Health
The new WHO Pandemic Treaty poses grave threats to freedom and national sovereignty

From LifeSiteNews
The Pandemic Treaty will likely lead to dangerous lab leaks, digitals IDs, censorship, and other threats – and it will still affect the US even after leaving the WHO.
Does the passage of the WHO Pandemic Agreement on May 20, 2025, create the framework to usher in a new era of globalist control, masquerading as health care? Even though the United States and Argentina have withdrawn from the WHO, will we nevertheless be affected by its machinations? These questions are of critical concern. Here are six paramount threats posed by the new Treaty.
- National Sovereignty. This treaty represents a threat to national sovereignty by establishing an unelected, unaccountable globalist organization at the helm of international health care policy and implementation, “[r]ecognizing that the World Health Organization is the directing and coordinating authority on international health work …” (Preamble, emphasis added). The treaty further expands the WHO’s purview not only to exercising its authority during actual pandemics, but also during potential pandemics (Article 1 (C)) and during the times between pandemics (Article 2(2)) – in other words, at all times, in perpetuity. Further, nations are expected to amend their domestic legal and regulatory frameworks in alignment with the Treaty, further eroding national sovereignty. (Article 8; Article 11 (6)
- Censorship. The Treaty requires nations to “prevent misinformation [and] disinformation.” (Preamble, page 6). “Misinformation and disinformation” are not defined in the Treaty, but we can discern what it will mean from the WHO’s behavior during the COVID-19 outbreak. Hence, preventing “misinformation and disinformation” will likely include censoring any information that differs from the official WHO narrative, even if true: for example, dissenting voices stating that the COVID-19 virus spreads via human-to-human transmission or that it emerged from a lab leak, which facts the WHO denied at the inception of the outbreak. How will governments “prevent” these dissenting voices except by surveillance and censorship? To do so would constitute a clear violation of the right to free speech. Restricting access to accurate data further subverts national sovereignty and personal medical freedom. How can nations or individuals make sovereign decisions over their medical affairs if they cannot access correct information?
- Digital IDs. The Treaty requires nations to endeavor to develop “national health information systems” utilizing “international data standards for interoperability” (Article 6 (3)), as well as “technical and digital health resources.” (Preamble). While digital health IDs are not specifically mentioned in the Treaty, the framework for these is set forth in the Amended International Health Regulations (Articles 35 and 36; Annex 6). WHO Director General Tedros Ghebreyesus announced the launch of the WHO-EU Global Health Certification Network on June 5, 2023. These digital health IDs may serve as the precursor to a broader digital ID. For a fuller expression of the proposed capacities of digital IDs, see this chart included in an article posted on the website of the World Economic Forum. This chart reveals that digital IDs may be required to access health care, open a bank account, buy and sell online, travel, access social media, file taxes, vote, collect government benefits, and to own a telecommunications device (such as a cell phone or laptop). Is the ultimate goal to set up a global biotech surveillance police state that could track citizens under the pretext of global health, similar to the China Social Credit System?
- One Health. The One Health Approach, “recognizing that the health of people is interconnected with animal health and the environment” (Article 5), including domestic animals (Introduction). This interconnectedness can lead to surveillance and control of virtually every aspect of life on earth. An article in The Lancet entitled “One Health: a call for ecological equity” states: “The consequences of this thinking entail a subtle but quite revolutionary shift of perspective: all life is equal, and of equal concern.” Are human lives really “equal and of equal concern” to the lives of cockroaches or crabgrass?
- Expedited Approval of Vaccines. The Treaty requires nations to “strengthen” domestic regulations in order to ensure that they have the “legal, financial and administrative frameworks” necessary to fast track the approval of vaccines and other medications, potentially short-circuiting important safety and testing protocols. (Article 8 – formerly Article 14).
- Pathogen Access and Benefit Sharing System. Perhaps most chilling, the Treaty sets up the Pathogen Access and Benefit Sharing System (PABS) to “promot[e] the rapid and timely sharing of ‘materials and sequence information on pathogens with pandemic potential.’” (Article 12). This system will concentrate all the world’s most deadly pathogens into the hands of unelected, unaccountable bureaucrats under the influence of the Chinese Communist Party and the pharmaceutical industry. The WHO may then share them with labs all over the world, ostensibly to develop vaccines, diagnostics, and other “treatments.”
The WHO and Switzerland have already established a partnership for a global “WHO Biohub System,” the purpose of which is “to create a fast and reliable system for sharing materials that could cause epidemics or pandemics.” This system poses a significant risk of escalating the chances of pandemics caused by lab leaks as well as bio-terrorist attacks. These in turn will greatly increase the profits of the pharmaceutical industry and will give governments so inclined the pretext to keep people under lockdown and deprive them of their constitutional rights.
It is concerning that the details of how this system will function – its “modalities, legal nature, terms and conditions and operational dimensions” are not in the Pandemic Treaty itself. Rather, these “shall be developed and agreed in an instrument … as an annex.” (Article 12 (2)). In other words, the heart of the PABS system – and arguably, of the Treaty itself – has been left undefined. The WHO has kicked this heavy can down the road.
That being said, under what authority did the WHO establish the WHO Biohub System? The Pandemic Treaty failed to make it to the floor for a vote at the May 2024 World Health Assembly. On June 13, 2024 – the date of the BioHub System press release – the Treaty, which is supposed to govern the PABS System, would not be adopted for almost a year, and the Annex to set forth the details still has not been negotiated. And yet, the WHO went right ahead and launched its BioHub System, doing what the PABS System is designed to do. Since the BioHub System preexists PABS, will it be governed by it? In the alternative, did the WHO commit an end-run around its member states, advancing the illusion that they will determine how PABS will be governed, when, in actuality, the WHO will do whatever it pleases, ultra vires, regardless of any Treaty or Annex?
Even though the U.S. and Argentina have withdrawn from the WHO, these nations will still be affected by the Pandemic Treaty – especially the constant stream of lab leaks that will likely result from the PABS system. Pandemics know no borders. We can also be affected by whatever travel restrictions may be imposed by other countries, consistent with the Treaty.
The Pandemic Treaty is dangerous on numerous fronts, and we need to continue to expose and oppose it, internationally. It is not a done deal. Even though the Treaty was adopted on May 20, 2025, it will not be open for signature until after the Annex articulating the details of the PABS system is also adopted – probably at the World Health Assembly in May of 2026. In addition, it will need to be ratified by at least 60 member nations. Therefore, failure either to come to agreement on the PABS annex or to reach 60 ratifications would stymie its entry into force.
Other nations should see the withdrawal of the U.S. from the WHO as a clarion call and consider taking similar action. We need a consortium of free nations collaborating to address global health concerns, without the interference of the irredeemably corrupt World Health Organization.
Treaty apologists point to Article 22 (2) to support the proposition that the Treaty will not affect national sovereignty. This section, however, is craftily worded and disingenuous. It pertains only to the Secretariat and the Director General, not to other WHO-related bodies, such as, for example, the Conference of the Parties, responsible for the “effective implementation” of the Treaty. (Article 19 (2)). Further, these apologists ignore the resounding impact that WHO pronouncements have on numerous governments, many of which follow WHO recommendations as though having the force of law.
Brock Chisholm, the first director general of the World Health Organization, once stated: “To achieve world government, it is necessary to remove from the minds of men their individualism, loyalty to family traditions, national patriotism, and religious dogmas.” Chisholm said the quiet part out loud. If “to achieve world government” was the goal of the first Director General of the WHO, then it would be naïve of us to believe that our national sovereignty and personal freedom are not at risk.
Take action by signing the Manifesto at Anti-Globalist International.
A graduate of Yale Law School, attorney Reggie Littlejohn is founder and president of Anti-Globalist International and Women’s Rights Without Frontiers. She is co-founder of the Sovereignty Coalition.




Looks like we made it. For another weekend at least. Until sanity settles down into the head into the head of the federal government that remains fixated on the killing of 399 healthy ostriches. As the clock wound down today, an announcement from the farm proclaimed, “We made it today,” calling it another “miracle Friday.”
WATCH TODAY’S Miracle Friday Announcement
Earlier in the day, Rebel News’ Drea Humphrey reported, “There’s apparently a SWAT team up the road, I hope that doesn’t mean they’ve gotten bad news,” wondering “if the police were preparing to aid the CFIA in the cull.”
 |
Dacey Media reported that the farm said that “Ostrich Hunters” were also spotted at Universal Ostrich Farms according to Katie Pasitney The “kill pen” is fully set up and CFIA have been luring ostriches into it.
But as of 5:30 ET, it seems the farm and the ostriches may have escaped to live another day as the Supreme Court of Canada (SCC) did not hand down a decision to grant a further leave to the farm to prepare its case, or dismiss the case, allowing the Canadian Food Inspection Agency (CFIA) to proceed with their “cull” to kill 399 healthy ostriches.
The palpable, raw government over-reach that includes over 100 Royal Canadian Mounted Police (RCMP) that have occupied the farm highlights the mismanagement of the CFIA and may be one of the reasons that the SCC has hesitated in making a decision before the weekend.
Call to Dismantle the CFIA
On today’s Stand on Guard interview Katie Pastiney, spokeswoman for the Universal Ostrich Farms in British Columbia called for the dismantlement of the Canadian Food Inspection Agency. She says that the CFIA:
“Needs to be dismantled and we need to rebuild this organization back up from the ground up and we need to have a new vision.
“We need to have a new mission and a brand-new face for Canadians that will give us hope that we will be protected not attacked.”
“The Canadian Food Inspection Agency continues to overuse their authority, overuse their excessive freedom that they’ve been given, and they have zero accountability for their actions.”
The farm has been embroiled in a dispute with the federal government and its CFIA agency for close to a year. The agency claims the flock of ostriches has the avian flu, but it refuses to test the farmers’ birds, even though they have been healthy for 258 days. At the same time the CFIA will not let the farmers pay for the tests themselves, saying they will charge them $250,000 per ostrich and put them in jail for 6 months.
 |
The federal agency and the RCMP have seized and occupied the farm since September 22, 2025. they have conducted a campaign of harassment of the farm family and their flock of ostriches that included: arresting the farmers when they were told to go feed their birds; using lights and heavy equipment at night’; sending drones to chase the birds that resulted in pushing one bird over the fence so it hurt its leg, not treating the animals properly; and not feeding the ostriches full rations of food and water and not treating the birds the CFIA injured. These activities have continued as the CFIA continues to construct a “kill box” of hay bales that have been on fire four times while under the CFIA’s supervision and occupation.
 |
Running Out of Time
In a stunning report on X October 2nd, however, before the Supreme Court of Canada had made decision, the CFIA has daily continued to move forward to kill the ostriches ignoring the SCC legal “stay.”
Karen Esperson, Pasitney’s mother yesterday reported on X:
“We need to put CFIA in check.
“This organization feels they are greater than the Supreme Court of Canada. they are still positioning the birds and putting them in the position to be killed immediately. They are assuming they know the outcome of the Supreme Court oof Canada. Do they think they are better than the Supreme court? That they are going to for sure win?
“The Supreme Court has not decided.
“What is happening?
“We are on a stay order and yet I just got a call that they have a whole bunch of birds herded in a little circle in the kill pen.
“Waiting. This is animal cruelty.”
 |
Efforts to Save the Ostriches
More and more Members of Parliament have been speaking up on behalf of the farmers including the local provincial representative, the local Member of Parliament Scott Anderson, who visited the farm trying to talk to the CFIA and also the Official Leader of the Opposition Pierre Poilievre spek out yesterday.
A second press conference hosted by John Catsimatidis, a New York radio host, billionaire and friend of Donald Trump and Dr. Oz, was also held yesterday. The USA Trump administration representatives including Robert F. Kennedy say they want to either pay for the ostrich testing or help re-locate them to the United States for further research opportunities. This outreach has been ignored.
CFIA Has Staff Enough to Kill but NOT Enough Staff to Test?
In my interview today with Pastiney she explained how the CFIA did originally give their ostrich farm an exemption that was later rescinded because the CFIA told them they were “understaffed and we’re not able to perform these tests.”
“There was an exemption package that was given to us on January 2nd. We have an email from Canadian Food Inspection Agency stating that we qualify for special rare genetics within our herd and that we could be exempt.
“Now when we followed through with that because we needed to test them just to show their DNA and their genetics and show their lineage that between January 2nd and January 10th something happened.
“Now we didn’t qualify we lost that right.
“And on January 10th they said sorry you don’t qualify for special rare genetics because we are understaffed and we’re not able to perform these tests.”
Why does the CFIA have staff to occupy the farm for weeks and to kill 399 ostriches as well as requisition the Royal Canadian Mounted Police (RCMP) over 40 cars and reportedly more than 100 police on the farm since September 22nd, and not have the money to test the birds for the exemption?
How much has this debacle and exercise into Carney Government overreach been charged to Canadian taxpayers?
 |
More than the tests to see if the ostriches are healthy or if they qualify for the exemption?
Other Farmers May Join in Efforts to Disband the CFIA
 |
Pastiney says:
“I just did an interview with a farmer that this very same thing happened to them and it was based off a suspicion of tuberculosis outbreak on their farm.
“They [the farmers] had over 600 head of cattle, they had sheep, they had goats, they had pig or pigs, they had chickens.
“They [the CFIA] came in based off suspicion and off their own negligence they killed everything this beautiful older farm had to find out in the end that they tested after everything was dead and there was no tuberculosis.”
“I asked her a very important question, and I said could you trust this organization again? And she said, absolutely not.
“So, it became very clear to me after this about talking to two or three farmers that the Canadian Food Inspection Agency needs to be dismantled.”
“It is an organization that has lost the trust of Canadians.
CONCLUSION
WATCH Katie is Fighting For Everyone’s Freedom | Stand on Guard

www.kraydensrightnews.com is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.

From LifeSiteNews
Roger Foley has been pressured to consider euthanasia while being denied adequate care, prompting a new campaign to cover his medical costs and support his fight to return home.
Roger Foley, an Ontario man, has been forced to turn to charity after being denied sufficient care from hospitals which continue to push euthanasia on him.
On September 30, the Life Care Network launched a LifeFunder to cover medical costs for Roger Foley, a disabled Canadian who is struggling to receive support in an Ontario hospital which is encouraging him to end his life with Medical Assistance in Dying (MAiD).
“Hospital staff have repeatedly offered and pressured me to consider Canada’s infamous assisted suicide program Medical Assistance in Dying (MAiD) while simultaneously obstructing the very services and supports I need to live safely,” Foley revealed in a write-up for the fundraiser.
“Despite my condition, I have fought tirelessly for my rights, dignity, and the ability to return to the community,” he continued.
Foley, who is well known for speaking out against the injustice of Canada’s euthanasia regime, suffers from spinocerebellar ataxia, an incurable brain disease that makes it difficult to move.
As a result of his, he requires caregivers to assist him in eating, drinking, and getting up. According to Foley, his caregivers mistreated him while caring for him at his home. In 2016, Foley was admitted to the London Health Sciences Centre (LHSC) in Ontario for food poisoning and has been there ever since.
Foley revealed that over the past nine years he has repeatedly been offered MAiD despite his desire to be released from the hospital and return home with the help of caregivers.
In May, Foley began enduring even more pain when the LHSC switched out the amber lights in his room for bright bulbs. Foley, who is light sensitive, is now in so much pain that he is unable to be lifted for meals.
“I can only tolerate fluids for a few minutes at a time using makeshift taped-together ski goggles. I am unable to eat solid food or take oral medications,” Foley explained.
“I live in constant pain, severe fatigue, and cognitive decline from dehydration and lack of sleep,” he continued. “Staff continue to impose arbitrary and unsafe ‘rules,’ including denying me side rails during transfers and barging in with bright lights – despite knowing it causes me extreme harm.”
Now Foley is seeking private funding for a Personal Support Worker to assist him with feeding, medication, hydration, and basic hygiene support. Life Care Network, an organization which assists vulnerable Canadians at risk for MAiD, has intervened to raise the necessary funds for Foley’s care.
In an interview with LifeSiteNews, Lino DeFacendis, founder and CEO of Life Care Network, stressed the importance of defending Foley from a medical system which appears to prioritize ending his life with MAiD over providing proper care.
“There needs to be a re-awakening that every life is precious and must be treated with true dignity and compassion no matter how difficult the circumstance,” DeFacendis said.
“Killing oneself via MAiD is never the answer to one’s problems,” he declared.
To support Foley’s medical care, please visit his LifeFunder page.



Taxpayers: Alberta must scrap its industrial carbon tax

$150 a week from the Province to help families with students 12 and under if teachers go on strike next week

Can Sugar Rush 1000 Satisfy Your Sweet Tooth for Wins?
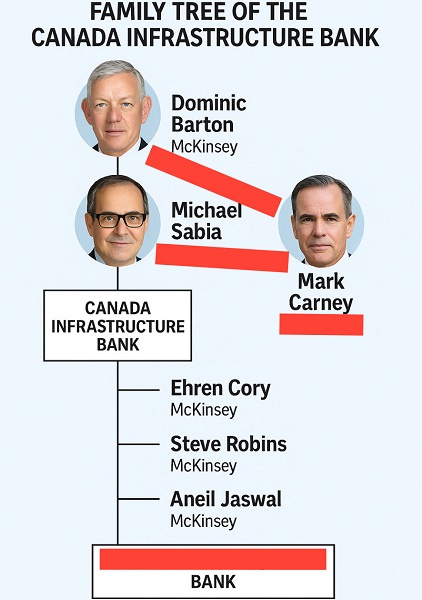
Dominic Barton’s Shadow Over $1-Billion PRC Ferry Deal: An Investigative Op-Ed


-
 Alberta2 days ago
Alberta2 days agoAlberta’s E3 Lithium delivers first battery-grade lithium carbonate
-
 Artificial Intelligence2 days ago
Artificial Intelligence2 days agoAI chatbots a child safety risk, parental groups report
-
 Business2 days ago
Business2 days agoLA skyscrapers for homeless could cost federal taxpayers over $1 billion
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoHurting someone’s feelings could be punishable under Canadian hate crime bill: legal expert
-
 Energy2 days ago
Energy2 days agoNuclear power outperforms renewables every time
-
 Automotive2 days ago
Automotive2 days agoCanada’s EV subsidies are wracking up billions in losses for taxpayers, and not just in the auto industry
-
 Crime1 day ago
Crime1 day agoThe “Strong Borders Act,” Misses the Mark — Only Deep Legal Reforms Will Confront Canada’s Fentanyl Networks
-
 Business1 day ago
Business1 day agoUK Government Dismisses Public Outcry, Pushes Ahead with Controversial Digital ID Plan