedy revealed how Fauci funded research that helped scientists hide evidence of lab-made viruses.
The technique, called “seamless ligation,” allowed researchers to engineer viruses in a lab without leaving telltale genetic fingerprints.
RFK Jr. explained:
“One of his fundees, Ralph Baric, from the University of North Carolina, developed a technique called the seamless ligation technique, which is a technique for hiding the laboratory origins of a manipulated virus.”
“… normally if there’s a virus manipulated, researchers can look at the DNA sequences and they can say this thing was created in a lab. Ralph Baric had developed a technique that he called the no-see technique and its technical name was seamless ligation, and it was a way of hiding evidence of human tampering.”
He called it the exact opposite of what real public health work should be. Carlson cut in, saying, “That’s what you would do if you’re creating viruses for biological warfare.”
The conversation shifted to Trump, leading to one of the biggest highlights of the entire interview.
First, Kennedy explained that Trump chose his cabinet in an unorthodox way: he wanted to see three clips of each candidate performing on TV before considering them for the job.
“One of the things with President Trump is that he really knows how to pick talent… For every one of the positions that he picked, he wanted to see three clips of them performing on TV. He’s very conscious of the fact that these people are going to be out selling his program to the public,” Kennedy said.
That’s when Kennedy ended the interview with a bang, sharing his genuine thoughts about Trump for three straight minutes. It was one of the standout moments of the entire conversation.
If you’re on the fence about Trump, listen to Kennedy here. It might just change how you see him.
“I had him pegged as a narcissist, when narcissists are incapable of empathy. And he’s one of the most empathetic people that I’ve met,” Kennedy said.
“He’s immensely curious, inquisitive, and immensely knowledgeable. He’s encyclopedic in certain areas that you wouldn’t expect,” he continued.
Kennedy added that Trump genuinely cares about soldiers who go to war, citing how Trump “always talks about the casualties on both sides” of the Russia–Ukraine conflict.
“Whether it’s vaccines or Medicaid or Medicare, he’s always thinking about how this impacts the little guy. And the Democrats have him pegged as a guy who’s sort of sitting in the Cabinet meeting talking about how can we make billionaires richer. He’s the opposite of that. He’s a genuine populist,” Kennedy said.
There’s so much more in this conversation, and it might change the way you think about vaccines forever.
For the full picture, watch the entire interview below.
I also wanted to let you know I’m sharing a lot more than just posts like this throughout the day.
For quick clips and updates, check out my Substack Notes page.
Alongside my top 10 daily roundup, it’s one of the best ways to keep up with the news cycle.
Just download the Substack app and follow my page there to see content that doesn’t appear on this main page.

Subscribe to The Vigilant Fox

DMSO’s unique therapeutic properties reveal the unifying thread between many different “incurable” eye diseases.
Story at a Glance:
• DMSO is an “umbrella remedy” capable of treating a wide range of challenging ailments due to its combination of therapeutic properties (e.g., reducing inflammation, improving circulation, and reviving dying cells).
• DMSO has a unique affinity for the eyes, resulting in it (often spontaneously) treating a wide range of visual disorders that frequently cannot be treated with conventional therapeutic options.
• DMSO’s ability to restore circulation, revive dying cells, and stabilize misfolded proteins allows it to treat a variety of retinal diseases (e.g., macular degeneration, diabetic retinopathy or retinitis pigmentosa—in some cases reversing permanent blindness), eliminate visual obstructions (e.g., floaters and cataracts), reverse glaucoma or Fuchs’ dystrophy, and restore normal focus (frequently eliminating the need for glasses).
• DMSO’s anti-inflammatory and antimicrobial properties allow it to treat dry eyes, inflammatory diseases around the eye (e.g., blepharitis, styes, and psoriasis) or within the eye (e.g., iritis, uveitis, conjunctivitis, keratitis), along with bacterial, fungal, parasitic, or viral eye infections such as shingles.
•DMSO’s healing properties also allow it to heal a variety of eye injuries (including severe ones which would otherwise require eye removal), skin issues around the eye (e.g., burns, skin tags, and under-eye bags), and eliminate eye muscle spasms.
•This article will review the extensive data demonstrating DMSO’s efficacy for eye diseases, along with an examination of the most common protocols used for them and other natural approaches that also aid in the treatment of common eye disorders.
Since 2024, I have been working diligently to present the extensive data that DMSO is a remarkable therapeutic that is uniquely suited to treat many highly challenging medical conditions due to its counteracting many root causes of disease (whereas, in contrast, vaccines cause a myriad of health issues by inducing those key drivers of illness). From this, I’ve compiled a series of articles synthesizing thousands of studies that have shown DMSO effectively treats:
- Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
- A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
- Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
- A wide range of autoimmune, protein, and contractile disorders, such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
- A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
- A wide range of internal organ diseases (discussed here).
- Many different respiratory disorders, including asthma and COPD (discussed here)
- Many different gastrointestinal disorders, such as bowel inflammation, cirrhosis, and pancreatitis (discussed here)
- A wide range of skin conditions, such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
- Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
- Many aspects of cancer (e.g., many of cancer’s debilitating symptoms, making cancer treatments more potent, greatly reducing the toxicity of conventional therapies, and turning cancer cells back into normal cells), which I discussed here.
Since the evidence in those articles (along with one on how DMSO can be synergistically combined with pharmaceuticals and another on how DMSO combines with natural therapies) made a compelling case for the use of DMSO, many readers opted to start using it. Many of them, in turn, had remarkable improvements which caused them to recommend DMSO to their peers, and because of all those successes, a widespread interest in DMSO has now emerged.
On one hand, this has been quite surprising to me as the information I publicized has been widely available for decades, but (possibly due to it being impossible to profit off DMSO because of how little it costs) most of the people exposed to this series were not even aware this therapy existed, let alone what DMSO could do. Conversely, the groundswell of interest is not surprising as it’s nearly identical to what happened when DMSO was first discovered in the 1960s and it rapidly became the most popular drug in America—particularly since relatively minimal progress has been made on most of the “incurable” conditions it cured back then. Consider for example this 1980 segment 60 minutes created, which showed the remarkable results generated from the therapeutic use of DMSO and more importantly, the exact same stonewalling and suppression of DMSO from the FDA that we saw throughout COVID-19:
User DMSO Reports
Because of DMSO’s high degree of efficacy, the moment I began the series, I started being flooded with testimonials from readers of the remarkable improvements DMSO had created for them. Before long, I realized I was in a similar situation to what I’d been in throughout COVID-19.
I have long believed one of the core strategies the ruling class always follows is to establish rigid hierarchical systems that have dominion over critical facets of society and then buy out the top of the pyramid, as that provides a relatively low-cost way to control the entire society. In the case of medicine, this has translated to having pharmaceutical compliant individuals (through industry funding and media complicity) be anointed as experts who reinforce the profitable orthodoxy alongside having medical journals only publish things which cater to the existing vested interests.
Because of this, things that are “controversial” (threatening vested interests) are rarely published in a “credible” medium, and as a result, anyone who tries to advocate for them is not listened to; instead, they are chastised for endorsing “unproven” and unscientific beliefs.
When the COVID vaccines hit the market, I had expected they would cause a significant number of chronic issues that would take years to be recognized—so I was quite shocked to be immediately flooded with reports across the country of severe reactions of all types from the vaccine. Because of this, I felt I needed to log them as I knew injuries like these would never get published in medical journals and I wanted to have some type of proof that vaccine injuries were real, so in the future I could present accurate information to skeptical parties. I hence spent an inordinate amount of time interviewing those involved and compiling all of them and after unexpectedly gaining a Substack audience, I published that log, and it went viral because my small sample accurately represented the pattern of vaccine injuries everyone was seeing around them and because more than a year into the COVID vaccine rollout, no one had done anything similar—despite the massive demand for this type of information.
In the process of doing that, I had also received a lot of reports of individuals who appeared to be being injured by COVID vaccine shedding—despite this being “impossible” based on the purported design of the vaccines. As the reports, like those for the COVID-19 vaccine injuries, were consistent in character (and like the vaccines many affected by shedding were understandably desperate for information on the topic) I decided to spend a year compiling thousands of those reports as I knew there would never be a journal willing to touch the subject. Following this, I then produced a synthesis of that data which showed there were clear repeating patterns to mRNA shedding and provided the critical mechanisms to explain this seemingly inexplicable phenomenon. That, in turn, was an inordinate amount of work to do, but succeeded and made many realize shedding is a real risk of the mRNA technology—something which will be critical for opposing future attempts to inject the population with experimental gene therapies.
In the case of DMSO, as I started receiving all of these reports (at a time when I had essentially finished the shedding project), I realized that I had access to a unique dataset that had not previously been available. More importantly, because there were so many different things that DMSO could treat, a dataset like this would likely be the only place much of that therapeutic data could ever be compiled (as no one would ever get around to conducting studies on many of those uses—particularly since the current academic publishing climate is much more hostile to publishing unorthodox research now than it was fifty years ago).
So, over the last 13 months, one of my primary projects has been to compile all the reports I’ve received (which I did in the comments here), and I presently have 4,721 comments—of which I think roughly 3,000 are unique stories of therapeutic benefit people have experienced. In turn, my plan is to eventually compile and synthesize all of that, but as doing that will take at least a month, I’ve held off until the end of the series (so I wouldn’t have to redo it with new data that was subsequently received).
Note: my general sense from all the testimonials I’ve received is that between 80-90% of users have a positive response to using DMSO (which is frankly extraordinary), with lower rates (50%) being seen for certain issues which are harder to correctly treat with DMSO, and give or take 0% success rates being seen for issues DMSO is not thought to treat (suggesting the sample I’m observing is representative of real life data).
Within those comments, while most of the reports I’ve received are consistent with what DMSO is recognized to do (e.g., rapidly eliminating debilitating pain that nothing else had worked on), some were quite extraordinary and not what I’d expected to come across. For example, after I learned a 75 year old reader who’d been blind since birth had regained their sight after using DMSO to treat a sinus issue, I realized his story needed to be shared:
Note: as fate had it, Murray lived about 3 hours away from Rebecca Cunningham, the Texas-based documentary film maker who cured her neighbor’s terminal COPD with nebulized DMSO, after which millions saw Dan’s COPD story.1,2 As DMSO changed her life, she is currently collecting other DMSO testimonials on her Rumble channel and kindly agreed to travel to Murray to film this. If you have a story to share and are ever passing through Wimberley or visiting the hill country in Texas, please reach out to her.
In compiling these reports, I was struck by how many were for the eyes, by how well DMSO worked across an extensive range of eye conditions, and by the fact that, in the majority of cases, it provided better results than could be expected from existing ophthalmology options.
Note: the only well-recognized ophthalmologic conditions I did not receive reports on were amblyopia, strabismus, diabetic retinopathy, keratitis, optic neuritis, retinal detachment, retinopathy of prematurity, chalazions, central retinal vein occlusion (although a reader’s branched retinal vein occlusion responded to DMSO), and eye cancers—many of which, as I will show in this article, existing data sources suggest do respond to DMSO.
Later, while translating the discoveries of the German community, I learned their data matched that of the readers here:
One of the first new adopters of DMSO (circa 2012), began successfully using highly diluted DMSO for eye treatments in his practice. This led to a network of practitioners using DMSO for eye health, accumulating substantial experience, and, in many cases, treating eye issues where the cause could not be determined.
In general, there are a surprising number of successful reports using DMSO eye drops for a wide variety of eye symptoms and diseases. So many, in fact, that I now consider the DMSO eye solution an exceptional “eye care.”
Many users (especially those with heavy screen time) apply DMSO preventively to maintain eye freshness, improve tear quality, and reduce night glare. Positive effects, including improved vision, better tear film, fresher eyes, and reduced night glare, are often reported after the first few applications, enhancing overall eye comfort and function—including in people whom ophthalmologists did not diagnose with any eye conditions.
The positive effects are often reported after the first few applications, but I consider [low dose eye drops] a longer-term option. Due to the excellent diagnostic results and the complete absence of adverse effects from low dose drops (including results from ophthalmologists for a wide range of eye disorders) I increasingly view DMSO eye drops as a preventative measure, eye care for those with (still) healthy eyes, since modern life, particularly excessive screen time, places significant demands on our eyes.
Note: the above was extracted from an AI-generated summary of hundreds of hours of non-English lectures, then further condensed by me and hence not a direct quote (but one that accurately represents the author’s statements).
While this might be difficult to believe, consider a parallel situation. Another umbrella remedy I have been deeply impressed by, ultraviolet blood irradiation (which has many similar therapeutic properties to DMSO), has a vast volume of literature demonstrating its clinical value—including for numerous immensely challenging to treat diseases. Yet, virtually none of the medical profession even knows this therapy exists.
For this reason, we are currently sorting through thousands of UVBI studies, including dozens of studies (many of which were conducted with hundreds of patients) which show UVBI treats a myriad of challenging ophthalmologic conditions such as:
blepharitis,1 keratitis,1 corneal inflammation,1 herpes zoster ophthalmicus,1 traumatic eye infection,1 uveitis,1,2,3,4,5 iridocyclitis,1,2 choroiditis,1 chorioretinopathy,1,2,3,4 choroidal and chorioretinal dystrophy,1,2 macular degeneration,1 retinitis pigmentosa,1,2 retinal contusion,1 retinal ischemia,1,2 retinal and fundus hemorrhages,1,2,3,4 retinal artery and vein occlusions,1,2,3,4,5,6,7,8,9,1
0,11,12,13,14,15 diabetic retinopathy,1 ischemic optic neuropathy,1,2,3,4,5 optic neuritis,1,2,3 optic nerve atrophy (traumatic or inflammatory),1,2,3 encephalopathic vision loss1
Note: in this article, each superscipt number links to either a reader’s story or an applicable study—like the many I listed above (which the ophthalmology profession does not realize exists).
As such, the purpose of this article will be to highlight exactly how DMSO is transforming ophthalmology, along with the supporting data.
The Forgotten Side of Medicine is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
To learn more about this newsletter and how others have benefitted from it, click here!
Note: the best review paper on DMSO’s uses in ophthalmology (which is an excellent resource to provide to physicians who are skeptical of using DMSO for the eyes) can be read here.
![]()
The Justice Centre for Constitutional Freedoms has released a new report titled Canada’s Surrender of Sovereignty: New WHO health regulations undermine Canadian democracy and Charter freedoms. Authored by Nigel Hannaford, a veteran journalist and researcher, the report warns that Canada’s acceptance of the World Health Organization’s (WHO) revised International Health Regulations (IHR) represents a serious erosion of national independence and democratic accountability.
The IHR amendments, which took effect on September 19, 2025, authorize the WHO Director-General to declare global “health emergencies” that could require Canada to follow directives from bureaucrats in Geneva, bypassing the House of Commons and the will of Canadian voters.
The WHO regards these regulations as “binding,” despite having no ability or legal authority to impose such regulations. Even so, Canada is opting to accept the regulations as binding.
By accepting the WHO’s revised IHR, the report explains, Canada has relinquished its own control over future health crises and instead has agreed to let the WHO determine when a “pandemic emergency” exists and what Canada must do to respond to it, after which Canada must report back to the WHO.
In fact, under these International Health Regulations, the WHO could demand countries like Canada impose stringent freedom-violating health policies, such as lockdowns, vaccine mandates, or travel restrictions without debate, evidence review, or public accountability, the report explains.
Once the WHO declares a “Pandemic Emergency,” member states are obligated to implement such emergency measures “without delay” for a minimum of three months.
Importantly, following these WHO directives would undermine government accountability as politicians may hide behind international “commitments” to justify their actions as “simply following international rules,” the report warns.
Canada should instead withdraw from the revised IHR, following the example of countries like Germany, Austria, Italy, Czech Republic, and the United States. The report recommends continued international cooperation without surrendering control over domestic health policies.
Constitutional lawyer Allison Pejovic said, “[b]y treating WHO edicts as binding, the federal government has effectively placed Canadian sovereignty on loan to an unelected international body.”
“Such directives, if enforced, would likely violate Canadians’ Charter rights and freedoms,” she added.
Mr. Hannaford agreed, saying, “Canada’s health policies must be made in Canada. No free and democratic nation should outsource its emergency powers to unelected bureaucrats in Geneva.”
The Justice Centre urges Canadians to contact their Members of Parliament and demand they support withdrawing from the revised IHR to restore Canadian sovereignty and reject blind compliance with WHO directives.




Disabled Canadians increasingly under pressure to opt for euthanasia during routine doctor visits

Petition threatens independent school funding in Alberta
From Underdog to Top Broodmare

Busting five myths about the Alberta oil sands

-
MAiD23 hours ago
Disabled Canadians increasingly under pressure to opt for euthanasia during routine doctor visits
-
Alberta1 day ago
Petition threatens independent school funding in Alberta
-
Alberta2 days ago
Busting five myths about the Alberta oil sands
-
 Courageous Discourse2 days ago
Courageous Discourse2 days agoNo Exit Wound – EITHER there was a very public “miracle” OR Charlie Kirk’s murder is not as it appears
-
 Business24 hours ago
Business24 hours agoCanada Revenue Agency found a way to hit “Worse Than Rock Bottom”
-
 Digital ID22 hours ago
Digital ID22 hours agoToronto airport requests approval of ‘digital IDs’ for domestic airport travel
-
 Fraser Institute2 days ago
Fraser Institute2 days agoMétis will now get piece of ever-expanding payout pie
-
 Business2 days ago
Business2 days agoCarney government risks fiscal crisis of its own making