Health
Trump’s surgeon general pick is a threat to Big Pharma, not medical freedom


From LifeSiteNews
By John Leake
Dr. Casey Means has faced backlash for spotlighting America’s metabolic crisis and pushing for reform of junk food production and marketing instead of the hyper-vaccination problem.
“You are what you eat,” as the old saying goes.
Anyone who visits a U.S. airport and looks around can see that something has gone terribly wrong with the metabolic health of the American people. It’s therefore an astonishing fact that President Donald Trump’s new pick for Surgeon General, Casey Means, has come under fire from all quarters for suggesting that there is something wrong with our food supply that needs to be investigated and corrected.
I get it, it’s up to the individual to avoid eating junk food. Nevertheless, it is still perfectly sensible public policy to ascertain how the American food industry deliberately engineers and encourages the consumption of junk food, especially among the young.
A thorough investigation of the American food industry could also yield sensible strategies for investing in higher quality food production. This, in turn, could revitalize America’s moribund agricultural sector. There’s a lot of talk of “bringing jobs back to America.” How about jobs producing high quality food in local markets all over the country?
I am aware of the suspicion within the medical freedom movement that Casey Means is controlled opposition for changing the subject from the real enemy of public health – namely, the hyper-vaccination of children, which is doing Lord knows what to their gastrointestinal, neurological, and metabolic health.
Though I appreciate the fact that the Vaccine-Industrial Complex is skilled at changing the subject to divert critical scrutiny away from vaccines, I have not seen any evidence that Casey Means is serving the Vaccine Cartel with her stated objective of scrutinizing the food supply.

Some of my readers have pointed out that Casey’s father, Grady Means, worked in President Gerald Ford’s administration as an assistant to Vice President Nelson Rockefeller, and that this should be regarded as evidence that she is serving undeclared interests. One should remember that it was the Ford Administration that quickly pulled the Swine Flu vaccine off the market after reports that about 25 people had died after receiving the shots and a few hundred developed Guillain-Barre.
Moreover, the fact that one’s family has worked for U.S. government institutions is not evidence that one is compromised by nefarious interests. A notable example of this was young Tyler Shultz, who blew the whistle on Theranos, even though his grandfather – former Secretary of State George Shultz – was an investor in the bogus blood testing company and was extremely unhappy about his grandson’s decision.
Secretary Kennedy supports her, and he has done more than anyone in the public forum to raise concern about vaccine safety.
People frequently ask me why Secretary Kennedy isn’t working faster to counter the unwarranted influence of Vaccine-Industrial Complex. This strikes me as the equivalent of complaining that Indiana Jones didn’t escape from the Well of Souls fast enough.
Secretary Kennedy has entered one of the largest dens of venomous serpents ever erected. It’s going to take him a while to slash through it.
Reprinted with permission from Focal Points.
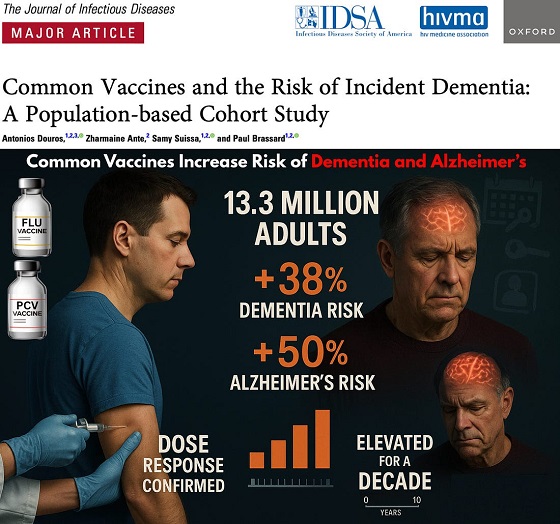

The single largest vaccine–dementia study ever conducted (n=13.3 million) finds risk intensifies with more doses, remains elevated for a full decade, and is strongest after flu and pneumococcal shots.
The single largest and most rigorous study ever conducted on vaccines and dementia — spanning 13.3 million UK adults — has uncovered a deeply troubling pattern: those who received common adult vaccines faced a significantly higher risk of both dementia and Alzheimer’s disease.
The risk intensifies with more doses, remains elevated for a full decade, and is strongest after influenza and pneumococcal vaccination. With each layer of statistical adjustment, the signal doesn’t fade — it becomes sharper, more consistent, and increasingly difficult to explain away.
And critically, these associations persisted even after adjusting for an unusually wide range of potential confounders, including age, sex, socioeconomic status, BMI, smoking, alcohol-related disorders, hypertension, atrial fibrillation, heart failure, coronary artery disease, stroke/TIA, peripheral vascular disease, diabetes, chronic kidney and liver disease, depression, epilepsy, Parkinson’s disease, cancer, traumatic brain injury, hypothyroidism, osteoporosis, and dozens of medications ranging from NSAIDs and opioids to statins, antiplatelets, immunosuppressants, and antidepressants.
Even after controlling for this extensive list, the elevated risks remained strong and remarkably stable.
Vaccinated Adults Had a 38% Higher Risk of Dementia
The primary adjusted model showed that adults receiving common adult vaccines (influenza, pneumococcal, shingles, tetanus, diphtheria, pertussis) had a:
38% increased risk of developing dementia (OR 1.38)
This alone dismantles the narrative of “vaccines protect the brain,” but the deeper findings are far worse.
Alzheimer’s Disease Risk Is Even Higher — 50% Increased Risk
Buried in the supplemental tables is a more shocking result: when the authors restricted analyses to Alzheimer’s disease specifically, the association grew even stronger.
50% increased risk of Alzheimer’s (Adjusted OR 1.50)
This indicates the effect is not random. The association intensifies for the most devastating subtype of dementia.
Clear Dose–Response Pattern: More Vaccines = Higher Risk
 |
The authors ran multiple dose–response models, and every one of them shows the same pattern:
Dementia (all types)
From eTable 2:
- 1 vaccine dose → Adjusted OR 1.26 (26% higher risk)
- 2–3 doses → Adjusted OR 1.32 (32% higher risk)
- 4–7 doses → Adjusted OR 1.42 (42% higher risk)
- 8–12 doses → Adjusted OR 1.50 (50% higher risk)
- ≥13 doses → Adjusted OR 1.55 (55% higher risk)
Alzheimer’s Disease (AD) Shows the Same—and Even Stronger—Trend
From eTable 7:
- 1 dose → Adjusted OR 1.32 (32% higher risk)
- 2–3 doses → Adjusted OR 1.41 (41% higher risk)
- ≥4 doses → Adjusted OR 1.61 (61% higher risk)
This is one of the most powerful and unmistakable signals in epidemiology.
Time–Response Curve: Risk Peaks Soon After Vaccination and Remains Elevated for Years
 |
Another signal strongly inconsistent with mere bias: a time-response relationship.
The highest dementia risk occurs 2–4.9 years after vaccination (Adjusted OR 1.56). The risk then slowly attenuates but never returns to baseline, remaining elevated across all time windows.
After 12.5 years, the risk is still meaningfully elevated (Adjusted OR 1.28) — a persistence incompatible with short-term “detection bias” and suggestive of a long-lasting biological impact.
This pattern is what you expect from a biological trigger with long-latency neuroinflammatory or neurodegenerative consequences.
Even After a 10-Year Lag, the Increased Risk Does Not Disappear
When the authors apply a long 10-year lag — meant to eliminate early detection bias — the elevated risk persists:
- Dementia: OR 1.20
- Alzheimer’s: OR 1.26
If this were simply “people who see doctors more often get diagnosed earlier,” the association should disappear under long lag correction.
Influenza and Pneumococcal Vaccines Drive the Signal
Two vaccines show particularly strong associations:
Influenza vaccine
- Dementia: OR 1.39 → 39% higher risk
- Alzheimer’s: OR 1.49 → 49% higher risk
Pneumococcal vaccine
- Dementia: OR 1.12 → 12% higher risk
- Alzheimer’s: OR 1.15 → 15% higher risk
And again, both exhibit dose–response escalation — the hallmark pattern of a genuine exposure–outcome relationship.
Taken together, the findings across primary, supplemental, dose–response, time–response, stratified, and sensitivity analyses paint the same picture:
• A consistent association between cumulative vaccination and increased dementia risk
• A stronger association for Alzheimer’s than for general dementia
• A dose–response effect — more vaccines, higher risk
• A time–response effect — risk peaks after exposure and persists long-term
• Influenza and pneumococcal vaccines strongly drive the signal
• The association remains after 10-year lag correction and active comparator controls
This is what a robust epidemiologic signal looks like.
In the largest single study ever conducted on vaccines and dementia, common adult vaccinations were associated with a 38% higher risk of dementia and a 50% higher risk of Alzheimer’s disease. The risk increases with more doses, persists for a decade, and is strongest for influenza and pneumococcal vaccines.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


After unnecessary hepatitis B vaccine dropped for 3.6 million annual healthy live births, POTUS calls for entire ACIP schedule to better align with other countries
After the CDC ACIP panel voted 8-3 to drop the hepatitis B vaccine for millions of healthy babies born from seronegative mothers, President Trump who has previously said the ACIP schedule is a “disgrace” has ordered a review of the US vaccine schedule in relationship to the countries. Alter AI assisted in this review.
 |
Based on the 2025 immunization schedules published by health authorities worldwide — including the CDC/ACIP (U.S.), Public Health England/UKHSA, Health Canada, Australia’s Department of Health, and the EU’s national public health programs — there are significant differences in how intensively children are vaccinated from birth to age 18.
Although all developed countries recommend broadly similar vaccines (targeting diphtheria, measles, polio, etc.), the United States stands at the top in total injections and doses, followed by Canada, France/Germany, the UK, Australia, Sweden, and Japan.
 United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
The 2025 CDC/ACIP schedule (see CDC PDF schedule, 2025) remains the most aggressive among Western nations.
By age one, a typical American baby receives 20+ doses spanning nine diseases (Hepatitis B, Rotavirus, DTaP, Hib, Pneumococcal, Polio, COVID‑19, Influenza, RSV). By age two, 32 individual antigens including monoclonal antibodies have been received in utero and after birth.
By age six, most children have accumulated around 27 to 29 doses, and around 30–32 total doses by age 18 (including HPV, meningococcal, Tdap boosters, annual flu shots, and now COVID boosters). Doses include combination products, so the number of antigens is much greater approximately 72-93 depending on maternal injections and other factors.
The U.S. uniquely begins vaccination at birth with Hepatitis B (now restricted to ~25,000 seropositive/carrier mothers) and adds multiple annual vaccines regardless of local exposure risk. It also promotes simultaneous injection of up to six vaccines at once (“combination vaccines” or same-visit stacking), magnifying early childhood exposure to adjuvants and preservatives.
 Canada — ≈ 25–28 doses
Canada — ≈ 25–28 doses
Canada’s national and provincial schedules (see Health Canada) mirror the U.S., but some provinces delay or skip optional vaccines (like flu or COVID‑19 for healthy children). Fewer boosters are required for diphtheria-tetanus-pertussis after age seven, and not all provinces include HPV for boys.
Canada therefore averages 2–4 fewer total doses than the United States.
 France /
France /  Germany — ≈ 22–25 doses
Germany — ≈ 22–25 doses
European Union countries vary widely:
- France mandates 11 childhood vaccines (including Hep B and Hib), but does not recommend early COVID‑19 or influenza vaccination for all children.
- Germany (STIKO guidelines) offers a schedule very similar to the U.S. through age 2 but limits repeated influenza and COVID vaccination to high-risk groups, capping childhood totals around 22–24 doses.
European nations also tend to delay vaccination start ages to 8–12 weeks instead of giving Hep B or other shots at birth, resulting in fewer injections during infancy and more gradual immune stimulation.
 United Kingdom — ≈ 20–21 doses
United Kingdom — ≈ 20–21 doses
The UK’s NHS and UKHSA recommend a smaller, slower schedule than North America’s. Infants receive about 16–18 doses by age 5, increasing to 20–21 by age 18.
Notably:
- The UK still does not include chickenpox (varicella) as a routine childhood vaccine (unlike the U.S.).
- No routine flu or COVID vaccination for healthy children under school age.
- Uses combined 6‑in‑1 (DTaP/Hep B/Polio/Hib) and MMR vaccines, minimizing injections.
 Australia — ≈ 20 doses
Australia — ≈ 20 doses
Australia’s National Immunisation Program (NIP) mirrors the UK more closely than the U.S.
Infants start at 6–8 weeks, not at birth (Hep B exception). Only one influenza vaccine per year is recommended, and chickenpox is given later. No universal COVID vaccine for healthy under‑5s.
Total injections: about 20 by adulthood.
 Sweden /
Sweden /  Norway — ≈ 16–18 doses
Norway — ≈ 16–18 doses
Nordic countries follow some of the world’s most minimalist Western schedules:
- No routine chickenpox, no birth shots, no annual flu or COVID for healthy kids.
- Combined vaccines reduce needle count.
- Emphasis on fewer but spaced doses (e.g., 3‑dose DTaP schedule instead of 5).
Children typically receive around 16–18 total injections before 18 — roughly half the U.S. burden — without suffering higher rates of “vaccine‑preventable” illness, challenging the dogma that more vaccines equal better outcomes.
 Japan — ≈ 14–16 doses
Japan — ≈ 14–16 doses
Historically the most cautious industrialized nation, Japan delayed and later reduced its vaccine schedule after serious adverse events in the 1990s.
Although it now recommends many standard vaccines, lower frequency, single-antigen use, and minimal early‑life stacking mean the total doses remain lowest in the developed world, around 14–16 through adolescence.
Japan’s infant mortality and autism rates are lower than in the U.S., prompting renewed scientific interest in whether slower schedules might lower iatrogenic risk.
 Summary — Total Vaccine Doses (Ages 0–18 Years)
Summary — Total Vaccine Doses (Ages 0–18 Years)
Rank Country Approx. cumulative doses Notes on schedule intensity 1 United States 30–32 Most intensive; starts at birth; annual flu + COVID 2 Canada 25–28 Slightly milder than U.S.; fewer mandatory boosters 3 France / Germany 22–25 Similar core vaccines; delayed start; selective flu use 4 United Kingdom 20–21 No varicella or universal flu/COVID; efficient combinations 5 Australia ≈ 20 Spaced schedule; limited COVID coverage 6 Sweden / Norway 16–18 Simplified; no birth or seasonal routine vaccines 7 Japan 14–16 Most delayed; minimal birth and combination doses
 Interpretation
Interpretation
The data show a clear gradient: the United States vaccinates children more frequently and at earlier ages than any other Western nation, often stacking combinations before immune maturity. Nations with slower, smaller schedules — Sweden and Japan most notably — maintain equal or superior child health metrics, casting doubt on the premise that maximal dosing guarantees better outcomes.
The U.S. model prioritizes population‑wide compliance and theoretical herd immunity, while Europe and Japan incorporate a more individualized risk‑based approach. Given the expanding scientific literature on rising childhood allergic and neuropsychiatric illnesses, these cross‑national differences underscore the need for independent, transparent studies comparing long‑term health outcomes by cumulative vaccine burden — something major regulatory agencies have conspicuously avoided.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Please subscribe to FOCAL POINTS as a paying ($5 monthly) or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH

Media bound to pay the price for selling their freedom to (selectively) offend

Sometimes An Ingrate Nation Pt. 2: The Great One Makes His Choice

Recent price declines don’t solve Toronto’s housing affordability crisis

From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
Business2 days ago
Recent price declines don’t solve Toronto’s housing affordability crisis
-
MAiD17 hours ago
From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
 MAiD2 days ago
MAiD2 days agoHealth Canada report finds euthanasia now accounts for over 5% of deaths nationwide
-
 Daily Caller2 days ago
Daily Caller2 days agoTech Mogul Gives $6 Billion To 25 Million Kids To Boost Trump Investment Accounts
-
 Automotive1 day ago
Automotive1 day agoPower Struggle: Governments start quietly backing away from EV mandates
-
 Energy2 days ago
Energy2 days agoUnceded is uncertain
-
 Business15 hours ago
Business15 hours agoCarney government should privatize airports—then open airline industry to competition
-
 Business1 day ago
Business1 day agoNew Chevy ad celebrates marriage, raising children