Health
CDC Vaccine Panel Votes to End Universal Hep B Vaccine for Newborns



“While I question whether any baby should receive a vaccine against a rare disease in infancy, I am pleased that this is now a matter for parents and their healthcare practitioner to decide — not a state mandate based on a federal pharma-backed recommendation.”
Advisers to the Centers for Disease Control and Prevention (CDC) have voted to end a decades-long recommendation that all infants born in the U.S. receive the hepatitis B vaccine (Hep B) within 12-24 hours of birth.
Instead, for babies born to mothers who test negative for hepatitis B, the committee recommends that families determine whether to give their child the Hep B shot at birth through individual decision-making with their physician.
For infants who don’t get the birth dose, the committee recommends the initial dose of the vaccine not be administered until infants are at least 2 months old.
Three of the 11 committee members — Dr. Raymond Pollack, Dr. Cody Meissner and Dr. Joseph R. Hibbeln — opposed the recommendation. The remaining eight members supported it.
Andrew Johnson from the Centers for Medicare & Medicaid Services assured the committee that the language change will not affect Medicaid or insurance coverage of the vaccine.
For mothers whose hepatitis B status is unknown or who test positive, the birth dose recommendation remains in place.
Children’s Health Defense CEO Mary Holland, a long-time critic of the universal birth dose policy, welcomed the committee’s vote to “end the ill-considered universal recommendation for the Hep B birth vaccine dose.”
Holland added:
“The science behind that universal recommendation was a sham, based on thoroughly inadequate clinical trials. Hundreds of babies unquestionably died because of it. While I question whether any baby should receive a vaccine against a rare disease in infancy, I am pleased that this is now a matter for parents and their healthcare practitioner to decide — not a state mandate based on a federal pharma-backed recommendation.
“And while the ACIP [Advisory Committee on Immunization Practices] debate on this issue was tedious and rancorous at times, it is an extremely positive change that actual debate about childhood vaccines is occurring in government venues with impact. This is the transparency that Secretary Kennedy promised.”
Dr. Monique Yohanan, senior fellow for health policy at Independent Women, told The Defender there was never “a good science-based reason to have a universal vaccination that 99% of babies born in the United States are not at any risk,” and that the vote was “good news for babies.”
She added that she hoped it would “provide an opportunity to actually have outreach to the moms who are positive for hepatitis B, women who are immigrants, women who are IV drug users.” She said the previous policy was “performative compassion. And these are really underserved women who we ignored the outreach that they needed.”
The committee also voted 6-4 with one abstention that after the initial Hep B shot, parents should consult with healthcare providers to consider whether their child should have a serology test, which would show whether they had antibodies considered sufficient to protect them against the disease.
The committee voted to update the CDC Vaccines for Children (VFC) Program funding to match ACIP’s recommendations. Several committee members, including Meissner and Hibbeln, abstained from voting on the VFC resolution, protesting that they didn’t understand the implications of the vote — reflecting some of the disagreement that pervaded the two-day meeting.
The votes on the Hep B vaccine were originally scheduled for the September meeting, but were deferred to allow the CDC work group to put together more data to inform the committee’s decision.
Sunday’s vote was postponed from Saturday so members could have more time to review the language of the proposal.
Like flying in a plane that wasn’t safety tested?
The decision to postpone followed a contentious day-long meeting on Thursday, during which some members of the committee and liaisons from professional associations argued there was no need to change the recommendation, because there was no “evidence of harm” from the vaccine.
Advocates for changing the recommendation pointed to a near-complete lack of safety data — small clinical trials for the vaccines tracked infants for a week or less after the shot and little follow-up research on autoimmune and neurological disorders.
Big differences of opinion persisted at Sunday’s meeting.
ACIP member Retsef Levi, Ph.D., said that for parents whose children were at extremely low risk, the decision to give them the vaccine was analogous to flying in a plane — they wouldn’t get in a plane that hadn’t been safety tested, why should they give their child a vaccine that hadn’t been safety tested.
Meissner disagreed, saying, “We know vaccines are safe. There is no question that the COVID vaccine recommendations were dishonest, disingenuous, but the hepatitis B vaccine is very well established.”
In opening remarks, Dr. Robert Malone — who chaired the meeting because the newly named committee chairperson, Dr. Kirk Milhoun, is traveling — said “the credibility of the ACIP rests not on speed, but on rigor.”
Commenting on the heated discussions during Thursday’s meeting, Milhoun said that scientific debates are necessarily contentious.

“If they are not contentious, if they are not approached with rigor, then we end up with bad decisions. We end up with bad science. We must actively engage in responsible debate concerning contentious issues. We must boldly address change, risk new ideas, and conflicting hypotheses, which is the proper nature of evidence-based science.”
Dr. Jason Goldman, a liaison to the ACIP for the American College of Physicians, attacked opposing viewpoints as unscientific. Goldman said the Hep B vaccine discussion was “an unnecessary solution looking for a problem.”
‘If adults won’t go for the shots, then give them to babies’
The Hep B vaccine has been universally recommended for infants since 1991. The first shot is currently given within 24 hours after birth to prevent infection with hepatitis B from mothers who carry the disease — less than 0.5% of mothers.
Mothers can be tested in the hospital to determine whether they have the disease, and current tests have a 100% accuracy rate, according to FDA ex officio ACIP participant Tracy Beth Høeg, M.D., Ph.D.
However, a 1991 New York Times article posted on Substack yesterday by Dr. Meryl Nass showed that when the universal shot was rolled out, the goal was not to prevent maternal transmission — the goal was to prevent adult cases, at a time when adult cases were deemed a national crisis. However, adults commonly didn’t get the shot.
“If adults won’t go for the shots, then give them to babies,” the article said.
Following Thursday’s meeting, legacy media attacked the committee and the CDC’s presenters and highlighted charges of misinformation by liaison members. Liaisons are nonvoting members from professional medical organizations who can offer their opinions and advice to the committee.
Representatives from some of those groups, including the American Academy of Pediatrics (AAP) and the American Medical Association, were disinvited in August from participation in the workgroups due to conflicts of interest.
Since then, the AAP has boycotted the ACIP meetings
At the start of today’s meeting, Meissner castigated AAP for this move. He said he was concerned that by not participating, they would be seen as being more focused on making a political statement than attending to the health of children.
He said that pediatricians should be part of the discussions. “Refusal to participate in the ACIP meetings does not appear to be in the best interest of children.”
Immediately following today’s vote, the Times quoted “experts” from some of the staunchest advocates for all vaccines on the childhood schedule, such as the director of the Center for Infectious Disease Research & Policy, Michael Osterholm, Ph.D., saying that the vote shows federal health authorities can no longer be trusted.
Osterholm, a member of the COVID-19 Advisory Board under the Biden administration, is one of the key players in the “Vaccine Integrity Project,” funded by iAlumbra, a nonprofit founded by Walmart heiress and philanthropist Christy Walton. The project plans to make its own vaccine recommendations.
This Substack is reader-supported.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Vaccine recommendations ‘should not be treated as mandates’
During the day-and-a-half-long discussion about the Hep B vaccine, several committee members, including Dr. Evelyn Griffin, raised concerns that the birth recommendation posed challenges for informed consent, because mothers who had just delivered babies were not in a position to calmly evaluate risks and benefits.
Others, including Levi, argued that the vaccine requirements for children to attend school effectively functioned as mandates.
Liaison members universally disagreed that the recommendations were mandates and argued that ACIP recommendations were really only recommendations, and parents could do what they wanted.
CDC ex officio member, Dr. Adam Langer, who was opposed to changing the recommendation, said that the recommendations had come to function as mandates, but that was not the intention. He proposed the committee make a formal statement that “all vaccine recommendations are recommendations. They should not be treated as mandates.”
He added that mandates put in place by state and local jurisdictions were “problematic.”
“We have a lot of challenges with our culture and our traditions in this country, with telling people what they must and must not do. But that’s not what we’re saying here. We’re saying that at the population level, in the majority of cases, this is what the sign shows is the best practice.”
He said providers should always make the best decision for the individual patient they are working with. “That’s the reason why you’ve been entrusted with a license to practice medicine.”
Watch the ACIP meeting here:
 |
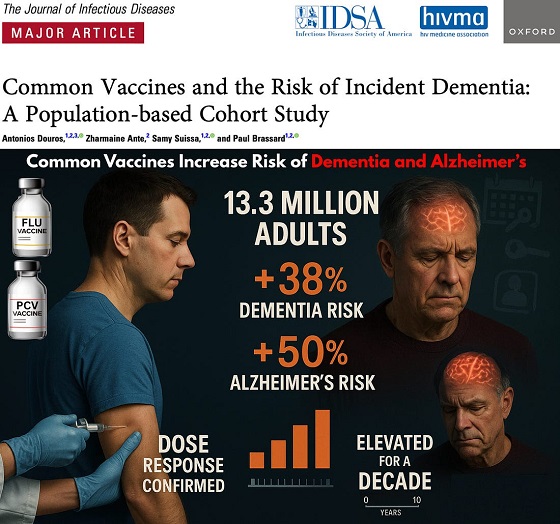

The single largest vaccine–dementia study ever conducted (n=13.3 million) finds risk intensifies with more doses, remains elevated for a full decade, and is strongest after flu and pneumococcal shots.
The single largest and most rigorous study ever conducted on vaccines and dementia — spanning 13.3 million UK adults — has uncovered a deeply troubling pattern: those who received common adult vaccines faced a significantly higher risk of both dementia and Alzheimer’s disease.
The risk intensifies with more doses, remains elevated for a full decade, and is strongest after influenza and pneumococcal vaccination. With each layer of statistical adjustment, the signal doesn’t fade — it becomes sharper, more consistent, and increasingly difficult to explain away.
And critically, these associations persisted even after adjusting for an unusually wide range of potential confounders, including age, sex, socioeconomic status, BMI, smoking, alcohol-related disorders, hypertension, atrial fibrillation, heart failure, coronary artery disease, stroke/TIA, peripheral vascular disease, diabetes, chronic kidney and liver disease, depression, epilepsy, Parkinson’s disease, cancer, traumatic brain injury, hypothyroidism, osteoporosis, and dozens of medications ranging from NSAIDs and opioids to statins, antiplatelets, immunosuppressants, and antidepressants.
Even after controlling for this extensive list, the elevated risks remained strong and remarkably stable.
Vaccinated Adults Had a 38% Higher Risk of Dementia
The primary adjusted model showed that adults receiving common adult vaccines (influenza, pneumococcal, shingles, tetanus, diphtheria, pertussis) had a:
38% increased risk of developing dementia (OR 1.38)
This alone dismantles the narrative of “vaccines protect the brain,” but the deeper findings are far worse.
Alzheimer’s Disease Risk Is Even Higher — 50% Increased Risk
Buried in the supplemental tables is a more shocking result: when the authors restricted analyses to Alzheimer’s disease specifically, the association grew even stronger.
50% increased risk of Alzheimer’s (Adjusted OR 1.50)
This indicates the effect is not random. The association intensifies for the most devastating subtype of dementia.
Clear Dose–Response Pattern: More Vaccines = Higher Risk
 |
The authors ran multiple dose–response models, and every one of them shows the same pattern:
Dementia (all types)
From eTable 2:
- 1 vaccine dose → Adjusted OR 1.26 (26% higher risk)
- 2–3 doses → Adjusted OR 1.32 (32% higher risk)
- 4–7 doses → Adjusted OR 1.42 (42% higher risk)
- 8–12 doses → Adjusted OR 1.50 (50% higher risk)
- ≥13 doses → Adjusted OR 1.55 (55% higher risk)
Alzheimer’s Disease (AD) Shows the Same—and Even Stronger—Trend
From eTable 7:
- 1 dose → Adjusted OR 1.32 (32% higher risk)
- 2–3 doses → Adjusted OR 1.41 (41% higher risk)
- ≥4 doses → Adjusted OR 1.61 (61% higher risk)
This is one of the most powerful and unmistakable signals in epidemiology.
Time–Response Curve: Risk Peaks Soon After Vaccination and Remains Elevated for Years
 |
Another signal strongly inconsistent with mere bias: a time-response relationship.
The highest dementia risk occurs 2–4.9 years after vaccination (Adjusted OR 1.56). The risk then slowly attenuates but never returns to baseline, remaining elevated across all time windows.
After 12.5 years, the risk is still meaningfully elevated (Adjusted OR 1.28) — a persistence incompatible with short-term “detection bias” and suggestive of a long-lasting biological impact.
This pattern is what you expect from a biological trigger with long-latency neuroinflammatory or neurodegenerative consequences.
Even After a 10-Year Lag, the Increased Risk Does Not Disappear
When the authors apply a long 10-year lag — meant to eliminate early detection bias — the elevated risk persists:
- Dementia: OR 1.20
- Alzheimer’s: OR 1.26
If this were simply “people who see doctors more often get diagnosed earlier,” the association should disappear under long lag correction.
Influenza and Pneumococcal Vaccines Drive the Signal
Two vaccines show particularly strong associations:
Influenza vaccine
- Dementia: OR 1.39 → 39% higher risk
- Alzheimer’s: OR 1.49 → 49% higher risk
Pneumococcal vaccine
- Dementia: OR 1.12 → 12% higher risk
- Alzheimer’s: OR 1.15 → 15% higher risk
And again, both exhibit dose–response escalation — the hallmark pattern of a genuine exposure–outcome relationship.
Taken together, the findings across primary, supplemental, dose–response, time–response, stratified, and sensitivity analyses paint the same picture:
• A consistent association between cumulative vaccination and increased dementia risk
• A stronger association for Alzheimer’s than for general dementia
• A dose–response effect — more vaccines, higher risk
• A time–response effect — risk peaks after exposure and persists long-term
• Influenza and pneumococcal vaccines strongly drive the signal
• The association remains after 10-year lag correction and active comparator controls
This is what a robust epidemiologic signal looks like.
In the largest single study ever conducted on vaccines and dementia, common adult vaccinations were associated with a 38% higher risk of dementia and a 50% higher risk of Alzheimer’s disease. The risk increases with more doses, persists for a decade, and is strongest for influenza and pneumococcal vaccines.
Epidemiologist and Foundation Administrator, McCullough Foundation
Support our mission: mcculloughfnd.org
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


After unnecessary hepatitis B vaccine dropped for 3.6 million annual healthy live births, POTUS calls for entire ACIP schedule to better align with other countries
After the CDC ACIP panel voted 8-3 to drop the hepatitis B vaccine for millions of healthy babies born from seronegative mothers, President Trump who has previously said the ACIP schedule is a “disgrace” has ordered a review of the US vaccine schedule in relationship to the countries. Alter AI assisted in this review.
 |
Based on the 2025 immunization schedules published by health authorities worldwide — including the CDC/ACIP (U.S.), Public Health England/UKHSA, Health Canada, Australia’s Department of Health, and the EU’s national public health programs — there are significant differences in how intensively children are vaccinated from birth to age 18.
Although all developed countries recommend broadly similar vaccines (targeting diphtheria, measles, polio, etc.), the United States stands at the top in total injections and doses, followed by Canada, France/Germany, the UK, Australia, Sweden, and Japan.
 United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
United States — Approx. 30–32 vaccine doses (counts combination products as single dose) before age 18
The 2025 CDC/ACIP schedule (see CDC PDF schedule, 2025) remains the most aggressive among Western nations.
By age one, a typical American baby receives 20+ doses spanning nine diseases (Hepatitis B, Rotavirus, DTaP, Hib, Pneumococcal, Polio, COVID‑19, Influenza, RSV). By age two, 32 individual antigens including monoclonal antibodies have been received in utero and after birth.
By age six, most children have accumulated around 27 to 29 doses, and around 30–32 total doses by age 18 (including HPV, meningococcal, Tdap boosters, annual flu shots, and now COVID boosters). Doses include combination products, so the number of antigens is much greater approximately 72-93 depending on maternal injections and other factors.
The U.S. uniquely begins vaccination at birth with Hepatitis B (now restricted to ~25,000 seropositive/carrier mothers) and adds multiple annual vaccines regardless of local exposure risk. It also promotes simultaneous injection of up to six vaccines at once (“combination vaccines” or same-visit stacking), magnifying early childhood exposure to adjuvants and preservatives.
 Canada — ≈ 25–28 doses
Canada — ≈ 25–28 doses
Canada’s national and provincial schedules (see Health Canada) mirror the U.S., but some provinces delay or skip optional vaccines (like flu or COVID‑19 for healthy children). Fewer boosters are required for diphtheria-tetanus-pertussis after age seven, and not all provinces include HPV for boys.
Canada therefore averages 2–4 fewer total doses than the United States.
 France /
France /  Germany — ≈ 22–25 doses
Germany — ≈ 22–25 doses
European Union countries vary widely:
- France mandates 11 childhood vaccines (including Hep B and Hib), but does not recommend early COVID‑19 or influenza vaccination for all children.
- Germany (STIKO guidelines) offers a schedule very similar to the U.S. through age 2 but limits repeated influenza and COVID vaccination to high-risk groups, capping childhood totals around 22–24 doses.
European nations also tend to delay vaccination start ages to 8–12 weeks instead of giving Hep B or other shots at birth, resulting in fewer injections during infancy and more gradual immune stimulation.
 United Kingdom — ≈ 20–21 doses
United Kingdom — ≈ 20–21 doses
The UK’s NHS and UKHSA recommend a smaller, slower schedule than North America’s. Infants receive about 16–18 doses by age 5, increasing to 20–21 by age 18.
Notably:
- The UK still does not include chickenpox (varicella) as a routine childhood vaccine (unlike the U.S.).
- No routine flu or COVID vaccination for healthy children under school age.
- Uses combined 6‑in‑1 (DTaP/Hep B/Polio/Hib) and MMR vaccines, minimizing injections.
 Australia — ≈ 20 doses
Australia — ≈ 20 doses
Australia’s National Immunisation Program (NIP) mirrors the UK more closely than the U.S.
Infants start at 6–8 weeks, not at birth (Hep B exception). Only one influenza vaccine per year is recommended, and chickenpox is given later. No universal COVID vaccine for healthy under‑5s.
Total injections: about 20 by adulthood.
 Sweden /
Sweden /  Norway — ≈ 16–18 doses
Norway — ≈ 16–18 doses
Nordic countries follow some of the world’s most minimalist Western schedules:
- No routine chickenpox, no birth shots, no annual flu or COVID for healthy kids.
- Combined vaccines reduce needle count.
- Emphasis on fewer but spaced doses (e.g., 3‑dose DTaP schedule instead of 5).
Children typically receive around 16–18 total injections before 18 — roughly half the U.S. burden — without suffering higher rates of “vaccine‑preventable” illness, challenging the dogma that more vaccines equal better outcomes.
 Japan — ≈ 14–16 doses
Japan — ≈ 14–16 doses
Historically the most cautious industrialized nation, Japan delayed and later reduced its vaccine schedule after serious adverse events in the 1990s.
Although it now recommends many standard vaccines, lower frequency, single-antigen use, and minimal early‑life stacking mean the total doses remain lowest in the developed world, around 14–16 through adolescence.
Japan’s infant mortality and autism rates are lower than in the U.S., prompting renewed scientific interest in whether slower schedules might lower iatrogenic risk.
 Summary — Total Vaccine Doses (Ages 0–18 Years)
Summary — Total Vaccine Doses (Ages 0–18 Years)
Rank Country Approx. cumulative doses Notes on schedule intensity 1 United States 30–32 Most intensive; starts at birth; annual flu + COVID 2 Canada 25–28 Slightly milder than U.S.; fewer mandatory boosters 3 France / Germany 22–25 Similar core vaccines; delayed start; selective flu use 4 United Kingdom 20–21 No varicella or universal flu/COVID; efficient combinations 5 Australia ≈ 20 Spaced schedule; limited COVID coverage 6 Sweden / Norway 16–18 Simplified; no birth or seasonal routine vaccines 7 Japan 14–16 Most delayed; minimal birth and combination doses
 Interpretation
Interpretation
The data show a clear gradient: the United States vaccinates children more frequently and at earlier ages than any other Western nation, often stacking combinations before immune maturity. Nations with slower, smaller schedules — Sweden and Japan most notably — maintain equal or superior child health metrics, casting doubt on the premise that maximal dosing guarantees better outcomes.
The U.S. model prioritizes population‑wide compliance and theoretical herd immunity, while Europe and Japan incorporate a more individualized risk‑based approach. Given the expanding scientific literature on rising childhood allergic and neuropsychiatric illnesses, these cross‑national differences underscore the need for independent, transparent studies comparing long‑term health outcomes by cumulative vaccine burden — something major regulatory agencies have conspicuously avoided.
FOCAL POINTS (Courageous Discourse) is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Please subscribe to FOCAL POINTS as a paying ($5 monthly) or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH

Media bound to pay the price for selling their freedom to (selectively) offend

Sometimes An Ingrate Nation Pt. 2: The Great One Makes His Choice

Recent price declines don’t solve Toronto’s housing affordability crisis

From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
MAiD1 day ago
From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
 Automotive2 days ago
Automotive2 days agoPower Struggle: Governments start quietly backing away from EV mandates
-
 Business1 day ago
Business1 day agoCarney government should privatize airports—then open airline industry to competition
-
 Business2 days ago
Business2 days agoNew Chevy ad celebrates marriage, raising children
-
 Business1 day ago
Business1 day agoWhat’s Going On With Global Affairs Canada and Their $392 Million Spending Trip to Brazil?
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoA Democracy That Can’t Take A Joke Won’t Tolerate Dissent
-
 Energy1 day ago
Energy1 day agoCanada following Europe’s stumble by ignoring energy reality
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoFrances Widdowson’s Arrest Should Alarm Every Canadian