COVID-19
Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal


 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
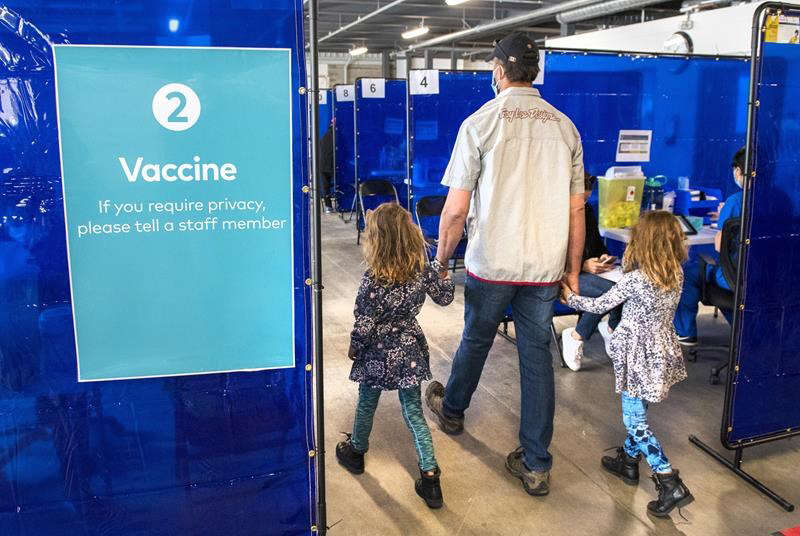
45.3% of “COVID-19 deaths” in Greece had no symptoms — exposing the coordinated PSYOP deployed to maximize fear and enforce mass compliance with draconian control measures.
The study titled “Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece” was just published in the journal Scientific Reports:
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19. In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
 |
Key Findings:
Massive Overcounting of COVID-19 Deaths
- Out of 530 hospital deaths registered as COVID-19 deaths, only 290 (54.7%) were actually caused by COVID-19.
- 240 deaths (45.3%) were found to be completely unrelated to COVID-19 — patients died with a positive PCR test, but showed no symptoms, required no COVID-specific treatment, and died of clearly unrelated causes.
Death Certificate Inaccuracy
- Of the 204 certificates listing COVID-19 as the direct cause of death, only 132 (64.7%) were confirmed as such after clinical review.
- Of the 324 certificates listing COVID-19 as a contributing factor, only 86 (26.5%) were found to be truly related.
Hospital-Acquired Infections Misclassified
- Patients infected during hospitalization were significantly more likely to be misclassified as COVID-19 deaths (OR: 2.3, p = 0.001).
Younger Age and Severe Comorbidities Associated with Misclassification
- Patients who died “with” COVID-19 were younger, more likely to be immunosuppressed, have end-stage liver disease, or be admitted for other causes.
Symptoms and Treatments Differed Sharply
Patients who died “due to” COVID-19 were more likely to:
- Exhibit classic symptoms: hypoxia (44.1%), shortness of breath, fever, and cough
- Require oxygen support (93.4% vs. 66.9%) and receive COVID-specific therapies:
- Remdesivir (5-day course: 61.9% vs. 35.2%)
- Dexamethasone (81.7% vs. 40.7%)
Study Strengths
This study went far beyond death certificate coding, implementing a rigorous, multi-source clinical audit:
- Full medical chart reviews: Included physician notes, lab data, imaging, and treatment records.
- Attending physician interviews: Structured questionnaires captured real-time clinical insights from those who treated the patients.
- Dual independent expert assessments: Two experienced infectious disease specialists (each with >2,500 COVID cases) reviewed each case independently for classification accuracy.
This study found that nearly half of all registered COVID-19 deaths during the Omicron wave in Greece were misclassified, with no clinical evidence linking them to COVID-19 as the true cause. Given that similar death coding practices were employed across Western nations, it is reasonable to conclude that COVID-19 death counts were artificially inflated to a comparable degree elsewhere.
This drastic inflation of death counts aligns with what many now understand to be a coordinated psychological operation (PSYOP)—designed to instill fear and maximize compliance with draconian pandemic measures such as lockdowns, mask mandates, and mass mRNA injection campaigns.
It is this weaponization of fear that has prompted criminal referrals in seven U.S. states, triggering active criminal investigations into top COVID-19 officials for terrorism, murder and racketeering:
BREAKING – The Pandemic Justice Phase Begins as Criminal Investigations Commence |
||||||
|
||||||
 |
||||||
|
By Nicolas Hulscher, MPH
|
||||||
|
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
COVID-19
A new study proves, yet again, that the mRNA Covid jabs should NEVER have been approved for young people.

2.7 million Spanish children and teenagers. ZERO Covid deaths.
Here’s some news from Spanish researchers: contrary to what American health bureaucrats said for years to justify the increasingly insane mRNA “vaccine” experiment, Covid doesn’t kill kids.
—
(More facts, fewer guesses. For pennies a day.)
—
Yes, making categorical statements like “Covid doesn’t kill kids” is foolish.
Look hard enough, and there will be an exception, perhaps a child terminally ill with cancer pushed over the edge by Covid.
But the Spanish study, which was peer-reviewed and published in The Pediatric Infectious Disease Journal, proves yet again that Covid’s risk is too low to measure — not just not to healthy children, but to all children. It is the strongest evidence yet that the oft-repeated claim that Covid has killed 2,100 American children is fiction.¹
The researchers examined medical records from 2.7 million Spanish children and teenagers from mid-2021 through the end of 2022, a period in which the Omicron variant infected almost everyone worldwide with Covid. The vast majority of those kids and adolescents, about 2.2 million, had not been vaccinated.
Yet none of those 2.7 million died of Covid.
None. As in zero.
—
(Good thing we closed the schools!)
 |
(SOURCE)
—
There really isn’t much more to say about the paper, except that the authors couldn’t find any difference for Covid hospitalization rates between vaccinated and unvaccinated kids under 12.
For adolescents 12-17, they calculated about 38,000 mRNA jabs were required to avoid one Covid hospitalization — an absurdly high number given the known short-term side effects of the shots and the potential long-term risks of exposing young people to mRNA.
At this point, any physician who recommends Covid jabs for kids (as a handful, mostly in blue states, still are) should be sued for malpractice.
—
One final note: this week’s immigration articles have gotten a LOT of likes and comments, more than any recent Covid or mRNA pieces. More new subscribers too.
I expect that will be true again today, though I hope you’ll prove me wrong. I understand. We all have moved on.
But when studies like this new one come out, covering them is crucial.
Nearly 1.5 billion people received mRNA Covid jabs worldwide, including perhaps 100 million kids and teenagers in the United States, Canada, Japan, Europe, and elsewhere. And the American public health establishment and legacy media outlets continue to push mRNA on children and fight even modest efforts to tighten restrictions on mRNA Covid jabs.
Witness the furious pushback Food and Drug Administration chief medical officer Dr. Vinay Prasad received in late November after he reported FDA reviewers found Covid shots had killed children.
So, even as I write about immigration, healthcare fraud, and other topics vital to you, I believe I have a duty to continue to update the factual record about the mRNAs. Duty is not too strong a word. In June 2023, I covered a paper from South Korean researchers about cardiac deaths of young adults who had received the mRNA jabs.
It is no exaggeration to say no one else — no other journalist or scientist covering Covid or the jabs — paid attention to that paper at the time . But now, in the wake of Prasad’s bombshell memo, I’ve again raised that paper. Even the mRNA fanatics at the Atlantic have been forced to acknowledge it.
It’s impossible to know if these articles will matter today, tomorrow, or years from now. But as long as the mRNA companies and their public health handmaidens keep pushing this troubled technology, I’ll keep trying to build the most complete possible record.
—
(And I hope you will support me.)
(More facts, fewer guesses. For pennies a day.)
That 2,100 death figure, which the American Academy of Pediatrics loves to quote, appears to come from a 2023 paper from the National Academy of Medicine paper that in turn relies on Centers for Disease Control data. But the CDC figures no distinction between “with” and “from” Covid deaths, which are particularly important in groups at low baseline risk from Covid. Further, the fact that the number hasn’t been updated in almost three years suggests that the people quoting it know it’s nonsense and don’t want to double-check it, much less try to update it.
What, kids just stopped dying from Covid in 2023 after getting mowed down during the first three years of the epidemic?
|
|||
|
|||||
|
|||||
| Independent, citizen-funded journalism |

From LifeSiteNews
A judge ruled that the Ontario Court of Justice is already ‘satisfied’ with Chris Barber’s sentence and taking away his very livelihood would be ‘disproportionate.’
A Canadian judge has dismissed a demand from Canadian government lawyers to seize Freedom Convoy leader Chris Barber’s “Big Red” semi-truck.
On Friday, Ontario Court of Justice Judge Heather Perkins-McVey denied the Crown’s application seeking to forfeit Barber’s truck.
She ruled that the court is already “satisfied” with Barber’s sentence and taking away his very livelihood would be “disproportionate.”
“This truck is my livelihood,” said Barber in a press release sent to LifeSiteNews.
“Trying to permanently seize it for peacefully protesting was wrong, and I’m relieved the court refused to allow that to happen,” he added.
Criminal defense lawyer Marwa Racha Younes was welcoming of the ruling as well, stating, “We find it was the right decision in the circumstances and are happy with the outcome.”
John Carpay, president of the Justice Centre for Constitutional Freedoms (JCCF), said the decision is “good news for all Canadians who cherish their Charter freedom to assemble peacefully.”
READ: Freedom Convoy protester appeals after judge dismissed challenge to frozen bank accounts
“Asset forfeiture is an extraordinary power, and it must not be used to punish Canadians for participating in peaceful protest,” he added in the press release.
As reported recently by LifeSiteNews, the Canadian government claimed that Barber’s truck is an “offence-related property” relating to his involvement in the 2022 protests against Canada’s COVID mandates.
At this time, the court ruling ends any forfeiture proceedings for the time being, however Barber will continue to try and appeal his criminal conviction and house arrest sentence.
Barber’s truck, a 2004 Kenworth long-haul he uses for business, was a focal point in the 2022 protests. He drove it to Ottawa, where it was parked for an extended period of time, but he complied when officials asked him to move it.
On October 7, 2025, after a long trial, Ontario Court Justice Perkins-McVey sentenced Barber and Tamara Lich, the other Freedom Convoy leader, to 18 months’ house arrest. They had been declared guilty of mischief for their roles as leaders of the 2022 protest against COVID mandates, and as social media influencers.
Lich and Barber have filed appeals of their own against their house arrest sentences, arguing that the trial judge did not correctly apply the law on their mischief charges.
Government lawyers for the Crown have filed an appeal of the acquittals of Lich and Barber on intimidation charges.
The pair’s convictions came after a nearly two-year trial despite the nonviolent nature of the popular movement.

Georgia county admits illegally certifying 315k ballots in 2020 presidential election

Why Japan wants Western Canadian LNG

Sweden Fixed What Canada Won’t Even Name

Land use will be British Columbia’s biggest issue in 2026
-
 International2 days ago
International2 days ago“Captured and flown out”: Trump announces dramatic capture of Maduro
-
 International2 days ago
International2 days agoTrump Says U.S. Strike Captured Nicolás Maduro and Wife Cilia Flores; Bondi Says Couple Possessed Machine Guns
-
Energy2 days ago
The U.S. Just Removed a Dictator and Canada is Collateral Damage
-
 International2 days ago
International2 days agoUS Justice Department Accusing Maduro’s Inner Circle of a Narco-State Conspiracy
-
 Haultain Research1 day ago
Haultain Research1 day agoTrying to Defend Maduro’s Legitimacy
-
 Business2 days ago
Business2 days agoVacant Somali Daycares In Viral Videos Are Also Linked To $300 Million ‘Feeding Our Future’ Fraud
-
International2 days ago
U.S. Claims Western Hemispheric Domination, Denies Russia Security Interests On Its Own Border
-
 Daily Caller1 day ago
Daily Caller1 day agoTrump Says US Going To Run Venezuela After Nabbing Maduro