Health
Quitting Coffee: Roasting the coffee bean out of my life



Roasting the coffee bean out of my life.
It was a regular morning when I overreacted. Now usually I’m calm, composed, I’m the guy that lets things slide off my shoulder. But on this day, I became a linguist of profanity. It’s not someone I feel I am in my core or someone I consciously strive to be.

I was triggered, triggered by the way my body reacted to the caffeine; it was time to give up coffee.
As a business owner, I get clients that request meetings with me all the time, and who’s business is dependant on the melding of minds, I’m always meeting clients for the first time at trendy coffee shops. So kicking the coffee cup was a conscious decision. Something of which I thought of for a while, but my lack of focus prevented me from achieving the perk-free focus I wanted.
Now, I love coffee, and I have since my mid-twenties since I purchased an espresso machine, which I used for a few months before stuffing it in my cabinet. You see, it wasn’t just the coffee I loved or the caffeine I craved, but I loved the coffee shop culture. It was hip, cool, filled with busy, successful-looking people.
With every order, my inner voice always questioning, “hmm, I wonder what all these $6.50 coffees are doing to my body, should I worry?” or another question I’d ask myself, “am I an addict? Nah,” I’d shrug inside, as I placed an order for a drip coffee with room.
I convinced myself I had my coffee intake under control because I only consumed it around my business meetings, which were, on average, up to 3 times a day. And the caffeine karma was always clean because I would offer to pick up the bill for clients I would meet. “no-no, it’s ok. I got this!” It was full of warm goodness, positive energy over discussions of our software project together, or next movie production, and ideas seemed to explode.
Things changed. It started to become a problem because my want for coffee was percolating between meetings. A promise I made to myself that I’d only consume coffee during meetings, I figured, if I were going to have a bad habit, it would be while I’m going to be productive.
My days started with a morning coffee with my wife during breakfast, then I’d grab a quick cup to sip while coding a software project, or filming, which I’d have close to me on set in a to-go cup, and times it was at night when visiting with friends or family.
It’s only been three days since I’ve quit, it’s been the three most productive days of my life. That’s why I’ve chosen to write this article. I love to write, but while in my coffee-addicted anxious haze, I always had that false sense that I never had the time. But since I’ve quit the bean, I’ve felt present, focused, and just…happy. And now that I’m #CaffeineSober, I realized what coffee and the caffeine in it did to me. I’m sharing this because, a quick google search, I couldn’t find a decent article I could connect with, so I thought I’d write one.
I’m well aware the drug affects people in different ways, but my coffee consumption made me:
- foggy in my mind
- feel like I never had enough time
- react or overreact to stressful events
- feel like I was carrying the weight of the world’s projects
- feel distant from my wife and kids
- feel like I couldn’t handle my daily stress loads and would push myself to get through them.
- not find the joy in the admin tasks of my business, like invoicing, or writing an article like this.
- not want to go to the gym because I would see a workout as an unachievable entire body, two-hour commitment, where now I see them as more focused, micro workouts.
- feel bloated around my waistline
The list goes on, but I didn’t feel GOOD.
I enjoy my coffee with lots of cream and lots of honey. I suspect there’s a possible combination of the three, caffeine, dairy, and sugar, a triple whammy of things which are affecting my mental health, and something I’m going to be tracking, but that’s an entirely different article. But for now, I’m enjoying a flatter stomach as well.
I’m not basing my article off any science. But there seems to be a common observation of the side effects of coffee. According to WebMD, coffee containing caffeine can cause insomnia, nervousness, and restlessness, stomach upset, nausea and vomiting, increased heart and breathing rate, and other side effects.
And if you hold a celebrity’s opinion as an expert’s, here’s an article. Harry Quits Alcohol, Tea, and Coffee for New Year as Meghan’s Healthy Lifestyle Rubs Off
I’m not arguing about the benefits either. I’m sharing my own experience in hopes that if you’re like me, there’s nothing wrong with finding the solution for your happiness.
Roasting the bean from my life hasn’t taken the joy out of meeting clients at trendy coffee shops — sipping something over discussions about video game development, software development, and movie production projects. I’ve switched to teas, I still pick up the bill, and my days are a bit brighter, and my resting-smile-face just a bit larger.
Tell me how quitting coffee has made you feel?
Raoul Bhatt
https://www.facebook.com/BhattTech/
About me, the Author:
I began my career as a graphic artist when I was still in high school, then followed with eight years of developing software before having the courage to create my own Windows XP based software in the mid 2005s with the goal of licensing it to users around the world. During that time, I had a secret passion for film, and making shortfilms and music videos, of which I wasn’t public about…. Fast forward to 2019. I’ve accumulated nearly a million users of my softwares, and developed over 2000 unique projects of which I’ve spent as the writer for, leading and developing my skills for the larger projects I create today which I post frequently on my channels.

From the Fraser Institute
By Nadeem Esmail and Mackenzie Moir
It’s an exciting time in Canadian health-care policy. But even the slew of new reforms in Alberta only go part of the way to using all the policy tools employed by high performing universal health-care systems.
For 2026, for the sake of Canadian patients, let’s hope Alberta stays the path on changes to how hospitals are paid and allowing some private purchases of health care, and that other provinces start to catch up.
While Alberta’s new reforms were welcome news this year, it’s clear Canada’s health-care system continued to struggle. Canadians were reminded by our annual comparison of health care systems that they pay for one of the developed world’s most expensive universal health-care systems, yet have some of the fewest physicians and hospital beds, while waiting in some of the longest queues.
And speaking of queues, wait times across Canada for non-emergency care reached the second-highest level ever measured at 28.6 weeks from general practitioner referral to actual treatment. That’s more than triple the wait of the early 1990s despite decades of government promises and spending commitments. Other work found that at least 23,746 patients died while waiting for care, and nearly 1.3 million Canadians left our overcrowded emergency rooms without being treated.
At least one province has shown a genuine willingness to do something about these problems.
The Smith government in Alberta announced early in the year that it would move towards paying hospitals per-patient treated as opposed to a fixed annual budget, a policy approach that Quebec has been working on for years. Albertans will also soon be able purchase, at least in a limited way, some diagnostic and surgical services for themselves, which is again already possible in Quebec. Alberta has also gone a step further by allowing physicians to work in both public and private settings.
While controversial in Canada, these approaches simply mirror what is being done in all of the developed world’s top-performing universal health-care systems. Australia, the Netherlands, Germany and Switzerland all pay their hospitals per patient treated, and allow patients the opportunity to purchase care privately if they wish. They all also have better and faster universally accessible health care than Canada’s provinces provide, while spending a little more (Switzerland) or less (Australia, Germany, the Netherlands) than we do.
While these reforms are clearly a step in the right direction, there’s more to be done.
Even if we include Alberta’s reforms, these countries still do some very important things differently.
Critically, all of these countries expect patients to pay a small amount for their universally accessible services. The reasoning is straightforward: we all spend our own money more carefully than we spend someone else’s, and patients will make more informed decisions about when and where it’s best to access the health-care system when they have to pay a little out of pocket.
The evidence around this policy is clear—with appropriate safeguards to protect the very ill and exemptions for lower-income and other vulnerable populations, the demand for outpatient healthcare services falls, reducing delays and freeing up resources for others.
Charging patients even small amounts for care would of course violate the Canada Health Act, but it would also emulate the approach of 100 per cent of the developed world’s top-performing health-care systems. In this case, violating outdated federal policy means better universal health care for Canadians.
These top-performing countries also see the private sector and innovative entrepreneurs as partners in delivering universal health care. A relationship that is far different from the limited individual contracts some provinces have with private clinics and surgical centres to provide care in Canada. In these other countries, even full-service hospitals are operated by private providers. Importantly, partnering with innovative private providers, even hospitals, to deliver universal health care does not violate the Canada Health Act.
So, while Alberta has made strides this past year moving towards the well-established higher performance policy approach followed elsewhere, the Smith government remains at least a couple steps short of truly adopting a more Australian or European approach for health care. And other provinces have yet to even get to where Alberta will soon be.
Let’s hope in 2026 that Alberta keeps moving towards a truly world class universal health-care experience for patients, and that the other provinces catch up.

From LifeSiteNews
Dr. Marty Makary took aim at the transgender-medical-industrial complex that has exploded in recent years during a recent press conference.
Food and Drug Administration (FDA) commissioner Dr. Marty Makary has sternly warned companies manufacturing “breast binders” to cease marketing and supplying their product to gender-confused girls seeking to make their bodies appear masculine.
“Today the FDA is taking action,” said Makary in a press conference. “We are sending warning letters to 12 manufacturers and retailers for illegal marketing of breast binders for children, for the purposes of treating gender dysphoria.”
“Breast binders are a class one medical device with legitimate medical users, such as being used by women after breast cancer surgery,” but “these binders are not benign,” he cautioned. “Long-term usage has been associated with pain, compromised lung function, and even difficulty breast feeding later in life.”
“The warning letters will formally notify the companies of their significant regulatory violations and require prompt corrective action,” said the FDA head.
.@DrMakaryFDA: “Today the FDA is taking action. We are sending warning letters to 12 manufacturers and retailers for illegal marketing of breast binders for children, for the purposes of treating gender dysphoria.” pic.twitter.com/6JNAy36223
— HHS Rapid Response (@HHSResponse) December 18, 2025
The warning letter addressed to California manufacturer, GenderBender, notes that the company’s website states that “[c]hest binding is the practice of compressing breast mass into a more masculine shape, often done in the LGBTQ community for gender euphoria.”
“Your firm should take prompt action to address any violations identified in this letter. Failure to adequately address this matter may result in regulatory action being initiated by the FDA without further notice. These actions include, but are not limited to, seizure and injunction,” advised the FDA.
During his presentation, Makary took aim at the transgender-medical-industrial complex that has exploded in recent years.
“One of the most barbaric features of a society is the genital mutilation of its children,” observed Makary.
“Pushing transgender ideology in children is predatory, it’s wrong, and it needs to stop,” he declared.
“This ideology is a belief system that some teachers, some pediatricians, and others are selling to children without their parents knowing sometimes, or with a deliberate attempt to remove parents from the decision making,” Makary explained.
To witness society “putting kids on a path of chest binders, drugs, castration, mastectomies, and other procedures is a path that now many kids regret,” he lamented, as he pointed to Chloe Cole, who has reverted to her God-given femininity after undergoing so-called “gender-affirming” surgery as a teen.
Cole is a leading voice for young people who have “detransitioned” after having medically, surgically, and socially attempted to “transition” to a member of the opposite sex.
.@DrMakaryFDA: “Pushing transgender ideology in children is predatory, it's wrong, and it needs to stop.” pic.twitter.com/TXxWNEtNZk
— HHS Rapid Response (@HHSResponse) December 18, 2025


Ottawa-Alberta agreement may produce oligopoly in the oilsands

Warning Canada: China’s Economic Miracle Was Built on Mass Displacement

‘The electric story is over’

The Top News Stories That Shaped Canadian Energy in 2025 and Will Continue to Shape Canadian Energy in 2026

The Climate Argument Against Livestock Doesn’t Add Up
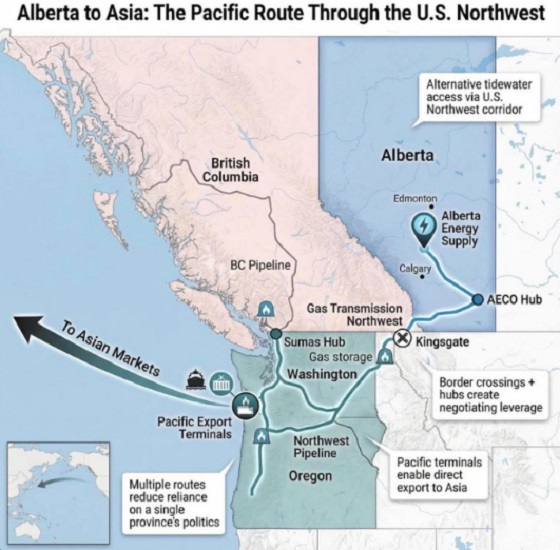
What are the odds of a pipeline through the American Pacific Northwest

Calgary’s new city council votes to ban foreign flags at government buildings
-
 Haultain Research2 days ago
Haultain Research2 days agoSweden Fixed What Canada Won’t Even Name
-
 Business2 days ago
Business2 days agoWhat Do Loyalty Rewards Programs Cost Us?
-
 Business1 day ago
Business1 day agoLand use will be British Columbia’s biggest issue in 2026
-
 Energy21 hours ago
Energy21 hours agoRulings could affect energy prices everywhere: Climate activists v. the energy industry in 2026
-
 International21 hours ago
International21 hours agoChina Stages Massive Live-Fire Encirclement Drill Around Taiwan as Washington and Japan Fortify
-
 Digital ID20 hours ago
Digital ID20 hours agoThe Global Push for Government Mandated Digital IDs And Why You Should Worry
-
 Business18 hours ago
Business18 hours agoFeds pull the plug on small business grants to Minnesota after massive fraud reports
-
 Business7 hours ago
Business7 hours agoDOOR TO DOOR: Feds descend on Minneapolis day cares tied to massive fraud
You must be logged in to post a comment Login