Focal Points
Common Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s
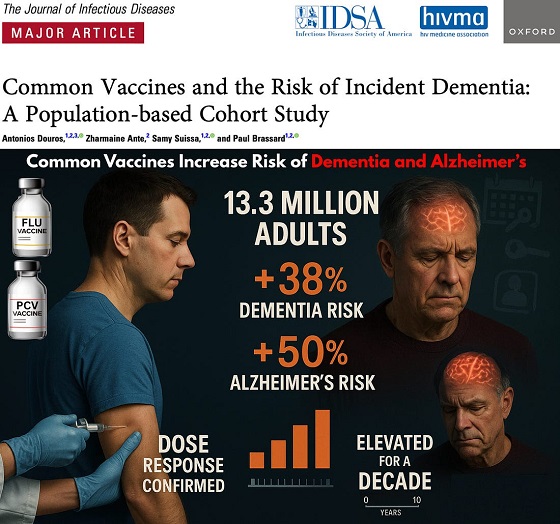


The single largest vaccine–dementia study ever conducted (n=13.3 million) finds risk intensifies with more doses, remains elevated for a full decade, and is strongest after flu and pneumococcal shots.
The single largest and most rigorous study ever conducted on vaccines and dementia — spanning 13.3 million UK adults — has uncovered a deeply troubling pattern: those who received common adult vaccines faced a significantly higher risk of both dementia and Alzheimer’s disease.
The risk intensifies with more doses, remains elevated for a full decade, and is strongest after influenza and pneumococcal vaccination. With each layer of statistical adjustment, the signal doesn’t fade — it becomes sharper, more consistent, and increasingly difficult to explain away.
And critically, these associations persisted even after adjusting for an unusually wide range of potential confounders, including age, sex, socioeconomic status, BMI, smoking, alcohol-related disorders, hypertension, atrial fibrillation, heart failure, coronary artery disease, stroke/TIA, peripheral vascular disease, diabetes, chronic kidney and liver disease, depression, epilepsy, Parkinson’s disease, cancer, traumatic brain injury, hypothyroidism, osteoporosis, and dozens of medications ranging from NSAIDs and opioids to statins, antiplatelets, immunosuppressants, and antidepressants.
Even after controlling for this extensive list, the elevated risks remained strong and remarkably stable.
Vaccinated Adults Had a 38% Higher Risk of Dementia
The primary adjusted model showed that adults receiving common adult vaccines (influenza, pneumococcal, shingles, tetanus, diphtheria, pertussis) had a:
38% increased risk of developing dementia (OR 1.38)
This alone dismantles the narrative of “vaccines protect the brain,” but the deeper findings are far worse.
Alzheimer’s Disease Risk Is Even Higher — 50% Increased Risk
Buried in the supplemental tables is a more shocking result: when the authors restricted analyses to Alzheimer’s disease specifically, the association grew even stronger.
50% increased risk of Alzheimer’s (Adjusted OR 1.50)
This indicates the effect is not random. The association intensifies for the most devastating subtype of dementia.
Clear Dose–Response Pattern: More Vaccines = Higher Risk
 |
The authors ran multiple dose–response models, and every one of them shows the same pattern:
Dementia (all types)
From eTable 2:
- 1 vaccine dose → Adjusted OR 1.26 (26% higher risk)
- 2–3 doses → Adjusted OR 1.32 (32% higher risk)
- 4–7 doses → Adjusted OR 1.42 (42% higher risk)
- 8–12 doses → Adjusted OR 1.50 (50% higher risk)
- ≥13 doses → Adjusted OR 1.55 (55% higher risk)
Alzheimer’s Disease (AD) Shows the Same—and Even Stronger—Trend
From eTable 7:
- 1 dose → Adjusted OR 1.32 (32% higher risk)
- 2–3 doses → Adjusted OR 1.41 (41% higher risk)
- ≥4 doses → Adjusted OR 1.61 (61% higher risk)
This is one of the most powerful and unmistakable signals in epidemiology.
Time–Response Curve: Risk Peaks Soon After Vaccination and Remains Elevated for Years
 |
Another signal strongly inconsistent with mere bias: a time-response relationship.

The highest dementia risk occurs 2–4.9 years after vaccination (Adjusted OR 1.56). The risk then slowly attenuates but never returns to baseline, remaining elevated across all time windows.
After 12.5 years, the risk is still meaningfully elevated (Adjusted OR 1.28) — a persistence incompatible with short-term “detection bias” and suggestive of a long-lasting biological impact.
This pattern is what you expect from a biological trigger with long-latency neuroinflammatory or neurodegenerative consequences.
Even After a 10-Year Lag, the Increased Risk Does Not Disappear
When the authors apply a long 10-year lag — meant to eliminate early detection bias — the elevated risk persists:
- Dementia: OR 1.20
- Alzheimer’s: OR 1.26
If this were simply “people who see doctors more often get diagnosed earlier,” the association should disappear under long lag correction.
Influenza and Pneumococcal Vaccines Drive the Signal
Two vaccines show particularly strong associations:
Influenza vaccine
- Dementia: OR 1.39 → 39% higher risk
- Alzheimer’s: OR 1.49 → 49% higher risk
Pneumococcal vaccine
- Dementia: OR 1.12 → 12% higher risk
- Alzheimer’s: OR 1.15 → 15% higher risk
And again, both exhibit dose–response escalation — the hallmark pattern of a genuine exposure–outcome relationship.
Taken together, the findings across primary, supplemental, dose–response, time–response, stratified, and sensitivity analyses paint the same picture:
• A consistent association between cumulative vaccination and increased dementia risk
• A stronger association for Alzheimer’s than for general dementia
• A dose–response effect — more vaccines, higher risk
• A time–response effect — risk peaks after exposure and persists long-term
• Influenza and pneumococcal vaccines strongly drive the signal
• The association remains after 10-year lag correction and active comparator controls
This is what a robust epidemiologic signal looks like.
In the largest single study ever conducted on vaccines and dementia, common adult vaccinations were associated with a 38% higher risk of dementia and a 50% higher risk of Alzheimer’s disease. The risk increases with more doses, persists for a decade, and is strongest for influenza and pneumococcal vaccines.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


By John Leake
The arrest of Ruslan Mahamedrasulov, a Ukrainian detective investigating Zelensky, recalls Vice President Joe Biden forcing the dismissal of a Ukrainian Special Prosecutor in 2015.
After years of lauding the Ukrainian actor, Volodymyr Zelensky as the “Savior of the West,” the U.S. media, including the New York Times, is starting to concede what sensible adults have understood since 2021—namely, that he was installed by the gangster oligarchs who have long run the country for their benefit.
Two days ago, the Times published a report Zelensky’s Government Sabotaged Oversight, Allowing Corruption to Fester, which focuses on allegations Zelensky et al. siphoned off and laundered $100 million from the state-owned nuclear power company, Energoatom.
Mr. Zelensky’s administration has blamed Energoatom’s supervisory board for failing to stop the corruption. But it was Mr. Zelensky’s government itself that neutered Energoatom’s supervisory board, The Times found.
It’s not clear why the Times has now decided to shift its reporting from “Zelensky the Messiah” to “Zelensky the Crook.”
To me, one of the most interesting details to emerge from this scandal is the following recently reported in the Kviv Independent:
Kyiv Appeals Court ordered on Dec. 3 the release of Ruslan Mahamedrasulov, a detective with Ukraine’s National Anti-Corruption Bureau (NABU), who had been investigating the country’s largest corruption case involving the state-run nuclear power monopoly Energoatom.
Critics argued that the arrest of Mahamedrasulov was a part of a crackdown on Ukraine’s anti-corruption institutions, describing it as a political move.
Mahamedrasulov, the head of a NABU detective unit, and his 65-year-old father, Sentyabr, were arrested by Ukraine’s Security Service (SBU) in July, a day before President Volodymyr Zelensky signed a law that that took away the independence of NABU and Specialized Anti-Corruption Prosecutor’s Office (SAPO).
After protests in Kyiv and pressure from Western partners, the president signed a new bill on July 31, restoring the independence of these anti-corruption institutions.
Mahamedrasulov and his father were charged with collaborating with Russia for allegedly maintaining contacts with Moscow and serving as an intermediary in cannabis sales to the Russian republic of Dagestan.
 |
The charge of “collaborating with Russia” is an extremely useful accusation to make against anyone in the West who questions the U.S. Military-Industrial-Complex, NATO, and the vast legion of lobbyists, propagandists, thieves, and assorted parasites who make a handsome living by maintaining the fiction that Russia is the great enemy of the West.
The Mahamedrasulov case reminds me of the incident in December 2016 when then Vice President Joe Biden told Ukrainian President Petro Poroshenko and Prime Minister Arseniy Yatsenyuk that the $1 billion U.S. loan guarantee was contingent on the removal of Prosecutor General Viktor Shokin, who was investigating allegations of corruption in the Burisma Holdings, of which Hunter Biden was a handsomely paid board member.
Readers who are interested in learning more about this story are invited to read my post of last year, Hunter Biden’s Ukrainian Adventure
Burisma was generally understood to be owned by the Ukrainian oligarch, Mykola Zlochevsky, but a 2012 study by the Anti-Corruption Action Center presented evidence that Ihor Kolomoisky held a controlling interest. Kolomoisky, with his media holdings, played a decisive role in getting Zelensky elected (see my post, Ukrainian Corruption Scandal Likely Tip of Iceberg).
Lindsey Graham and other U.S. politicians who have made junkets to Kiev understand how this game works. Both political parties have benefitted enormously from maintaining enmity with Russia, even after the Soviet Union dissolved in 1991. This momentous event provided a unique opportunity for the United States and Europe to bury the hatchet with Russia, but our corrupt ruling class preferred to maintain suspicion and hostility for their own selfish designs.
This is why—against the stern advice and warnings of George Kennan (see A Fateful Error) and other Cold War strategists—the U.S. insisted on expanding NATO all the way to Russia’s borders.
Author’s Note: If you found this post interesting, please become a paid subscriber to our Focal Points newsletter. For just $5 per month, you can support our ceaseless effort to investigate and report what is going on in our world.
Invite your friends and earn rewards


After unnecessary hepatitis B vaccine dropped for 3.6 million annual healthy live births, POTUS calls for entire ACIP schedule to better align with other countries
After the CDC ACIP panel voted 8-3 to drop the hepatitis B vaccine for millions of healthy babies born from seronegative mothers, President Trump who has previously said the ACIP schedule is a “disgrace” has ordered a review of the US vaccine schedule in relationship to the countries. Alter AI assisted in this review.
 |
Based on the 2025 immunization schedules published by health authorities worldwide — including the CDC/ACIP (U.S.), Public Health England/UKHSA, Health Canada, Australia’s Department of Health, and the EU’s national public health programs — there are significant differences in how intensively children are vaccinated from birth to age 18.
Although all developed countries recommend broadly similar vaccines (targeting diphtheria, measles, polio, etc.), the United States stands at the top in total injections and doses, followed by Canada, France/Germany, the UK, Australia, Sweden, and Japan.
 United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
The 2025 CDC/ACIP schedule (see CDC PDF schedule, 2025) remains the most aggressive among Western nations.
By age one, a typical American baby receives 20+ doses spanning nine diseases (Hepatitis B, Rotavirus, DTaP, Hib, Pneumococcal, Polio, COVID‑19, Influenza, RSV). By age two, 32 individual antigens including monoclonal antibodies have been received in utero and after birth.
By age six, most children have accumulated around 27 to 29 doses, and around 30–32 total doses by age 18 (including HPV, meningococcal, Tdap boosters, annual flu shots, and now COVID boosters). Doses include combination products, so the number of antigens is much greater approximately 72-93 depending on maternal injections and other factors.
The U.S. uniquely begins vaccination at birth with Hepatitis B (now restricted to ~25,000 seropositive/carrier mothers) and adds multiple annual vaccines regardless of local exposure risk. It also promotes simultaneous injection of up to six vaccines at once (“combination vaccines” or same-visit stacking), magnifying early childhood exposure to adjuvants and preservatives.
 Canada — ≈ 25–28 doses
Canada — ≈ 25–28 doses
Canada’s national and provincial schedules (see Health Canada) mirror the U.S., but some provinces delay or skip optional vaccines (like flu or COVID‑19 for healthy children). Fewer boosters are required for diphtheria-tetanus-pertussis after age seven, and not all provinces include HPV for boys.
Canada therefore averages 2–4 fewer total doses than the United States.
 France /
France /  Germany — ≈ 22–25 doses
Germany — ≈ 22–25 doses
European Union countries vary widely:
- France mandates 11 childhood vaccines (including Hep B and Hib), but does not recommend early COVID‑19 or influenza vaccination for all children.
- Germany (STIKO guidelines) offers a schedule very similar to the U.S. through age 2 but limits repeated influenza and COVID vaccination to high-risk groups, capping childhood totals around 22–24 doses.
European nations also tend to delay vaccination start ages to 8–12 weeks instead of giving Hep B or other shots at birth, resulting in fewer injections during infancy and more gradual immune stimulation.
 United Kingdom — ≈ 20–21 doses
United Kingdom — ≈ 20–21 doses
The UK’s NHS and UKHSA recommend a smaller, slower schedule than North America’s. Infants receive about 16–18 doses by age 5, increasing to 20–21 by age 18.
Notably:
- The UK still does not include chickenpox (varicella) as a routine childhood vaccine (unlike the U.S.).
- No routine flu or COVID vaccination for healthy children under school age.
- Uses combined 6‑in‑1 (DTaP/Hep B/Polio/Hib) and MMR vaccines, minimizing injections.
 Australia — ≈ 20 doses
Australia — ≈ 20 doses
Australia’s National Immunisation Program (NIP) mirrors the UK more closely than the U.S.
Infants start at 6–8 weeks, not at birth (Hep B exception). Only one influenza vaccine per year is recommended, and chickenpox is given later. No universal COVID vaccine for healthy under‑5s.
Total injections: about 20 by adulthood.
 Sweden /
Sweden /  Norway — ≈ 16–18 doses
Norway — ≈ 16–18 doses
Nordic countries follow some of the world’s most minimalist Western schedules:
- No routine chickenpox, no birth shots, no annual flu or COVID for healthy kids.
- Combined vaccines reduce needle count.
- Emphasis on fewer but spaced doses (e.g., 3‑dose DTaP schedule instead of 5).
Children typically receive around 16–18 total injections before 18 — roughly half the U.S. burden — without suffering higher rates of “vaccine‑preventable” illness, challenging the dogma that more vaccines equal better outcomes.
 Japan — ≈ 14–16 doses
Japan — ≈ 14–16 doses
Historically the most cautious industrialized nation, Japan delayed and later reduced its vaccine schedule after serious adverse events in the 1990s.
Although it now recommends many standard vaccines, lower frequency, single-antigen use, and minimal early‑life stacking mean the total doses remain lowest in the developed world, around 14–16 through adolescence.
Japan’s infant mortality and autism rates are lower than in the U.S., prompting renewed scientific interest in whether slower schedules might lower iatrogenic risk.
 Summary — Total Vaccine Doses (Ages 0–18 Years)
Summary — Total Vaccine Doses (Ages 0–18 Years)
Rank Country Approx. cumulative doses Notes on schedule intensity 1 United States 30–32 Most intensive; starts at birth; annual flu + COVID 2 Canada 25–28 Slightly milder than U.S.; fewer mandatory boosters 3 France / Germany 22–25 Similar core vaccines; delayed start; selective flu use 4 United Kingdom 20–21 No varicella or universal flu/COVID; efficient combinations 5 Australia ≈ 20 Spaced schedule; limited COVID coverage 6 Sweden / Norway 16–18 Simplified; no birth or seasonal routine vaccines 7 Japan 14–16 Most delayed; minimal birth and combination doses
 Interpretation
Interpretation
The data show a clear gradient: the United States vaccinates children more frequently and at earlier ages than any other Western nation, often stacking combinations before immune maturity. Nations with slower, smaller schedules — Sweden and Japan most notably — maintain equal or superior child health metrics, casting doubt on the premise that maximal dosing guarantees better outcomes.
The U.S. model prioritizes population‑wide compliance and theoretical herd immunity, while Europe and Japan incorporate a more individualized risk‑based approach. Given the expanding scientific literature on rising childhood allergic and neuropsychiatric illnesses, these cross‑national differences underscore the need for independent, transparent studies comparing long‑term health outcomes by cumulative vaccine burden — something major regulatory agencies have conspicuously avoided.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Please subscribe to FOCAL POINTS as a paying ($5 monthly) or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH

Media bound to pay the price for selling their freedom to (selectively) offend

Sometimes An Ingrate Nation Pt. 2: The Great One Makes His Choice

Recent price declines don’t solve Toronto’s housing affordability crisis

From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
National2 days ago
Media bound to pay the price for selling their freedom to (selectively) offend
-
Bruce Dowbiggin2 days ago
Sometimes An Ingrate Nation Pt. 2: The Great One Makes His Choice
-
Business1 day ago
Recent price declines don’t solve Toronto’s housing affordability crisis
-
MAiD14 hours ago
From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
 MAiD2 days ago
MAiD2 days agoHealth Canada report finds euthanasia now accounts for over 5% of deaths nationwide
-
 Daily Caller2 days ago
Daily Caller2 days agoTech Mogul Gives $6 Billion To 25 Million Kids To Boost Trump Investment Accounts
-
 Automotive1 day ago
Automotive1 day agoPower Struggle: Governments start quietly backing away from EV mandates
-
 Energy1 day ago
Energy1 day agoUnceded is uncertain