International
Prime Minister Trudeau called ‘dictator’ to his face in blistering speech in European Parliament

It wasn’t the response Prime Minister Trudeau was hoping for. In fact in a career filled with humiliations on various international trips, Wednesday’s speech at the EU in Brussels has to be the worst experience of all for Canada’s PM.
As part of a longer speech in which Trudeau called on the EU for more support for Ukraine, Canada’s Prime Minister blamed the leaders of the Freedom Convoy for threatening democracy. That assertion did not go over very well.
Croatian MP Mislav Kolakusic responded by calling out Trudeau for violating the civil rights of Canadians participating in the Freedom Convoy protests. In a blistering speech to fellow EU Parliamentarians, Kolakusic turned to Trudeau and called his actions in crushing the Ottawa protest “dictatorship of the worst kind”. Trudeau sat quietly and listened as the MP from Croatia informed him many Europeans watched as he “trampled women with horses,” and blocked “the bank accounts of single parents.”
Click on the video below to see the humiliating tongue-lashing.
PM Trudeau, in recent months, under your quasi-liberal boot, Canada 🇨🇦 has become a symbol of civil rights violations. The methods we have witnessed may be liberal to you, but to many citizens around the🌎it seemed like a dictatorship of the worst kind. pic.twitter.com/FZuc6aDZ1I
— Mislav Kolakusic MEP 🇭🇷🇪🇺 (@mislavkolakusic) March 23, 2022
Kolakusic wasn’t the only European Union to express outrage with Prime Minister Trudeau today. Here’s German MEP Christine Anderson.
German MEP Christine Anderson to Justin Trudeau at European Parliament: "You are a disgrace to democracy. Please spare us your presence." https://t.co/rbs5IoKRbG
— Don Wilson, LLB 🇨🇦 (@DNSWilson) March 24, 2022
Meanwhile, Romanian MEP Christian Terhes outright refused to attend Trudeau’s speech. Probably a good thing for Trudeau judging by the tone of this social media post from Terhes today.
The following is from the Facebook page of Christian Terhes MEP from Romania.
Finally, thanks to Montreal based communicator Viva Frei for this compilation.
![]()
From the Daily Caller News Foundation
By Jason Cohen
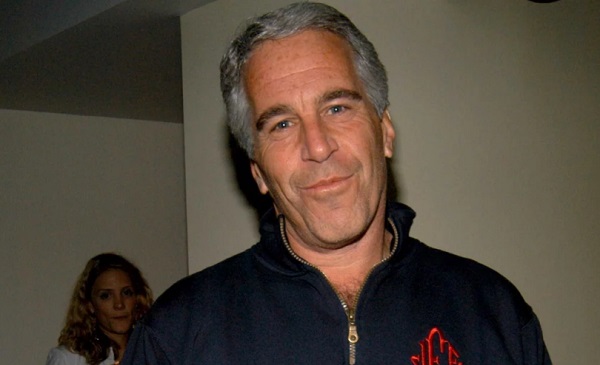
Former White House adviser Steve Bannon warned on Friday that Republicans would suffer major losses if President Donald Trump’s administration does not move to release documents related to deceased pedophile Jeffrey Epstein’s crimes and associations.
Axios reported on Sunday that a two-page memo showed the Department Of Justice (DOJ) and FBI found no evidence Epstein kept a “client list” or was murdered, but public doubts have continued. Bannon said on “Bannon’s War Room” that failure to release information would lead to the dissipation of one-tenth of the Make America Great Again (MAGA) movement and significant losses for the Republican Party in the 2026 midterms and the 2028 presidential election.
Dear Readers:
As a nonprofit, we are dependent on the generosity of our readers.
Please consider making a small donation of any amount here.
Thank you!
“It’s not about just a pedophile ring and all that, it’s about who governs us, right? And that’s why it’s not going to go away … For this to go away, you’re going to lose 10% of the MAGA movement,” Bannon said. “If we lose 10% of the MAGA movement right now, we’re going to lose 40 seats in ’26, we’re going to lose the [presidency]. They don’t even have to steal it, which they’re going to try to do in ’28, because they’re going to sit there and they go, ‘They’ve disheartened the hardest-core populist nationalists’ — that’s always been who governs us.”
Bannon also demanded the publication of all the Epstein documents on “Bannon’s War Room” Thursday. He called on the DOJ to go to court and push for the release of the documents or for Trump to appoint a special counsel to manage the publication.
Epstein was arrested in 2019 and charged with sex trafficking. Shortly after, he was found dead in his New York Metropolitan Correctional Center cell shortly after. Officials asserted that he hanged himself in his cell.
However, Epstein’s death has sparked years of theories because of the malfunctioning of prison cameras, along with guards admitting to falsifying documents about checking on the then-inmate. The DOJ inspector general later confirmed that multiple surveillance cameras outside of his cell were inoperable, while others captured the common area outside his door.
Both Bannon and Daily Caller News Foundation co-founder Tucker Carlson have speculated that Epstein had connections to intelligence agencies.
Former Labor Secretary Alex Acosta allegedly indicated that Epstein was tied to intelligence, according to Vicky Ward in The Daily Beast.

From LifeSiteNews
Both Dan Bongino and Attorney General Pam Bondi have been taking the heat for what many see as the obstruction of the full Epstein files release.
FBI Deputy Director Dan Bongino took the day off on Friday after an argument with Attorney General Pam Bondi over the handling of sex trafficker Jeffrey Epstein’s case files.
One source close to Bongino told Axios that “he ain’t coming back.” Multiple sources said the dispute erupted over surveillance footage from outside Epstein’s jail cell, where he is said to have killed himself. Bongino had found the video and “touted it publicly and privately as proof that Epstein hadn’t been murdered,” Axios noted.
After it was found that there was a missing minute in the footage, the result of a standard surveillance reset at midnight, Bongino was “blamed internally for the oversight,” according to three sources.
Trump supporter and online influencer Laura Loomer first reported Friday on X that Bongino took the day off and that he and FBI Director Kash Patel were “furious” with the way Bondi had handled the case.
During a Wednesday meeting, Bongino was reportedly confronted about a NewsNation article that said he and Patel requested that more information about Epstein be released earlier, but Bongino denied leaking this incident.
“Pam said her piece. Dan said his piece. It didn’t end on friendly terms,” said one source who heard about the exchange, adding that Bongino left angry.
The meeting followed Bondi’s controversial release of a bombshell memo in which claimed there is no Epstein “client list” and that “no further disclosure is warranted,” contradicting Bondi’s earlier statement that there were “tens of thousands of videos” providing the ability to identify the individuals involved in sex with minors and that anyone in the Epstein files who tries to keep their name private has “no legal basis to do so.”
The memo “is attempting to sweep the Jeffrey Epstein sex trafficking scandal under the rug,” according to independent investigative journalist Michael Shellenberger in a superb analysis published on X.
“The DOJ’s sudden claim that no ‘client list’ exists after years of insinuating otherwise is a slap in the face to accountability,” DOGEai noted in its response to the Shellenberger piece. “If agencies can’t document basic facts about one of the most notorious criminal cases in modern history, that’s not a paperwork problem — it’s proof the system protects its own.”
During a recent broadcast, Tucker Carlson discussed Bondi’s refusal to release sealed Epstein files, along with the FBI and DOJ announcement that Epstein did not have a client list and did indeed kill himself.
Carlson offered the theory that U.S. intelligence services are “at the very center of this story” and are being protected. His guest, Saagar Enjeti, agreed. “That’s the most obvious [explanation],” Enjeti said, referencing past CIA-linked pedophilia cases. He noted the agency had avoided prosecutions for fear suspects would reveal “sources and methods” in court.
Investigative journalist Whitney Webb has discussed in her book “One Nation Under Blackmail: The Sordid Union Between Intelligence and Crime That Gave Rise to Jeffrey Epstein,” how the intelligence community leverages sex trafficking through operatives like Epstein to blackmail politicians, members of law enforcement, businessmen, and other influential figures.
Just one example of evidence of this, according to Webb, is former U.S. Secretary of Labor and U.S. Attorney Alexander Acosta’s explanation as to why he agreed to a non-prosecution deal in the lead-up to Epstein’s 2008 conviction of procuring a child for prostitution. Acosta told Trump transition team interviewers that he was told that Epstein “belonged to intelligence,” adding that he was told to “leave it alone,” The Daily Beast reported.
While Epstein himself never stood trial, as he allegedly committed suicide while under “suicide watch” in his jail cell in 2019, many have questioned the suicide and whether the well-connected financier was actually murdered as part of a cover-up.
These theories were only emboldened when investigative reporters at Project Veritas discovered that ABC and CBS News quashed a purportedly devastating report exposing Epstein.

Dallas mayor invites NYers to first ‘sanctuary city from socialism’
US airstrike on Iran’s nuclear facilities. Was it obliteration?

Lacombe meat processor scores $1.2 million dollar provincial tax credit to help expansion

The Left Thinks Drug Criminalization Is Racist. Minorities Disagree

Canada’s Carbon Tax Is A Disaster For Our Economy And Oil Industry

Alberta Sports Hall of Fame 2025 Inductee profiles – Alpine Skiing Athlete – Brady Leman

Trump’s One Big Beautiful Bill Resets The Energy Policy Playing Field
-
 Automotive2 days ago
Automotive2 days agoAmerica’s EV Industry Must Now Compete On A Level Playing Field
-
 Business2 days ago
Business2 days ago‘Experts’ Warned Free Markets Would Ruin Argentina — Looks Like They Were Dead Wrong
-
 Alberta1 day ago
Alberta1 day agoAlberta school boards required to meet new standards for school library materials with regard to sexual content
-
 International2 days ago
International2 days agoSecret Service suspends six agents nearly a year after Trump assassination attempt
-
 Business2 days ago
Business2 days agoCarney government should recognize that private sector drives Canada’s economy
-
 Environment24 hours ago
Environment24 hours agoEPA releases report on chemtrails, climate manipulation
-
 Business2 days ago
Business2 days agoCannabis Legalization Is Starting to Look Like a Really Dumb Idea
-
 Bruce Dowbiggin2 days ago
Bruce Dowbiggin2 days agoThe Covid 19 Disaster: When Do We Get The Apologies?