Addictions
B.C. parents powerless to help their addicted teens


B.C. parents say the province’s safer supply program and legal treatment framework leave them powerless to help their addicted teens
On Aug. 19, 2022, Kamilah Sword took a single hydromorphone pill, believing it to be safe. She overdosed and was found dead by her grandmother the next day. She was 14.
Kamilah believed the drug was safe — despite having bought it illicitly — because she was told it came from a government-run “safer supply” program, according to Kamillah’s best friend Grace Miller and her father.
“I’ll never get to see her get married, never have grandkids, never get to see her graduate,” said Kamilah’s father, Gregory Sword, lowering his chin to keep his voice steady.
“It’s a black hole in the heart that never heals.”
Sword faced significant challenges trying to get his daughter help during the year he was aware she was struggling with addiction. He blames British Columbia’s safer supply program and the province’s legal youth treatment framework for exacerbating his daughter’s challenges and ultimately contributing to her death.
“It’s a B.C. law — you cannot force a minor into rehab without their permission,” said Sword. “You cannot parent your kid between the ages of 12 and 18 without their consent.”
Sword is now pursuing legal action against the B.C. and federal governments and several health agencies, seeking accountability for what he views as systemic failures.
B.C.’s “Safe” supply program
B.C.’s prescribed safer supply program, which was first launched in 2020, is designed to reduce substance users’ reliance on dangerous street drugs. Users are prescribed hydromorphone — an opioid as potent as heroin — as an alternative to using potentially lethal street drugs.
However, participants in the program often sell their hydromorphone, in some cases to teenagers, to get money to buy stronger drugs like fentanyl.
According to Grace Miller, she and Kamilah would obtain hydromorphone — which is commonly referred to as Dilaudid or “dillies” — from a teenage friend who bought them in Vancouver’s Downtown Eastside. The neighbourhood, which is the epicentre of Vancouver’s drug crisis, is a 30-minute SkyTrain ride from the teenagers’ home in Port Coquitlam.
Sword says he initially thought “dillies” referred to Dairy Queen’s Dilly Bars. “My daughter would ask me for $5, [and say], ‘Yeah, we’re going to Dairy Queen for a Dilly Bar.’ I had no idea.”
He says he only learned about hydromorphone after the coroner informed him that Kamilah had three substances in her system: cocaine, MDMA and hydromorphone.
“I had to start talking to people to figure out what [hydromorphone] was and where it was coming from.”
Sword is critical of B.C.’s safer supply program for being presented as safe and for lacking monitoring safeguards. “[Kamilah] knew where [the drugs] were coming from so she felt safe because her dealer would keep on telling her, ‘This is safe supply,’” Sword said.
In February, B.C. changed how it refers to the program from “prescribed safer supply” to “prescribed alternatives.”
Grace says another problem with the program is the quantities of drugs being distributed.
“It would be a big difference if the prescriptions that they were giving out were dosed properly,” she said, noting addicts would typically sell bottles containing 14 pills, with pricing starting at $1 a pill.
‘Safer supply’
Sword estimates his daughter struggled with addiction for about 18 to 24 months before her final, fatal overdose.
After Kamilah overdosed for the first time on Aug. 21, 2021, he tried to get her into treatment. A drug counsellor told him that, because she was over 12, she would need to verbally consent. Kamilah refused treatment.
B.C.’s Infants Act allows individuals aged 12 or older to consent to their own medical treatment if they understand the treatment and its implications. The province’s Mental Health Act requires minors aged 12 to 16 to consent to addiction or mental health treatment.
While parents can request involuntary admission for children under 16, a physician or nurse practitioner must first confirm the presence of a mental disorder that requires treatment. No law specifically addresses substance-use disorders in minors.
When Kamilah was admitted to the hospital on one occasion, she underwent a standard psychiatric evaluation and was quickly discharged — despite Sword’s protests.
Ontario also has a mental health law governing involuntary care. Similar to B.C., they permit involuntary care only where a minor has been diagnosed with a mental disorder.
By contrast, Alberta’s Protection of Children Abusing Drugs Act enables a parent or guardian to obtain a court order to place a child under 18 who is struggling with addiction into a secure facility for up to 15 days for detoxification, stabilization and assessment. Alberta is unique among the provinces and territories in permitting involuntary care of minors for substance-use issues.
Grace, who also became addicted to opioids, says her recovery journey involved several failed attempts.
“I never thought I would have almost died so many times,” said Grace, who is now 16. “I never thought I would even touch drugs in my life.”
Grace’s mother Amanda (a pseudonym) faced similar struggles as Sword in trying to get help for her daughter. Amanda says she was repeatedly told nothing more could be done for Grace, because Grace would not consent to treatment.
“One time, [Grace] overdosed at home, and I had to Narcan her because she was dead in her bed,” Amanda said. “I told the paramedic, ‘Our system is broken.’ And she just said, ‘Yes, I know.’”
Yet Grace, who today has been sober for 10 months, would question whether she even had the capacity to consent to treatment when she was addicted to drugs.
Under B.C.’s Health Care (Consent) and Care Facility (Admission) Act, an adult is only considered to have consented to health care if their consent is voluntary, informed, legitimately obtained and the individual is capable of making a decision about their care.
“Mentally able to give consent?” said Grace. “No, I was never really mentally there.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
System failure
Today, Sword is one of two plaintiffs leading a class-action lawsuit against several provincial and federal health authorities and organizations, including the B.C. Ministry of Health, Health Canada, Vancouver Coastal Health and Vancouver Island Health.
All four of these agencies declined to comment for this story, citing the ongoing court proceedings.
The lawsuit was filed Aug. 15 and is currently awaiting certification to proceed. It alleges the coroner initially identified safer supply drugs as a cause of Kamilah’s death, but later changed the report to omit this reference due to pressure from the province or for other unknown reasons.
It further alleges B.C. and Ottawa were aware that drugs prescribed under safer supply programs were being diverted as early as March 2021, but failed to monitor or control the drugs’ distribution. It points to a Health Canada report and data showing increased opioid-related problems from safer supply programs.
According to Amanda, Kamilah had wanted to overcome her addiction but B.C.’s system failed her.
“I had multiple conversations with Kamilah, and I know Kamilah wanted to get clean,” she says. “But she felt so stuck, like she couldn’t do it, and she felt guilty and ashamed.”
Grace, who battled addiction for four years, is relieved to be sober.
“I’ve never, ever been happier. I’ve never been healthier. It’s the best thing I’ve done for myself,” she said. “It’s just hard when you don’t have your best friend to do it with.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Break The Needle. Our content is always free – but if you want to help us commission more high-quality journalism, consider getting a voluntary paid subscription.


First responders say it is not overdoses that leave them feeling burned out—it is the endless cycle of calls they cannot meaningfully resolve
The soap bottle just missed his head.
Standing in the doorway of a cluttered Halifax apartment, Derek, a primary care paramedic, watched it smash against the wall.
Derek was there because the woman who threw it had called 911 again — she did so nearly every day. She said she had chest pain. But when she saw the green patch on his uniform, she erupted. Green meant he could not give her what she wanted: fentanyl.
She screamed at him to call “the red tags” — advanced care paramedics authorized to administer opioids. With none available, Derek declared the scene unsafe and left. Later that night, she called again. This time, a red-patched unit was available. She got her dose.
Derek says he was not angry at the woman, but at the system that left her trapped in addiction — and him powerless to help.
First responders across Canada say it is not overdoses that leave them feeling burned out — it is the endless cycle of calls they cannot meaningfully resolve. Understaffed, overburdened and dispatched into crises they are not equipped to fix, many feel morally and emotionally drained.
“We’re sending our first responders to try and manage what should otherwise be dealt with at structural and systemic levels,” said Nicholas Carleton, a University of Regina researcher who studies the mental health of public safety personnel.
Canadian Affairs agreed to use pseudonyms for the two frontline workers referenced in this story. Canadian Affairs also spoke with nine other first responders who agreed to speak only on background. All of these sources cited concerns about workplace retaliation for speaking out.
Moral injury
Canada’s opioid crisis is pushing frontline workers such as paramedics to the brink.
A 2024 study of 350 Quebec paramedics shows one in three have seriously considered suicide. Globally, ambulance workers have among the highest suicide rates of public service personnel.
Between 2017 and 2024, Canadian paramedics responded to nearly 240,000 suspected opioid overdoses. More than 50,000 of those were fatal.
Yet many paramedics say overdose calls are not the hardest part of the job.
“When they do come up, they’re pretty easy calls,” said Derek. Naloxone, a drug that reverses overdoses, is readily available. “I can actually fix the problem,” he said. “[It’s a] bit of instant gratification, honestly.”
What drains him are the calls they cannot fix: mental health crises, child neglect and abuse, homelessness.
“The ER has a [cardiac catheterization] lab that can do surgery in minutes to fix a heart attack. But there’s nowhere I can bring the mental health patients.
“So they call. And they call. And they call.”
Thomas, a primary care paramedic in Eastern Ontario, echoes that frustration.
“The ER isn’t a good place to treat addiction,” he said. “They need intensive, long-term psychological inpatient treatment and a healthy environment and support system — first responders cannot offer that.”
That powerlessness erodes trust. Paramedics say patients with addictions often become aggressive, or stop seeking help altogether.
“We have a terrible relationship with the people in our community struggling with addiction,” Thomas said. “They know they will sit in an ER bed for a few hours while being in withdrawals and then be discharged with a waitlist or no follow-up.”
Carleton, of the University of Regina, says that reviving people repeatedly without improvement decreases morale.
“You’re resuscitating someone time and time again,” said Carleton, who is also director of the Psychological Trauma and Stress Systems Lab, a federal unit dedicated to mental health research for public safety personnel. “That can lead to compassion fatigue … and moral injury.”
Katy Kamkar, a clinical psychologist focused on first responder mental health, says moral injury arises when workers are trapped in ethically impossible situations — saving a life while knowing that person will be back in the same state tomorrow.
“Burnout is … emotional exhaustion, depersonalization, and reduced personal accomplishment,” she said in an emailed statement. “High call volumes, lack of support or follow-up care for patients, and/or bureaucratic constraints … can increase the risk of reduced empathy, absenteeism and increased turnover.”
Kamkar says moral injury affects all branches of public safety, not just paramedics. Firefighters, who are often the first to arrive on the scene, face trauma from overdose deaths. Police report distress enforcing laws that criminalize suffering.
Understaffed and overburdened
Staffing shortages are another major stressor.
“First responders were amazing during the pandemic, but it also caused a lot of fatigue, and a lot of people left our business because of stress and violence,” said Marc-André Périard, vice president of the Paramedic Chiefs of Canada.
Nearly half of emergency medical services workers experience daily “Code Blacks,” where there are no ambulances available. Vacancy rates are climbing across emergency services. The federal government predicts paramedic shortages will persist over the coming decade, alongside moderate shortages of police and firefighters.
Unsafe work conditions are another concern. Responders enter chaotic scenes where bystanders — often fellow drug users — mistake them for police. Paramedics can face hostility from patients they just saved, says Périard.
“People are upset that they’ve been taken out of their high [when Naloxone is administered] and not realizing how close to dying they were,” he said.
Thomas says safety is undermined by vague, inconsistently enforced policies. And efforts to collect meaningful data can be hampered by a work culture that punishes reporting workplace dangers.
“If you report violence, it can come back to haunt you in performance reviews” he said.
Some hesitate to wait for police before entering volatile scenes, fearing delayed response times.
“[What] would help mitigate violence is to have management support their staff directly in … waiting for police before arriving at the scene, support paramedics in leaving an unsafe scene … and for police and the Crown to pursue cases of violence against health-care workers,” Thomas said.
“Right now, the onus is on us … [but once you enter], leaving a scene is considered patient abandonment,” he said.
Upstream solutions
Carleton says paramedics’ ability to refer patients to addiction and mental health referral networks varies widely based on their location. These networks rely on inconsistent local staffing, creating a patchwork system where people easily fall through the cracks.
“[Any] referral system butts up really quickly against the challenges our health-care system is facing,” he said. “Those infrastructures simply don’t exist at the size and scale that we need.”
Périard agrees. “There’s a lot of investment in safe injection sites, but not as much [resources] put into help[ing] these people deal with their addictions,” he said.
Until that changes, the cycle will continue.
On May 8, Alberta renewed a $1.5 million grant to support first responders’ mental health. Carleton welcomes the funding, but says it risks being futile without also addressing understaffing, excessive workloads and unsafe conditions.
“I applaud Alberta’s investment. But there need to be guardrails and protections in place, because some programs should be quickly dismissed as ineffective — but they aren’t always,” he said.
Carleton’s research found that fewer than 10 mental health programs marketed to Canadian governments — out of 300 in total — are backed up by evidence showing their effectiveness.
In his view, the answer is not complicated — but enormous.
“We’ve got to get way further upstream,” he said.
“We’re rapidly approaching more and more crisis-level challenges… with fewer and fewer [first responders], and we’re asking them to do more and more.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
News release from Alberta RCMP
Virtual Opioid Dependency Program serves vulnerable population in Red Deer
Since April 2024, your Alberta RCMP’s Community Safety and Well-being Branch (CSWB) has been piloting the Virtual Opioid Dependency Program (VODP) program in Red Deer to assist those facing opioid dependency with initial-stage intervention services. VODP is a collaboration with the Government of Alberta, Recovery Alberta, and the Alberta RCMP, and was created to help address opioid addiction across the province.
Red Deer’s VODP consists of two teams, each consisting of a police officer and a paramedic. These teams cover the communities of Red Deer, Innisfail, Blackfalds and Sylvan Lake. The goal of the program is to have frontline points of contact that can assist opioid users by getting them access to treatment, counselling, and life-saving medication.
The Alberta RCMP’s role in VODP:
- Conducting outreach in the community, on foot, by vehicle, and even UTV, and interacting with vulnerable persons and talking with them about treatment options and making VODP referrals.
- Attending calls for service in which opioid use may be a factor, such as drug poisonings, open drug use in public, social diversion calls, etc.
- Administering medication such as Suboxone and Sublocade to opioid users who are arrested and lodged in RCMP cells and voluntarily wish to participate in VODP; these medications help with withdrawal symptoms and are the primary method for treating opioid addiction. Individuals may be provided ongoing treatment while in police custody or incarceration.
- Collaborating with agencies in the treatment and addiction space to work together on client care. Red Deer’s VODP chairs a quarterly Vulnerable Populations Working Group meeting consisting of a number of local stakeholders who come together to address both client and community needs.
While accountability for criminal actions is necessary, the Alberta RCMP recognizes that opioid addiction is part of larger social and health issues that require long-term supports. Often people facing addictions are among offenders who land in a cycle of criminality. As first responders, our officers are frequently in contact with these individuals. We are ideally placed to help connect those individuals with the VODP. The Alberta RCMP helps those individuals who wish to participate in the VODP by ensuring that they have access to necessary resources and receive the medical care they need, even while they are in police custody.
Since its start, the Red Deer program has made nearly 2,500 referrals and touchpoints with individuals, discussing VODP participation and treatment options. Some successes of the program include:
- In October 2024, Red Deer VODP assessed a 35-year-old male who was arrested and in police custody. The individual was put in contact with medical care and was prescribed and administered Suboxone. The team members did not have any contact with the male again until April 2025 when the individual visited the detachment to thank the team for treating him with care and dignity while in cells, and for getting him access to treatment. The individual stated he had been sober since, saying the treatment saved his life.
- In May 2025, the VODP team worked with a 14-year-old female who was arrested on warrants and lodged in RCMP cells. She had run away from home and was located downtown using opioids. The team spoke to the girl about treatment, was referred to VODP, and was administered Sublocade to treat her addiction. During follow-up, the team received positive feedback from both the family and the attending care providers.
The VODP provides same-day medication starts, opioid treatment transition services, and ongoing opioid dependency care to people anywhere in Alberta who are living with opioid addiction. Visit vodp.ca to learn more.
“This collaboration between Alberta’s Government, Recovery Alberta and the RCMP is a powerful example of how partnerships between health and public safety can change lives. The Virtual Opioid Dependency Program can be the first step in a person’s journey to recovery,” says Alberta’s Minister of Mental Health and Addiction Rick Wilson. “By connecting people to treatment when and where they need it most, we are helping build more paths to recovery and to a healthier Alberta.”
“Part of the Alberta RCMP’s CSWB mandate is the enhancement of public safety through community partnerships,” says Supt. Holly Glassford, Detachment Commander of Red Deer RCMP. “Through VODP, we are committed to building upon community partnerships with social and health agencies, so that we can increase accessibility to supports in our city and reduce crime in Red Deer. Together we are creating a stronger, safer Alberta.”


RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
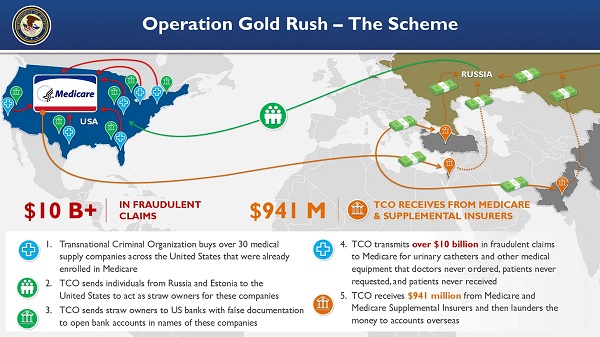
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud

-
 Indigenous2 days ago
Indigenous2 days agoInternal emails show Canadian gov’t doubted ‘mass graves’ narrative but went along with it
-
 Bruce Dowbiggin2 days ago
Bruce Dowbiggin2 days agoEau Canada! Join Us In An Inclusive New National Anthem
-
 Crime2 days ago
Crime2 days agoEyebrows Raise as Karoline Leavitt Answers Tough Questions About Epstein
-
 Business2 days ago
Business2 days agoCarney’s new agenda faces old Canadian problems
-
 Alberta2 days ago
Alberta2 days agoCOWBOY UP! Pierre Poilievre Promises to Fight for Oil and Gas, a Stronger Military and the Interests of Western Canada
-
 Alberta2 days ago
Alberta2 days agoAlberta and Ontario sign agreements to drive oil and gas pipelines, energy corridors, and repeal investment blocking federal policies
-
 Crime1 day ago
Crime1 day ago“This is a total fucking disaster”
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV