COVID-19
Supreme Court will not hear case about government’s violation of rights and freedoms


News release from the Justice Centre for Constitutional Freedoms
The Justice Centre for Constitutional Freedoms is disappointed that the Supreme Court of Canada has decided not to hear the appeal of the challenge to Manitoba’s lockdown restrictions. The decision was announced on Thursday, March 14, 2024.
The Leave to Appeal application, under the name Gateway Bible Baptist Church et al. v. Manitoba et al., was filed on September 18, 2023. Five Manitoba churches, a pastor and a deacon asked the Supreme Court of Canada to hear their appeal of the lower courts’ dismissal of their constitutional challenge to closures of churches and restrictions on outdoor gatherings during Covid lockdowns in late 2020 and 2021. Included in the application was protester Ross MacKay, who had been ticketed and who was seeking to appeal the lower courts’ dismissal of his constitutional challenge to the outdoor gathering limits.
Through public health orders, Manitoba had closed churches while permitting businesses to continue to operate. Taxis, in-person university classes, film and tv productions, law offices, and liquor stores were allowed to remain open. The Winnipeg Jets could meet and train indoors with their extended crew, and summer Olympic competitors were allowed to train indoors. Outdoor gatherings were reduced to no more than five people, while at the same time hundreds of people could legally gather indoors at big box stores.
The initial case was heard in May 2021 before the Manitoba Court of King’s Bench. The province did not produce any evidence that Covid spreads outdoors, or that outdoor gatherings were risky activities. That hearing did produce a significant admission from a government expert witness, Chief Microbiologist and Laboratory Specialist Dr. Jared Bullard, who, under questioning from Justice Centre lawyers, admitted that 56 percent of positive Covid cases were not infectious. The hearing was also notable for the Applicants’ expert report and testimony from world-renowned Stanford Professor, epidemiologist Dr. Jay Bhattacharya, co-author of The Great Barrington Declaration. Dr. Bhattacharya has moved on to even greater international fame as one of the litigants in a lawsuit, Missouri v. Biden, against the U.S federal government for medical censorship uncovered in The Twitter Files investigation.
The Manitoba Court of King’s Bench ruled that the government’s public health officials should not be “second guessed” and that the government need not meet a high threshold of providing persuasive evidence to demonstrably justify that violations of the Canadian Charter of Rights and Freedoms were reasonable. The Manitoba Court of King’s Bench did not order the unsuccessful Applicants to pay court costs, finding there to be significant public interest in having this case adjudicated.

In December 2022, the Applicants appealed. The appeal was dismissed by the Manitoba Court of Appeal in June 2023.
In the Application for Leave to Appeal to the Supreme Court of Canada, lawyers provided by the Justice Centre argued that the case raised issues of national importance. For instance:
- How are constitutionally protected activities to be juridically measured against comparable non-constitutionally protected activities? What is the proper approach to the minimal impairment stage of the Oakes analysis with respect to public health orders that fully prohibit Charter-protected activities (e.g. In- person religious worship) while permitting comparable non-Charter-protected activities (e.g. In-person university classes, film and television productions, indoor team-training for the Winnipeg Jets, etc.).
- Does reliance on the “precautionary principle” satisfy the state’s onus under Charter section 1 to provide “cogent and persuasive” evidence to justify Charter-infringing measures?
The Applicants’ legal team believed the case was critically important, as it could have served as guidance for governments in crafting public health measures on efforts needed to accommodate Charter-protected rights and freedoms.
Allison Pejovic, lawyer for the Applicants, stated, “Our clients are disappointed in the Supreme Court’s decision not to hear their appeal. It was past time to have a conversation with Canada’s highest court about whether Charter-protected rights such as rights to worship and assemble ought to be prioritized over economic interests, such as ensuring that the Winnipeg Jets could practice indoors and that movie productions could continue. It was also critical to hear from the Court on the importance of respecting the Charter during a declared ’emergency’. Governments urgently needed the Supreme Court of Canada’s guidance as to the degree to which they should accommodate Charter rights during a future pandemic or other emergency proclaimed by government. Leaving that issue undecided at the highest level is a grave injustice for all Canadians.”

From LifeSiteNews
The Justice Department attorney did not mention the Trump FDA’s recent admission linking the COVID shots to at least 10 child deaths so far.
The Trump Department of Justice (DOJ) is attempting to dismiss a whistleblower case against Pfizer over its COVID-19 shots, even as the Trump Food & Drug Administration (FDA) is beginning to admit their culpability in children’ s deaths.
As previously covered by LifeSiteNews, in 2021 the BMJ published a report on insider information from a former regional director of the medical research company Ventavia, which Pfizer hired in 2020 to conduct research for the company’s mRNA-based COVID-19 shot.
The regional director, Brook Jackson, sent BMJ “dozens of internal company documents, photos, audio recordings, and emails,” which “revealed a host of poor clinical trial research practices occurring at Ventavia that could impact data integrity and patient safety […] We also discovered that, despite receiving a direct complaint about these problems over a year ago, the FDA did not inspect Ventavia’s trial sites.”
According to the report, Ventavia “falsified data, unblinded patients, employed inadequately trained vaccinators, and was slow to follow up on adverse events reported in Pfizer’s pivotal phase III trial.” Overwhelmed by numerous problems with the trial data, Jackson filed an official complaint with the FDA.
Jackson was fired the same day, and Ventavia later claimed that Jackson did not work on the Pfizer COVID-19 shot trial; but Jackson produced documents proving she had been invited to the Pfizer trial team and given access codes to software relating to the trial. Jackson filed a lawsuit against Pfizer for violating the federal False Claims Act and other regulations in January 2021, which was sealed until February 2022. That case has been ongoing ever since.
Last August, U.S. District Judge Michael Truncale dismissed most of Jackson’s claims with prejudice, meaning they could not be refiled. Jackson challenged the decision, but the Trump DOJ has argued in court to uphold it, Just the News reports, with DOJ attorney Nicole Smith arguing that the case concerns preserving the government’s unfettered power to dismiss whistleblower cases.
The rationale echoes a recurring trend in DOJ strategy that Politico described in May as “preserving executive power and preventing courts from second-guessing agency decisions,” even in cases that involve “backing policies favored by Democrats.”
Jackson’s attorney Warner Mendenhall responded that the administration “really sort of made our case for us” in effectively admitting that DOJ is taking the Fair Claims Act’s “good cause” standard for state intervention to mean “mere desire to dismiss,” which infringes on his client’s “First Amendment right to access the courts, to vindicate what she learned.”
Mendenhall added that in a refiled case, Jackson “may be able to bring a very different case along the same lines, but with the additional information” to prove fraud, whereas rejection would send the message that “if fraud involves government complicity, don’t bother reporting it.”
That additional information would presumably include the FDA’s recent admission that at least 10 children the agency has reviewed so far “died after and because of receiving COVID-19 vaccination.”
“The truth is we do not know if we saved lives on balance,” admitted FDA Chief Medical Officer Vinay Prasad in a recent leaked email. “It is horrifying to consider that the U.S. vaccine regulation, including our actions, may have harmed more children than we saved. This requires humility and introspection.”
The COVID shots have been highly controversial ever since the first Trump administration’s Operation Warp Speed initiative prepared and released them in a fraction of the time any previous vaccine had ever been developed and tested. As LifeSiteNews has extensively covered, a large body of evidence has steadily accumulated over the past five years indicating that the COVID jabs failed to prevent transmission and, more importantly, carried severe risks of their own.
Ever since, many have intently watched and hotly debated what President Donald Trump would do about the situation upon his return to office. Though he never backed mandates like former President Joe Biden did, for years Trump refused to disavow the shots to the chagrin of his base, seeing Operation Warp Speed as one of his crowning achievements. At the same time, during his latest run he embraced the “Make America Healthy Again” movement and its suspicion of the medical establishment more broadly.
So far, Trump’s second administration has rolled back several recommendations for the shots but not yet pulled them from the market, despite hiring several vocal critics of the COVID establishment and putting the Department of Health & Human Services under the leadership of America’s most prominent anti-vaccine advocate, Robert F. Kennedy Jr. Most recently, the administration has settled on leaving the current jabs optional but not supporting work to develop successors.
In a July interview, FDA Commissioner Marty Makary asked for patience from those unsatisfied by the administration’s handling of the shots, insisting more time was needed for comprehensive trials to get more definitive data.
COVID-19
University of Colorado will pay $10 million to staff, students for trying to force them to take COVID shots

From LifeSiteNews
The University of Colorado Anschutz School of Medicine caused ‘life-altering damage’ to Catholics and other religious groups by denying them exemptions to its COVID shot mandate, and now the school must pay a hefty settlement.
The University of Colorado’s Anschutz School of Medicine must pay more than $10.3 million to 18 plaintiffs it attempted to force into taking COVID-19 shots despite religious objections, in a settlement announced by the religious liberty law firm the Thomas More Society.
As previously covered by LifeSiteNews, in April 2021, the University of Colorado (UC) announced its requirement that all staff and students receive COVID jabs, leaving specific policy details to individual campuses. On September 1, 2021, it enforced an updated policy stating that “religious exemption may be submitted based on a person’s religious belief whose teachings are opposed to all immunizations,” but required not only a written explanation why one’s “sincerely held religious belief, practice of observance prevents them” from taking the jabs, but also whether they “had an influenza or other vaccine in the past.”
On September 24, the policy was revised to stating that “religious accommodation may be granted based on an employee’s religious beliefs,” but “will not be granted if the accommodation would unduly burden the health and safety of other Individuals, patients, or the campus community.”
In practice, the school denied religious exemptions to Catholic, Buddhist, Eastern Orthodox, Evangelical, Protestant, and other applicants, most represented by Thomas More in a lawsuit contending that administrators “rejected any application for a religious exemption unless an applicant could convince the Administration that her religion ‘teaches (them) and all other adherents that immunizations are forbidden under all circumstances.’”
The UC system dropped the mandate in May 2023, but the harm had been done to those denied exemptions while it was in effect, including unpaid leave, eventual firing, being forced into remote work, and pay cuts.
In May 2024, a three-judge panel of the U.S. Tenth Circuit Court of Appeals rebuked the school for denying the accommodations. Writing for the majority, Judge Allison Eid found that a “government employer may not punish some employees, but not others, for the same activity, due only to differences in the employee’s religious beliefs.”
Now, Thomas More announces that year-long settlement negotiations have finally secured the aforementioned hefty settlement for their clients, covering damages, tuition costs, and attorney’s fees. It also ensured the UC will agree to allow and consider religious accommodation requests on an equal basis to medical exemption requests and abstain from probing the validity of applicants’ religious beliefs in the future.
“No amount of compensation or course-correction can make up for the life-altering damage Chancellor Elliman and Anschutz inflicted on the plaintiffs and so many others throughout this case, who felt forced to succumb to a manifestly irrational mandate,” declared senior Thomas More attorney Michael McHale. “At great, and sometimes career-ending, costs, our heroic clients fought for the First Amendment freedoms of all Americans who were put to the unconscionable choice of their livelihoods or their faith during what Justice Gorsuch has rightly declared one of ‘the greatest intrusion[s] on civil liberties in the peacetime history of this country.’ We are confident our clients’ long-overdue victory indeed confirms, despite the tyrannical efforts of many, that our shared constitutional right to religious liberty endures.”
On top of the numerous serious adverse medical events that have been linked to the COVID shots and their demonstrated ineffectiveness at reducing symptoms or transmission of the virus, many religious and pro-life Americans also object to the shots on moral grounds, due to the ethics of how they were developed.
According to a detailed overview by the pro-life Charlotte Lozier Institute, Pfizer, Moderna, and Johnson & Johnson all used fetal cells derived from aborted babies during their COVID shots’ testing phase; and Johnson & Johnson also used the cells during the design and development and production phases. The American Association for the Advancement of Science’s journal Science and even the left-wing “fact-checking” outlet Snopes have also admitted the shots’ abortion connection, which gives many a moral aversion to associating with them.
Catholic World Report notes that similarly large sums have been won in other high-profile lawsuits against COVID shot mandates, including $10.3 million to more than 500 NorthShore University HealthSystem employees in 2022 and $12.7 million to a Catholic Michigander fired by Blue Cross Blue Shield in 2024.


Wayne Gretzky’s Terrible, Awful Week.. And Soccer/ Football.

Western Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns
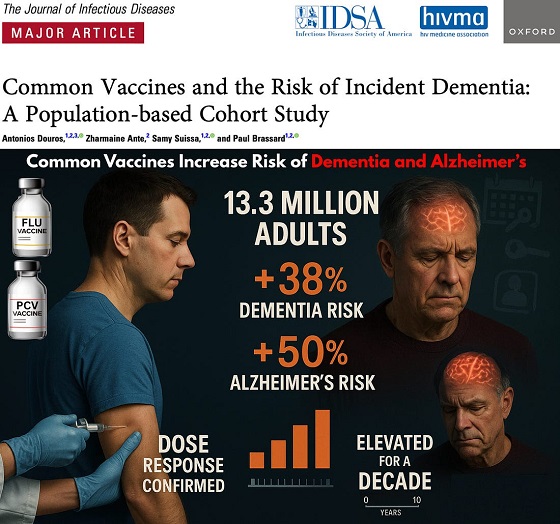
Common Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s

The $50 Billion Question: EVs Never Delivered What Ottawa Promised
-
COVID-192 days ago
Trump DOJ seeks to quash Pfizer whistleblower’s lawsuit over COVID shots
-
 Alberta2 days ago
Alberta2 days agoAlberta introducing three “all-season resort areas” to provide more summer activities in Alberta’s mountain parks
-
 Agriculture2 days ago
Agriculture2 days agoGrowing Alberta’s fresh food future
-
 International2 days ago
International2 days agoTrump admin wants to help Canadian woman rethink euthanasia, Glenn Beck says
-
 Alberta2 days ago
Alberta2 days agoThe case for expanding Canada’s energy exports
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoOttawa’s New Hate Law Goes Too Far
-
 Business2 days ago
Business2 days agoFuelled by federalism—America’s economically freest states come out on top
-
 Automotive1 day ago
Automotive1 day agoPoliticians should be honest about environmental pros and cons of electric vehicles