Health
DMSO Heals the Eyes and Transforms Ophthalmology


DMSO’s unique therapeutic properties reveal the unifying thread between many different “incurable” eye diseases.
Story at a Glance:
• DMSO is an “umbrella remedy” capable of treating a wide range of challenging ailments due to its combination of therapeutic properties (e.g., reducing inflammation, improving circulation, and reviving dying cells).
• DMSO has a unique affinity for the eyes, resulting in it (often spontaneously) treating a wide range of visual disorders that frequently cannot be treated with conventional therapeutic options.
• DMSO’s ability to restore circulation, revive dying cells, and stabilize misfolded proteins allows it to treat a variety of retinal diseases (e.g., macular degeneration, diabetic retinopathy or retinitis pigmentosa—in some cases reversing permanent blindness), eliminate visual obstructions (e.g., floaters and cataracts), reverse glaucoma or Fuchs’ dystrophy, and restore normal focus (frequently eliminating the need for glasses).
• DMSO’s anti-inflammatory and antimicrobial properties allow it to treat dry eyes, inflammatory diseases around the eye (e.g., blepharitis, styes, and psoriasis) or within the eye (e.g., iritis, uveitis, conjunctivitis, keratitis), along with bacterial, fungal, parasitic, or viral eye infections such as shingles.
•DMSO’s healing properties also allow it to heal a variety of eye injuries (including severe ones which would otherwise require eye removal), skin issues around the eye (e.g., burns, skin tags, and under-eye bags), and eliminate eye muscle spasms.
•This article will review the extensive data demonstrating DMSO’s efficacy for eye diseases, along with an examination of the most common protocols used for them and other natural approaches that also aid in the treatment of common eye disorders.
Since 2024, I have been working diligently to present the extensive data that DMSO is a remarkable therapeutic that is uniquely suited to treat many highly challenging medical conditions due to its counteracting many root causes of disease (whereas, in contrast, vaccines cause a myriad of health issues by inducing those key drivers of illness). From this, I’ve compiled a series of articles synthesizing thousands of studies that have shown DMSO effectively treats:
- Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
- A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
- Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
- A wide range of autoimmune, protein, and contractile disorders, such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
- A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
- A wide range of internal organ diseases (discussed here).
- Many different respiratory disorders, including asthma and COPD (discussed here)
- Many different gastrointestinal disorders, such as bowel inflammation, cirrhosis, and pancreatitis (discussed here)
- A wide range of skin conditions, such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
- Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
- Many aspects of cancer (e.g., many of cancer’s debilitating symptoms, making cancer treatments more potent, greatly reducing the toxicity of conventional therapies, and turning cancer cells back into normal cells), which I discussed here.
Since the evidence in those articles (along with one on how DMSO can be synergistically combined with pharmaceuticals and another on how DMSO combines with natural therapies) made a compelling case for the use of DMSO, many readers opted to start using it. Many of them, in turn, had remarkable improvements which caused them to recommend DMSO to their peers, and because of all those successes, a widespread interest in DMSO has now emerged.
On one hand, this has been quite surprising to me as the information I publicized has been widely available for decades, but (possibly due to it being impossible to profit off DMSO because of how little it costs) most of the people exposed to this series were not even aware this therapy existed, let alone what DMSO could do. Conversely, the groundswell of interest is not surprising as it’s nearly identical to what happened when DMSO was first discovered in the 1960s and it rapidly became the most popular drug in America—particularly since relatively minimal progress has been made on most of the “incurable” conditions it cured back then. Consider for example this 1980 segment 60 minutes created, which showed the remarkable results generated from the therapeutic use of DMSO and more importantly, the exact same stonewalling and suppression of DMSO from the FDA that we saw throughout COVID-19:
User DMSO Reports
Because of DMSO’s high degree of efficacy, the moment I began the series, I started being flooded with testimonials from readers of the remarkable improvements DMSO had created for them. Before long, I realized I was in a similar situation to what I’d been in throughout COVID-19.
I have long believed one of the core strategies the ruling class always follows is to establish rigid hierarchical systems that have dominion over critical facets of society and then buy out the top of the pyramid, as that provides a relatively low-cost way to control the entire society. In the case of medicine, this has translated to having pharmaceutical compliant individuals (through industry funding and media complicity) be anointed as experts who reinforce the profitable orthodoxy alongside having medical journals only publish things which cater to the existing vested interests.
Because of this, things that are “controversial” (threatening vested interests) are rarely published in a “credible” medium, and as a result, anyone who tries to advocate for them is not listened to; instead, they are chastised for endorsing “unproven” and unscientific beliefs.
When the COVID vaccines hit the market, I had expected they would cause a significant number of chronic issues that would take years to be recognized—so I was quite shocked to be immediately flooded with reports across the country of severe reactions of all types from the vaccine. Because of this, I felt I needed to log them as I knew injuries like these would never get published in medical journals and I wanted to have some type of proof that vaccine injuries were real, so in the future I could present accurate information to skeptical parties. I hence spent an inordinate amount of time interviewing those involved and compiling all of them and after unexpectedly gaining a Substack audience, I published that log, and it went viral because my small sample accurately represented the pattern of vaccine injuries everyone was seeing around them and because more than a year into the COVID vaccine rollout, no one had done anything similar—despite the massive demand for this type of information.

In the process of doing that, I had also received a lot of reports of individuals who appeared to be being injured by COVID vaccine shedding—despite this being “impossible” based on the purported design of the vaccines. As the reports, like those for the COVID-19 vaccine injuries, were consistent in character (and like the vaccines many affected by shedding were understandably desperate for information on the topic) I decided to spend a year compiling thousands of those reports as I knew there would never be a journal willing to touch the subject. Following this, I then produced a synthesis of that data which showed there were clear repeating patterns to mRNA shedding and provided the critical mechanisms to explain this seemingly inexplicable phenomenon. That, in turn, was an inordinate amount of work to do, but succeeded and made many realize shedding is a real risk of the mRNA technology—something which will be critical for opposing future attempts to inject the population with experimental gene therapies.
In the case of DMSO, as I started receiving all of these reports (at a time when I had essentially finished the shedding project), I realized that I had access to a unique dataset that had not previously been available. More importantly, because there were so many different things that DMSO could treat, a dataset like this would likely be the only place much of that therapeutic data could ever be compiled (as no one would ever get around to conducting studies on many of those uses—particularly since the current academic publishing climate is much more hostile to publishing unorthodox research now than it was fifty years ago).
So, over the last 13 months, one of my primary projects has been to compile all the reports I’ve received (which I did in the comments here), and I presently have 4,721 comments—of which I think roughly 3,000 are unique stories of therapeutic benefit people have experienced. In turn, my plan is to eventually compile and synthesize all of that, but as doing that will take at least a month, I’ve held off until the end of the series (so I wouldn’t have to redo it with new data that was subsequently received).
Note: my general sense from all the testimonials I’ve received is that between 80-90% of users have a positive response to using DMSO (which is frankly extraordinary), with lower rates (50%) being seen for certain issues which are harder to correctly treat with DMSO, and give or take 0% success rates being seen for issues DMSO is not thought to treat (suggesting the sample I’m observing is representative of real life data).
Within those comments, while most of the reports I’ve received are consistent with what DMSO is recognized to do (e.g., rapidly eliminating debilitating pain that nothing else had worked on), some were quite extraordinary and not what I’d expected to come across. For example, after I learned a 75 year old reader who’d been blind since birth had regained their sight after using DMSO to treat a sinus issue, I realized his story needed to be shared:
Note: as fate had it, Murray lived about 3 hours away from Rebecca Cunningham, the Texas-based documentary film maker who cured her neighbor’s terminal COPD with nebulized DMSO, after which millions saw Dan’s COPD story.1,2 As DMSO changed her life, she is currently collecting other DMSO testimonials on her Rumble channel and kindly agreed to travel to Murray to film this. If you have a story to share and are ever passing through Wimberley or visiting the hill country in Texas, please reach out to her.
In compiling these reports, I was struck by how many were for the eyes, by how well DMSO worked across an extensive range of eye conditions, and by the fact that, in the majority of cases, it provided better results than could be expected from existing ophthalmology options.
Note: the only well-recognized ophthalmologic conditions I did not receive reports on were amblyopia, strabismus, diabetic retinopathy, keratitis, optic neuritis, retinal detachment, retinopathy of prematurity, chalazions, central retinal vein occlusion (although a reader’s branched retinal vein occlusion responded to DMSO), and eye cancers—many of which, as I will show in this article, existing data sources suggest do respond to DMSO.
Later, while translating the discoveries of the German community, I learned their data matched that of the readers here:
One of the first new adopters of DMSO (circa 2012), began successfully using highly diluted DMSO for eye treatments in his practice. This led to a network of practitioners using DMSO for eye health, accumulating substantial experience, and, in many cases, treating eye issues where the cause could not be determined.
In general, there are a surprising number of successful reports using DMSO eye drops for a wide variety of eye symptoms and diseases. So many, in fact, that I now consider the DMSO eye solution an exceptional “eye care.”
Many users (especially those with heavy screen time) apply DMSO preventively to maintain eye freshness, improve tear quality, and reduce night glare. Positive effects, including improved vision, better tear film, fresher eyes, and reduced night glare, are often reported after the first few applications, enhancing overall eye comfort and function—including in people whom ophthalmologists did not diagnose with any eye conditions.
The positive effects are often reported after the first few applications, but I consider [low dose eye drops] a longer-term option. Due to the excellent diagnostic results and the complete absence of adverse effects from low dose drops (including results from ophthalmologists for a wide range of eye disorders) I increasingly view DMSO eye drops as a preventative measure, eye care for those with (still) healthy eyes, since modern life, particularly excessive screen time, places significant demands on our eyes.
Note: the above was extracted from an AI-generated summary of hundreds of hours of non-English lectures, then further condensed by me and hence not a direct quote (but one that accurately represents the author’s statements).
While this might be difficult to believe, consider a parallel situation. Another umbrella remedy I have been deeply impressed by, ultraviolet blood irradiation (which has many similar therapeutic properties to DMSO), has a vast volume of literature demonstrating its clinical value—including for numerous immensely challenging to treat diseases. Yet, virtually none of the medical profession even knows this therapy exists.
For this reason, we are currently sorting through thousands of UVBI studies, including dozens of studies (many of which were conducted with hundreds of patients) which show UVBI treats a myriad of challenging ophthalmologic conditions such as:
blepharitis,1 keratitis,1 corneal inflammation,1 herpes zoster ophthalmicus,1 traumatic eye infection,1 uveitis,1,2,3,4,5 iridocyclitis,1,2 choroiditis,1 chorioretinopathy,1,2,3,4 choroidal and chorioretinal dystrophy,1,2 macular degeneration,1 retinitis pigmentosa,1,2 retinal contusion,1 retinal ischemia,1,2 retinal and fundus hemorrhages,1,2,3,4 retinal artery and vein occlusions,1,2,3,4,5,6,7,8,9,1
0,11,12,13,14,15 diabetic retinopathy,1 ischemic optic neuropathy,1,2,3,4,5 optic neuritis,1,2,3 optic nerve atrophy (traumatic or inflammatory),1,2,3 encephalopathic vision loss1
Note: in this article, each superscipt number links to either a reader’s story or an applicable study—like the many I listed above (which the ophthalmology profession does not realize exists).
As such, the purpose of this article will be to highlight exactly how DMSO is transforming ophthalmology, along with the supporting data.
The Forgotten Side of Medicine is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
To learn more about this newsletter and how others have benefitted from it, click here!
Note: the best review paper on DMSO’s uses in ophthalmology (which is an excellent resource to provide to physicians who are skeptical of using DMSO for the eyes) can be read here.


ACIP voted to un-recommend the Hep B birth dose, but here’s the problem: they still can’t weigh the other side of the ledger
Sunday, something happened that has never happened in the history of American public health: ACIP voted 8-3 to un-recommend the universal birth dose of hepatitis B for babies born to mothers who test negative for the virus. After 34 years of jabbing every American newborn within hours of taking their first breath—regardless of whether their mother had hepatitis B—the committee finally acknowledged what 25 European countries figured out decades ago: it doesn’t make sense.
But watching this vote unfold, I couldn’t help but notice the absurdity of the debate itself. Committee members who opposed the change kept saying variations of the same thing: “We’ve heard ‘do no harm’ as a moral imperative. We are doing harm by changing this wording.” Another said “no rational science has been presented” to support the change.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
And therein lies the fundamental problem with ACIP—and with the entire vaccine regulatory apparatus in America. They literally cannot weigh risk versus benefit because they only have data on one side of the scale.
The Missing Side of the Ledger
When ACIP debates adding or removing a vaccine from the schedule, they can produce endless data on disease incidence. They can show you charts demonstrating how hepatitis B cases in infants dropped from thousands to single digits after 1991. They can model projected infections if vaccination rates decline. They have this data at their fingertips because tracking infectious disease is something our public health apparatus actually does.
But ask them to produce equivalent data on vaccine injury, and you’ll get silence. Not “the data shows injuries are rare.” Not “here’s our comprehensive tracking of adverse events.” Just… nothing. A void where information should be.
This is not an accident. This is by design.
The safety trials for Engerix-B and Recombivax HB—the two hepatitis B vaccines given to American newborns—monitored adverse events for four to five days after injection. That’s it. If your baby developed seizures on day six, or regressed into autism over the following months, or developed autoimmune disease in the following year—none of that would appear in the pre-licensure safety data.
And the post-market surveillance? VAERS is a voluntary reporting system that the CDC itself acknowledges captures only a tiny fraction of adverse events. A Harvard-funded study found it captures perhaps 1% of actual vaccine injuries. Vaccine court has paid out over $5 billion in claims while simultaneously being structured to make filing nearly impossible for average families.
So when Dr. Cody Meissner voted against removing the Hep B birth dose and said he saw “clear evidence of the benefits” but “not the harms,” he was accidentally revealing the entire rotten structure. Of course he doesn’t see the harms. Nobody is systematically looking for them.
The Invisibility of Vaccine Injury
Here’s what most people don’t understand about vaccine injury: it’s nothing like a gunshot wound.
If you shoot someone, the cause is obvious. There’s a bullet, a wound, blood, a clear mechanism of action visible to any observer. Even a medical examiner who’s never seen the victim before can determine cause of death.
Vaccine injury doesn’t work that way. When aluminum nanoparticles from a vaccine cross the blood-brain barrier via macrophages, when they lodge in brain tissue and trigger chronic neuroinflammation, when a child slowly regresses over weeks or months—there’s no bullet. There’s no smoking gun. There’s just a before and an after, and a desperate parent trying to explain to doctors that something changed.
This invisibility is the vaccine program’s greatest protection. Because the injury mechanism is complex and delayed, because it doesn’t leave an obvious wound, because it requires actually looking to find—and because no one in authority is looking—the injuries simply don’t exist in the official record.
I watched my own son Jamie regress after his vaccines. A healthy, developing toddler who lost his words, stopped making eye contact, and retreated into a world we couldn’t reach. My wife and I know what happened. Thousands of other parents know the same thing happened to their children. But because this type of injury doesn’t show up on a simple blood test, because there’s no autopsy finding that says “vaccine-induced encephalopathy,” ACIP members can sit in a room and say with straight faces that they don’t see evidence of harm.
They’re not lying. They literally can’t see it. Because no one is measuring it.
The Chicken Pox Conundrum
Here’s an example that illustrates the insanity of our current approach.
The varicella (chicken pox) vaccine was added to the schedule in 1995. It definitely reduces chicken pox cases. The data is clear on that front. Mission accomplished, right?
But what about the other side of the ledger?
Emerging research suggests that wild chicken pox infection provides some protective effect against brain cancers—particularly glioma, the most common type of primary brain tumor. Multiple studies have found that people who had chicken pox as children have significantly lower rates of brain cancer later in life. The hypothesis is that the immune response to wild varicella provides lasting immunological benefits that extend far beyond preventing itchy spots.
Meanwhile, the vaccine itself has been associated with increased rates of autoimmune conditions. Studies have linked varicella vaccination to higher rates of herpes zoster (shingles) outbreaks in younger age groups, to autoimmune disorders, to various adverse events that weren’t captured in the original short-term safety trials.
So what’s the true risk-benefit of the chicken pox vaccine? Does preventing a week of itchy discomfort in childhood justify potentially increased rates of brain cancer and autoimmune disease later in life?
ACIP can’t answer this question. They literally don’t have the data. They can show you chicken pox cases going down. They cannot show you a comprehensive analysis of long-term neurological and immunological outcomes in vaccinated versus unvaccinated populations, because that study has never been done.
And so they keep recommending the vaccine based on the only data they have—the disease prevention data—while remaining willfully blind to consequences they’ve never bothered to measure.
The ACIP Paradox
Sunday’s vote was historic, but it also revealed the fundamental paradox of vaccine regulation in America.
The committee members who voted to remove the universal Hep B birth dose recommendation did so largely based on comparative evidence from Europe, parental concerns, and the basic logic that vaccinating a 12-hour-old baby for a sexually transmitted disease their mother doesn’t have makes no medical sense. They were right to do so.
But the committee members who voted against the change weren’t wrong either, from their perspective. They looked at the only data they have—disease prevention data—and concluded that removing the recommendation could lead to more hepatitis B cases. And within their limited framework, they’re correct.
The problem is the framework itself.
True risk-benefit analysis requires data on both risks AND benefits. ACIP has comprehensive data on benefits (disease prevention) and virtually no data on risks (vaccine injury). So every decision they make is fundamentally flawed from the start.
When Dr. Joseph Hibbeln complained that “no rational science has been presented” to support changing the recommendations, he was inadvertently indicting the entire system. Of course no comprehensive vaccine injury data was presented—such data doesn’t exist because no one has been willing to collect it.
This is like asking someone to make an informed financial decision while only showing them potential profits and hiding all possible losses. Of course the decision will be skewed. Of course you’ll end up with a bloated portfolio of high-risk investments that look great on paper.
The Real Reform
If RFK Jr. and the new HHS leadership want to actually fix the vaccine program, they need to understand that removing individual vaccines or making them “optional” is just rearranging deck chairs on the Titanic.
The real reform is creating the data infrastructure that should have existed from the beginning.
We need a comprehensive, long-term, vaccinated-versus-unvaccinated health outcomes study. Not a five-day safety trial. A multi-decade tracking of neurological, immunological, and developmental outcomes across populations with varying vaccination status. Florida just eliminated all vaccine mandates—that state alone could provide the data we need within ten years if someone had the courage to actually collect it.
We need a vaccine injury surveillance system that actually captures adverse events. Not a voluntary reporting system that misses 99% of injuries. An active surveillance system with trained clinicians looking for the kinds of delayed, complex injuries that vaccines actually cause.
We need accountability for manufacturers. The 1986 National Childhood Vaccine Injury Act removed all liability from vaccine makers—and predictably, the vaccine schedule exploded afterward while safety research stagnated. Why would any company invest in safety when they can’t be sued for injuries?
Without this data, every ACIP meeting will be the same performance we watched this week: members confidently citing disease prevention data while admitting they can’t see evidence of harm—not because harm doesn’t exist, but because no one is looking for it.
What Comes Next
Sunday’s vote was a crack in the wall. For the first time, an American regulatory body acknowledged that perhaps vaccinating every newborn within hours of birth for a disease primarily transmitted through sex and IV drug use doesn’t make sense when the mother has already tested negative.
But the forces of institutional inertia are already mobilizing. The American Academy of Pediatrics is “disappointed.” The American Medical Association is calling for the CDC to reject the recommendation. The pharmaceutical industry—which collects over $225 million annually from Hep B birth doses alone—will fight to restore the universal recommendation.
They will cite the same data they always cite: disease prevention data. Cases prevented. Infections avoided. Lives saved—theoretically.
They will not cite vaccine injury data, because that data doesn’t exist in any comprehensive form. They will not present long-term health outcomes in vaccinated versus unvaccinated children, because those studies have been actively avoided for decades. They will not acknowledge the thousands of families who have watched their children regress after vaccination, because those injuries aren’t captured in any official database.
And this is why ACIP will always be hamstrung. Until we build the data infrastructure to actually measure vaccine injury—to put real numbers on the other side of the ledger—every vaccine decision will be based on incomplete information. Every “risk-benefit analysis” will be a fraud, because we’re only measuring half the equation.
The hepatitis B birth dose vote was a small victory. But the larger battle—for actual science, for complete data, for true informed consent—that battle is just beginning.
And until we win it, ACIP will continue making decisions in the dark, confidently citing evidence of benefits while remaining deliberately blind to the harms they’ve never bothered to measure.
About the author
 |
J.B. Handley is the proud father of a child with Autism. He spent his career in the private equity industry and received his undergraduate degree with honors from Stanford University. His first book, How to End the Autism Epidemic, was published in September 2018. The book has sold more than 75,000 copies, was an NPD Bookscan and Publisher’s Weekly Bestseller, broke the Top 40 on Amazon, and has more than 1,000 Five-star reviews. Mr. Handley and his nonspeaking son are also the authors of Underestimated: An Autism Miracle and co-produced the film SPELLERS, available now on YouTube.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
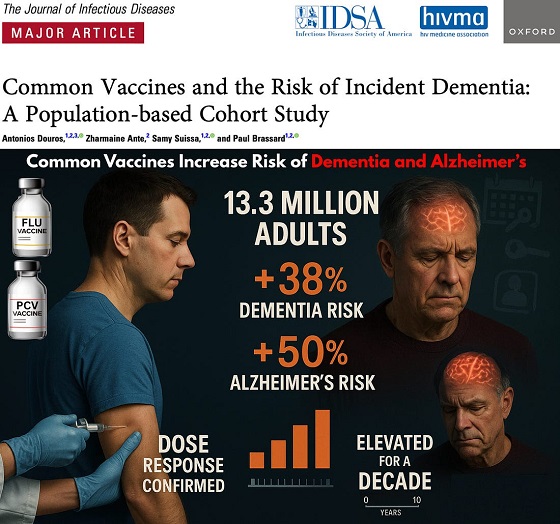

The single largest vaccine–dementia study ever conducted (n=13.3 million) finds risk intensifies with more doses, remains elevated for a full decade, and is strongest after flu and pneumococcal shots.
The single largest and most rigorous study ever conducted on vaccines and dementia — spanning 13.3 million UK adults — has uncovered a deeply troubling pattern: those who received common adult vaccines faced a significantly higher risk of both dementia and Alzheimer’s disease.
The risk intensifies with more doses, remains elevated for a full decade, and is strongest after influenza and pneumococcal vaccination. With each layer of statistical adjustment, the signal doesn’t fade — it becomes sharper, more consistent, and increasingly difficult to explain away.
And critically, these associations persisted even after adjusting for an unusually wide range of potential confounders, including age, sex, socioeconomic status, BMI, smoking, alcohol-related disorders, hypertension, atrial fibrillation, heart failure, coronary artery disease, stroke/TIA, peripheral vascular disease, diabetes, chronic kidney and liver disease, depression, epilepsy, Parkinson’s disease, cancer, traumatic brain injury, hypothyroidism, osteoporosis, and dozens of medications ranging from NSAIDs and opioids to statins, antiplatelets, immunosuppressants, and antidepressants.
Even after controlling for this extensive list, the elevated risks remained strong and remarkably stable.
Vaccinated Adults Had a 38% Higher Risk of Dementia
The primary adjusted model showed that adults receiving common adult vaccines (influenza, pneumococcal, shingles, tetanus, diphtheria, pertussis) had a:
38% increased risk of developing dementia (OR 1.38)
This alone dismantles the narrative of “vaccines protect the brain,” but the deeper findings are far worse.
Alzheimer’s Disease Risk Is Even Higher — 50% Increased Risk
Buried in the supplemental tables is a more shocking result: when the authors restricted analyses to Alzheimer’s disease specifically, the association grew even stronger.
50% increased risk of Alzheimer’s (Adjusted OR 1.50)
This indicates the effect is not random. The association intensifies for the most devastating subtype of dementia.
Clear Dose–Response Pattern: More Vaccines = Higher Risk
 |
The authors ran multiple dose–response models, and every one of them shows the same pattern:
Dementia (all types)
From eTable 2:
- 1 vaccine dose → Adjusted OR 1.26 (26% higher risk)
- 2–3 doses → Adjusted OR 1.32 (32% higher risk)
- 4–7 doses → Adjusted OR 1.42 (42% higher risk)
- 8–12 doses → Adjusted OR 1.50 (50% higher risk)
- ≥13 doses → Adjusted OR 1.55 (55% higher risk)
Alzheimer’s Disease (AD) Shows the Same—and Even Stronger—Trend
From eTable 7:
- 1 dose → Adjusted OR 1.32 (32% higher risk)
- 2–3 doses → Adjusted OR 1.41 (41% higher risk)
- ≥4 doses → Adjusted OR 1.61 (61% higher risk)
This is one of the most powerful and unmistakable signals in epidemiology.
Time–Response Curve: Risk Peaks Soon After Vaccination and Remains Elevated for Years
 |
Another signal strongly inconsistent with mere bias: a time-response relationship.
The highest dementia risk occurs 2–4.9 years after vaccination (Adjusted OR 1.56). The risk then slowly attenuates but never returns to baseline, remaining elevated across all time windows.
After 12.5 years, the risk is still meaningfully elevated (Adjusted OR 1.28) — a persistence incompatible with short-term “detection bias” and suggestive of a long-lasting biological impact.
This pattern is what you expect from a biological trigger with long-latency neuroinflammatory or neurodegenerative consequences.
Even After a 10-Year Lag, the Increased Risk Does Not Disappear
When the authors apply a long 10-year lag — meant to eliminate early detection bias — the elevated risk persists:
- Dementia: OR 1.20
- Alzheimer’s: OR 1.26
If this were simply “people who see doctors more often get diagnosed earlier,” the association should disappear under long lag correction.
Influenza and Pneumococcal Vaccines Drive the Signal
Two vaccines show particularly strong associations:
Influenza vaccine
- Dementia: OR 1.39 → 39% higher risk
- Alzheimer’s: OR 1.49 → 49% higher risk
Pneumococcal vaccine
- Dementia: OR 1.12 → 12% higher risk
- Alzheimer’s: OR 1.15 → 15% higher risk
And again, both exhibit dose–response escalation — the hallmark pattern of a genuine exposure–outcome relationship.
Taken together, the findings across primary, supplemental, dose–response, time–response, stratified, and sensitivity analyses paint the same picture:
• A consistent association between cumulative vaccination and increased dementia risk
• A stronger association for Alzheimer’s than for general dementia
• A dose–response effect — more vaccines, higher risk
• A time–response effect — risk peaks after exposure and persists long-term
• Influenza and pneumococcal vaccines strongly drive the signal
• The association remains after 10-year lag correction and active comparator controls
This is what a robust epidemiologic signal looks like.
In the largest single study ever conducted on vaccines and dementia, common adult vaccinations were associated with a 38% higher risk of dementia and a 50% higher risk of Alzheimer’s disease. The risk increases with more doses, persists for a decade, and is strongest for influenza and pneumococcal vaccines.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


Wayne Gretzky’s Terrible, Awful Week.. And Soccer/ Football.

Western Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns
Common Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s

US podcaster Glenn Beck extends a lifeline to a Saskatchewan woman waiting for MAiD
-
Bruce Dowbiggin1 day ago
Wayne Gretzky’s Terrible, Awful Week.. And Soccer/ Football.
-
espionage22 hours ago
Western Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns
-
Focal Points13 hours ago
Common Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s
-
 Opinion1 day ago
Opinion1 day agoThe day the ‘King of rock ‘n’ roll saved the Arizona memorial
-
 Automotive3 hours ago
Automotive3 hours agoThe $50 Billion Question: EVs Never Delivered What Ottawa Promised
-
 Agriculture1 day ago
Agriculture1 day agoCanada’s air quality among the best in the world
-
 Business20 hours ago
Business20 hours agoCanada invests $34 million in Chinese drones now considered to be ‘high security risks’
-
Health11 hours ago
The Data That Doesn’t Exist