Dr. Robert Malone
WHO and G20 Exaggerate the Risk and Economic Impact of Outbreaks

From Malone News
Poor quality modeling is being used by WHO and a G20 panel to project our risk of infectious disease pandemics and the financial requirements to address them.
Previously considered a once in a century event, major pandemics are now predicted to occur every 20 to 40 years.
Global authorities view this as an existential threat, and have called for a coordinated international response led by the World Health Organization or the WHO…but not everyone agrees with this perspective.
Researchers from the University of Leeds, including policy experts, Professor Garrett Brown and Dr David Bell, are challenging the assumptions behind these dire warnings. They question whether the massive resources being allocated to pandemic preparedness are truly supported by the evidence.
One of their critiques centers on a chart frequently cited by the WHO, which appears to show a dramatic increase in the outbreaks over the past two decades. Brown and Bell say the chart omits crucial historical context and misrepresents today’s health threats.
Long-standing diseases like yellow fever, influenza, cholera, and the plague have been steadily brought under control, and outbreaks of diseases like monkey pox or natural coronaviruses have likely remained consistent over time, but what has changed, they say, is our improved diagnostic technology enabling us to distinguish diseases more readily than ever before.
Essentially, as surveillance increases, so does the likelihood of finding diseases that may have existed but previously went unnoticed.
In reality, mortality from infectious diseases has been declining for decades, thanks to advances in hygiene, nutrition, medical treatments and reduced poverty, even with COVID 2020, to 2021, mortality remained below 2010 levels.
The WHO has identified nine priority diseases for research and development, yet five of these diseases have never caused more than 1000 recorded deaths in history, aside from COVID 19, whose origins remain a topic of debate, the rest of the diseases are largely confined to specific regions, primarily in parts of Africa.
On the list the WHO also includes a hypothetical outbreak that they call disease X – it’s a placeholder for an unknown outbreak that could emerge in the future.
And while it’s intended to promote vigilance, its severity is entirely speculative and can encourage modelers to use catastrophic scenarios to estimate future risk, causing governments to make fear-based policy decisions based on little evidence.
Brown and Bell are concerned that so much focus on speculative pandemic preparedness is diverting critical resources away from urgent health issues such as tuberculosis and malaria.
Tuberculosis alone kills 1.3 million people annually, while malaria accounts for over 600,000 deaths, mostly among children.
Although testing and treatment for these diseases is relatively inexpensive, their funding could be at risk as more resources are directed towards hypothetical future threats in 2022 a high level, independent panel was convened by the G20 to review our risk of pandemics and the financial requirements to address it.
But again, the two main pieces of evidence the panel relied on to draw its conclusions grossly exaggerated the actual risk of a pandemic.
The first report provided by the G20 panel analysed the major outbreaks of the past two decades, and it was poorly referenced, excluding Covid-19 and the 2009 swine flu, which caused fewer deaths than seasonal flu, the total number of deaths from these events over the last 20 years was under 26,000 a relatively insignificant figure in the context of global disease burdens.
The second report was from Metabiota, a former private. US based corporation, the two graphs provided appear to show an exponential increase in recorded outbreaks. Yet the researchers point out that this trend aligns with the development of modern diagnostic technologies, which naturally increase the detection of previously unnoticed diseases, indeed, the absence of recorded disease outbreaks in the 60s coincides with a lack of technology and communication systems needed to document them.
Metabiota report also included data from an article published in the British Medical Journal in 2023 it shows the rise in mortality outbreaks over the last decade is almost entirely due to Ebola outbreaks – and when these Ebola deaths are excluded from Metabiota data – the mortality trend over the last two decades shows a clear decline – a finding that contradicts the narrative of increasing pandemic risk, the financial demands of the pandemic agenda are another concern.
The G20 panel relied on a report released by the World Bank and the WHO in 2022, which sought $31.1 billion in funding, and an additional World Bank report, using poorly supportive data, sought another 10 to 11 billion annually.
On top this report referenced a 2020 study by Maryanne, which also claimed to show an increase in the frequency of disease outbreaks, but closer inspection reveals the opposite, a sharp decline in disease outbreaks between 2010 and 2020 – and like the Metabiota report – this World Bank report overlooks the fact that the development of new diagnostic tests could account for any observed increase In disease outbreaks since 1960.
Finally, the WHO report exaggerates the economic impact of outbreaks by including extraordinary costs of actions, such as stimulus packages, while downplaying the costs of endemic diseases used for comparison.
This creates a false impression that these relatively low fatality outbreaks were costlier than other diseases, and that such costs could be fully avoided while preparing for pandemics is undoubtedly important.
Brown and Bell argue that the narrative of escalating pandemic threats is misleading. They suggest that the risk from naturally occurring disease outbreaks may actually be decreasing with the rise in detected outbreaks, primarily a result of better diagnostic tools.
Researchers warn that essential global priorities such as cancer, tuberculosis, malaria and nutrition support could be neglected. For example, funding for nutrition development dropped 10% in 2020 and has yet to return to pre pandemic levels.
If resources continue to be diverted towards speculative future scenarios, proven efforts to combat the world’s deadliest diseases may be overshadowed and ultimately cause more harm than good.


“We’re Going Bold to Tackle Autism”
Speaking from the Roosevelt Room today, President Donald J. Trump and U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy, Jr. announced bold new actions to confront the nation’s autism spectrum disorder (ASD) epidemic, which has surged nearly 400% since 2000 and now affects 1 in 31 American children.
“For too long, families have been left without answers or options as autism rates have soared,” Secretary Kennedy said. “Today, we are taking bold action—opening the door to the first FDA-recognized treatment pathway, informing doctors and families about potential risks, and investing in groundbreaking research. We will follow the science, restore trust, and deliver hope to millions of American families.”
First, the U.S. Food and Drug Administration (FDA) will act on a potential treatment for speech-related deficits associated with ASD. The FDA today is publishing a Federal Register notice outlining a label update for leucovorin for cerebral folate deficiency, which has been associated with autism. This action establishes the first FDA-recognized therapeutic for children with cerebral folate deficiency and autistic symptoms.
The change will authorize treatment for children with ASD, with continued use if children show language, social, or adaptive gains. Following the label update for ASD, state Medicaid programs will be able to cover leucovorin for the indication of ASD, in partnership with the Centers for Medicare & Medicaid Services (CMS). Finally, the National Institutes of Health (NIH) will launch confirmatory trials and new research into the impact of leucovorin including safety studies.
While promising, it is important to note that leucovorin is not a cure for ASD and may only lead to improvements in speech-related deficits for a subset of children with ASD. Furthermore, this treatment must be administered under close medical supervision and in conjunction with other non-pharmacological approaches for children with ASD (e.g., behavioral therapy).
“As a physician, I have seen how devastating autism spectrum disorder can be for children and their families,” CMS Administrator Dr. Mehmet Oz said. “Today’s actions represent an unprecedented, comprehensive approach to deepen our understanding of the causes of autism, share what we know and don’t know based on current research, and ensure that every child has a better chance to thrive. By providing access to a drug to treat symptoms associated with autism, we are providing hope to families and providers who have until today had very limited options.”
Second, HHS will act on acetaminophen. Today, the FDA will issue a physician notice and begin the process to initiate a safety label change for acetaminophen (Tylenol and similar products). HHS will launch a nationwide public service campaign to inform families and protect public health.
The FDA is responding to prior clinical and laboratory studies that suggest a potential association between acetaminophen use during pregnancy and adverse neurodevelopmental outcomes. FDA also recognizes that there are contrary studies showing no association and that there can be risks for untreated fever in pregnancy, both for the mother and fetus.
Given the conflicting literature and lack of clear causal evidence, HHS wants to encourage clinicians to exercise their best judgment in use of acetaminophen for fevers and pain in pregnancy by prescribing the lowest effective dose for the shortest duration when treatment is required. Furthermore, FDA recognizes that acetaminophen is often the only tool for fevers and pain in pregnancy, as other alternatives (e.g., NSAIDs) have well documented adverse effects. FDA is partnering with manufacturers to update labeling and drive new research to safeguard mothers, children, and families.
“A growing body of evidence suggests that some children suffering from autism are folate deficient within the brain—a problem that can be treated with leucovorin,” FDA Commissioner Dr. Marty Makary said. “Given the extent of the current autism epidemic, physicians should immediately have this treatment option available for candidate children. We are also sharing new information about the potential risks of acetaminophen so patients can make a more informed decision with their health care provider.”
Third, NIH today is announcing the recipients of the Autism Data Science Initiative (ADSI), funding 13 projects totaling more than $50 million to transform autism research. ADSI integrates large-scale biological, clinical, and behavioral data with an exposomics approach that examines environmental, nutritional, medical, and social factors alongside genetics.
Projects employ advanced methods such as machine learning and organoid models, address both children and adults across the lifespan, and establish replication hubs to ensure rigor. Each project includes community engagement to align research with the needs of autistic individuals, families, and clinicians.
“Millions of American families who care for autistic kids need scientists to apply gold standard science, expertise, and open minds to figure out how to help these kids,” NIH Director Dr. Jay Bhattacharya said. “With the Autism Data Science Initiative, NIH is harnessing cutting-edge science to uncover the root causes of autism. We are building knowledge that can improve lives and restore hope for families.”
Malone News is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.

 Robert W Malone MD, MS
Robert W Malone MD, MS
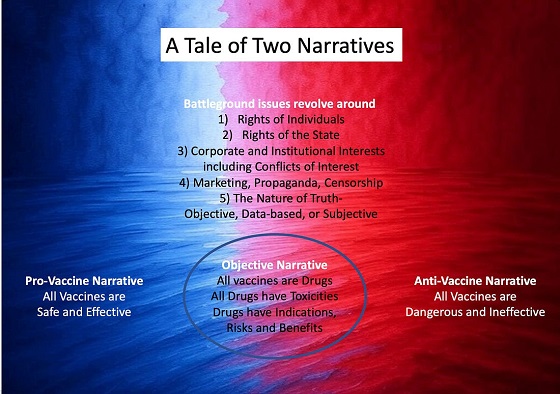
A Tale of Two Narratives
The recent West Texas outbreak of Measles has become politicized and now provides a case study of how the polarization and weaponization of politics and public health in the United States results in dysfunctional public policy. Currently, there are two major competing narratives concerning US public health policy concerning vaccines.
The Dominant Narrative
The dominant narrative, repeatedly reinforced via a wide range of channels, marketing, propaganda, and censorship – particularly during the SARS-CoV-2 outbreak- is that all vaccines, including the mRNA and adenovirus genetic therapy-based vaccines, are “safe and effective.” This typically unqualified but oft-repeated phrase has characteristics of a catechism of faith repeated by “true believers” of a vaccine-promoting cult of public health officers, academics dependent on the vaccine industry, industrial vaccinologists, the vast majority of specialist physician guilds (that universally accept funding from vaccine-manufacturing corporations), and their surrogates. Surrogates include corporate media, politicians, and academic journals that almost universally also accept significant direct or indirect funding from vaccine manufacturers. Any who question any aspect of this catechism are typically attacked, censored, and ostracized by cult members.
To illustrate with a recent example, these two terms (“safe and effective”) were repeatedly deployed and reinforced in corporate media and government messaging during the outbreak without defining or clarifying what criteria were being applied to define “safe” or “effective.” The repeated deployment and repetition of terms such as these without qualification or clarification as a key component of a public messaging campaign is a psychological manipulation tool known by the terms “neurolinguistic programming,” “natural language processing or technology,” or simply “subliminal marketing”, and relies on the use of messages designed to influence subconscious thoughts and behaviors without the audience’s conscious awareness. The use of censorship, nudge technology and other psychological manipulation methods to suppress discussion of potential harms and examination of risk/benefit/harm assessment and stratification by age and risk factors was justified as necessary to prevent “vaccine hesitancy” by the general public. Quite literally thousands of federally funded, peer-reviewed academic studies and publications examined and documented means by which ‘vaccine hesitancy” in the general public could be overcome using a wide range of propaganda, censorship, and psychological manipulation methods.
A false narrative of “vaccine hesitancy” creating risks of widespread unnecessary deaths due to infection by SARS-CoV-2 was justified, supported and promoted based on two subsidiary false narratives – 1) that SARS-CoV-2 infection was associated with a 3-4% “case fatality rate” (between 3 and 4 out of every one hundred people infected by SARS-CoV-2 would die), and 2) that the Emergency Use Authorized COVID “vaccines” were sufficiently protective to enable development of “herd immunity” if a sufficient fraction of the population would accept dosing with these products.
Like the dominant “safe and effective” narrative, these subsidiary false narratives upon which the primary dominant narrative rested were also repeated until the burden of “counterfactual” evidence became overwhelming. At that point, corporate media and government messaging was shifted to assert that these products would partially protect against severe disease and death. Strategically overlooked was that reduction in risk of severe disease and death were not listed as criteria in the Emergency Use Authorization or subsequent product marketing authorization by the US FDA. Over time, additional clinical research – notably from the Cleveland Clinic, a leading US provider of clinical services- indicated that any such benefits in reduction of clinical disease, disease severity, and death were short-lived and within weeks to months post product administration the risk of these outcomes increased relative to those that did not accept the products. This is referred to as “negative efficacy.”
In the current context of weaponization of the West Texas measles outbreak for various purposes, this dominant narrative has been repurposed and continues to be actively promoted by pivoting from COVID vaccine promotion of the childhood-focused 1960s legacy combination vaccine products Measles, Mumps and Rubella vaccines marketed as M-M-R II (Merck) and PRIORIX (GSK).
It has been my experience that the modern use of psychological manipulation (PsyWar), propaganda, censorship and marketing methods to reinforce this dominant vaccine narrative is so effective that most reporters and medical care providers do not even question whether this is true. It “feels” true to them, and therefore must be true.
In turn this profoundly influences both how front line journalists approach a ‘breaking news” story, and how medical care providers approach patient management. The baseline assumption being that if a patient that did not accept a “safe and effective” prophylactic vaccine develops a “vaccine preventable” infectious disease, then all clinical sequelae are the consequence of their failure to comply with the recommendation to accept the “safe and effective” vaccine product. The ultimate embodiment of this logic was that all who died with a positive PCR SARS-CoV-2 test during the COVID crisis died of COVID (despite any confounding medical conditions) rather than having died with COVID.
This recent post on “X” illustrates one consequence of the promotion and reinforcement of the dominant narrative in the context of measles and measles vaccines. Safe and effective. Apparently a case involving a physician who self-censors to avoid professional consequences despite being present with hard evidence of a case of vaccine-associated measles due to reversion of the vaccine strain to a disease-causing variant. Not perfectly safe and effective after all.
 |
Another example that contradicts the dominant “safe and effective” live attenuated measles vaccine narrative comes from a front-line primary care physician involved in managing West Texas outbreak-associated measles patients:
“Yes, I’ve treated fully vaccinated folks in their 20’s, 30’s, 40’s, and 50’s and even some children in Gaines County who went and got vaccinated at the health department’s recommendation and then got measles.”
Not perfectly safe and effective after all.
The Counter Narrative
The subdominant counter-narrative to “all vaccines are safe and effective” appears to have become “no vaccines are safe and effective.” This has also become a catechism for the alternative cult, one that has developed in reaction to the heavy-handed enforcement and widespread acceptance of the dominant narrative.
It should come as no surprise that this tenant of the “medical freedom movement” has developed in this way and no surprise that those who self-identify as being “medical freedom movement” warriors often self-identify as “the resistance” and will expel and delegitimize all those who reject this simplistic binary, either-or construct. This now extends even to their former champion HHS Secretary Robert Kennedy Jr., who has recently been labeled as a traitor to the cause (e.g., cult) for his statement as HHS Secretary that the best way to prevent the spread of measles is to vaccinate. This is a true statement – no alternative methods have proven to be more effective at slowing or stopping the spread of this highly infectious, very low-mortality disease. This is not the same as stating that measles vaccination is either fully safe or effective or that breakthrough cases or reversion to measles in vaccinated persons do not occur. RFK Jr. did not say that he recommended that people have their children vaccinated for measles. Yet that is what those who have accepted the counter-narrative heard, and many of them then launched campaigns to ostracize and delegitimize the HHS Secretary. Because, like in all cults, you are either for us or against us.
It is often assumed by those promoting the counter-narrative to this dominant catechism of all those who accept this storyline that all vaccines, including the childhood Measles, Mumps, and Rubella vaccines, are safe and effective have some sort of conflict of interest (COI) and that this COI extends down to individual reporters and medical care providers. In contrast, what I observe is that, although COI is rampant, in many cases, what one encounters is more akin to unthinking acceptance of the promoted dominant narrative as unquestioned truth. Or, to be more blunt, propaganda, censorship, psyops, and marketing work amazingly well on those who do not think for themselves.
Allow me to illustrate this with a recent example.
I was on a podcast discussing the West Texas measles outbreak when a phone call came in from West Texas. I responded with an automated text message that I was busy and would call back later. I immediately got a call from the same number, and I responded with another automated text message. The podcast concluded, and I called the number back. A young reporter for a West Texas-based newspaper wanted to question me about my original substack essay reporting that the “second measles death” was a second case of medical mismanagement of bacterial pneumonia. The reporter kept insisting that the hospital was saying otherwise and that this was a measles death. We went back and forth, her seeking some insight into who had tipped me off with the information that went into my initial report and my refusal to disclose my source. All of this concluded when I reprimanded her for taking the word of the hospital communications officer at face value and rather bluntly told her to seek out what was stated on the death certificate rather than relying on hospital PR at a time when the hospital was at risk for a medical malpractice/wrongful death lawsuit. I knew that neither the reporter nor the hospital had seen the death certificate because I knew that no death certificate had been issued at this time. However, it illustrated that, just as the managing physicians in the hospital had been biased by the dominant narrative regarding measles and measles vaccination, this young reporter had accepted that narrative without questioning the facts of the case. I very much doubt either the reporter or the managing physicians had accepted Pharma dollars to promote the dominant vaccine narrative. Still, they had become inadvertent allies in advancing and reinforcing that narrative.
The Sins of Binary Thought within the State
We are living in a time when virtually all issues in politics and public health are framed as binary. There is a right way or a wrong way to think. But life, science, and medicine are not binary, but rather more of a nuanced spectrum of information, ideas, opinion and truth. When framed as either A or B, then it becomes impossible to have a productive discussion or to negotiate nuanced public policy. And as if that is not bad enough, we are also living in a time when the State has assumed a role historically played by centralized religion. The State has assigned to itself the role of being arbiter of truth, to such a degree that information collected by the State which contradicts the approved truth will be suppressed. Suppose you find this discordant with your view of the State as a fair and balanced actor. In that case, I recommend that you look into the manipulation and deletion of adverse event data associated with the COVID genetic therapy-based products by those managing the Defense Medical Epidemiological Databased (DMED) or the CDC VAERS system.
The consequence of this simplistic, binary way of thinking, combined with the State assuming the role of being the ultimate arbiter of truth, is a sort of mass groupthink that creates barriers to effective policy decision-making in all aspects of political life. The consequences in public health are particularly stark and visible, but the same forces extend across the entire range of public policy.
Is There Another Way?
Both the pro-vaccine and the anti-vaccine cults will launch a withering social media firestorm on anyone who takes this position, but the inconvenient truth is that vaccines are helpful in some situations and not valuable for others. All vaccines, like all drugs, have side effects. In many cases, most if not all authorized vaccines have some degree of efficacy against the disease or infections they are purported to prevent. The issue should not be a binary argument between pro- vs anti-vaccine. This real issues are:
- What are the actual data supporting or refuting the usefulness of each individual vaccine? The true safety, effectiveness, and risk/benefit/harm analyses of each product stratified by age and co-morbidity. The only way to determine this is with solid, unbiased data, analyzed by people and processes that are free of bias. Fortunately or unfortunately, depending on your point of view, the COVID crisis has revealed and documented that open, transparent collection and analysis of the necessary public health and clinical trial data describing key safety and effectiveness characteristics of virtually all vaccines are not available. Furthermore, solid data on the true incidence and risks of virtually all “vaccine preventable” diseases are not available. Data gathered in compliance with modern standards, and with availability of modern medical care norms such as antibiotic treatment of secondary bacterial infections. Without such data, a valid assessment of risk/benefit stratified by age and co-morbidity is impossible. And so any statement that a given vaccine is either “safe and effective” or the contrary is invalid.
- Does the State have the right to impose a medical procedure on an individual without informed consent? Speaking personally, this is the issue that really got me fired up at the beginning of the COVID genetic therapy-based intervention campaign. I was under the illusion, reinforced by decades of training as a clinical researcher, regulatory specialist, and bioethicist that this had been decided by the post-WWII Nuremberg trials, US Belmont report, and the rich literature of modern clinical research bioethics. But this body of legal precedent, public policy, and academic study was thrown in the ash can at a moment’s notice in the face of the promoted false narrative of a severely inflated infectious disease threat. When this issue has been referred to the US Judiciary in various forms, it has predominantly acted to support the Murray Rothbard thesis that the role of the Judiciary is to support and legitimize the State. The Judiciary has not acted to ensure justice for those harmed, and it has not acted to support fundamental constitutional tenants concerning the rights of individuals. This issue must become a major focus of political discourse, but the constant framing of any related discourse as either pro- or anti-vaccine prevents this from happening.
In Conclusion
My advice? Take a step back and take a deep breath. Don’t get distracted by the chaos and promoted binary narratives. These artificially promoted cult-like positions primarily act to maintain stasis and prevent effective policy discussion and decisions. In other words, developing and driving cult-like behavior in support of extremist positions primarily serves to maintain status quo. This is likely to be intentional in a world where PsyWar techniques and technologies have become the norm.
The way out of the woods is to allow and enable objective, unbiased data to be gathered and analyzed. Then, make public health policy decisions based on those data. The current data are biased in various ways, and the interpretation of those data has not been objective or free of COI. In the meantime, neither trench warfare nor circular firing squads will permit or support effective public health policy decisions.
By the way, that happens to be the position taken by HHS Secretary Robert F. Kennedy Jr. to the best of my knowledge. We need more data, we need time to gather and analyze those data, and in the interim, we need to avoid exacerbating and inflaming the situation by yet more hasty, arbitrary, and capricious decision-making.
And we need the Judiciary to step up and defend the Constitution and individuals’ rights to bodily autonomy in a non-partisan manner.
Malone News is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
Invite your friends and earn rewards





-
 Business2 days ago
Business2 days agoCarney’s ‘major projects’ list no cause for celebration
-
 Business2 days ago
Business2 days agoGlobal elites insisting on digital currency to phase out cash
-
 Business2 days ago
Business2 days agoRed tape is killing Canadian housing affordability
-
 Health2 days ago
Health2 days agoMAiD should not be a response to depression
-
 Artificial Intelligence2 days ago
Artificial Intelligence2 days agoUK Police Chief Hails Facial Recognition, Outlines Drone and AI Policing Plans
-
 Business2 days ago
Business2 days agoOttawa’s so-called ‘Clean Fuel Standards’ cause more harm than good
-
 Business2 days ago
Business2 days agoThe Truth Is Buried Under Sechelt’s Unproven Graves
-
 International2 days ago
International2 days agoFrance records more deaths than births for the first time in 80 years