Alberta
Graven Images: The Greening Of Calgary

The city of Calgary this week elected the first woman mayor in its history. This is a source of great satisfaction to those citizens who cringe at Calgary’s image as part buckaroo/ part bitumen cowboy. The fact that Jyoti Gondek is of Pashtun origin only deepens the sense of accomplishment for the urban elite of Calgary.
How giddy are the wokesters? A CBC reporter illustrated the story with a tweet showing a long series of emoji men followed by a single emoji of a woman. Because journalistic objectivity at the national broadcaster demands a clever tweet. “Look what we’ve done, world! Woman! Punjabi! Now we can hold our heads up in the polite society of the urban hives.”
The new mayor has a PhD in urban sociology which “furnishes understanding of the complex as well as profound meaning of every urban reality, notably the territorial stabilization of social life, the rise of a space symbol system and culture, and the origin and evolution of human settlements.”
Which sounds like the sort of convoluted stuff that Wokesters toss around when they’re trying to distance themselves from the Stampede crowd. What it means in reality is that Gondek will commit $250 K to declare a climate emergency in Calgary as her first priority as mayor. As this photo below shows, it’s not a moment too soon.

Can she tame the city’s transit snarls and stare down a council bent on destroying the budget? Who knows? Who cares? The natural gas/ petroleum bastards will now have to take a knee to the symbolism of her outreach to Big Climate. And that’s enough.
Okay, it’s just a mayor in a mid-sized Canadian city, but you have to start with small dreams if you’re going to make the world a progressive paradise. Especially when, like Gondek, you spend every working day cloying with guilt over how Calgary’s energy industry is ravaging Mother Earth.
The big Green virtue dreams are the ones about to be dreamt in Glasgow in the next weeks as the world’s guiltiest liberals— aka the IPCC— convene to reconstitute the world economy by killing fossil fuels. If this all sounds familiar it’s because the Al Gores and Neil Youngs have been hard at this project for decades, sending thunderbolts of doom via a captive media. (Sample: 1987: NASA’s James Hansen predicts world 3C warmer by 2020. Reality: average temp only 0.44C higher.) And lots more faceplants.
No matter. The evolution of Green is a litany of half-baked predictions and salacious slanders. Even as European governments scramble to replace their sacred renewable dreams with the realities of nuclear power or, gasp, Russian natural gas, the pious will still party like it’s 1999— when all things seemed possible. There’s a revolution of purity happening here, folks, and a few inconvenient facts isn’t going to harsh the vibe.
The vibe, of course, is not climate change or even first women mayors. The vibe is victim culture, re-fitting Marxism so the uncouth and intemperate opposition can be permanently rendered inert. If Marx’s wealth re-distribution is to happen equity— not just equality— must be achieved. Any weapon at hand— climate, gender, victimization— will serve to get there.
The old Commie’s theories just need a new coat of victim’s paint to make them current. Author Chris Rufo explains how the Left is making the quick flip after their Cold War dreams died in the ‘70s at the altar of capitalist riches. : “… rather than abandon their political project, Marxist scholars in the West simply adapted their revolutionary theory to the social and racial unrest of the 1960s. Abandoning Marx’s economic dialectic of capitalists and workers, they substituted race for class and sought to create a revolutionary coalition of the dispossessed based on racial and ethnic categories.”
Suddenly, it’s all victims, all the time.
Thus the new liturgy, funded by Big Tech oligarchs such as Mark Zuckerberg and Bill Gates. Capitalist roaders are failed humans. Writes Christopher Chantrill: “Today’s elites are totally down as Allies of the Oppressed Peoples. Their political power is justified by their untiring support of and advocacy for The Victims.”
Andrea Widburg describes the role reversal in The American Thinker: “In its new iteration, Whites are irredeemably racist and evil. Equality is a trap because White societal dominance means that the other races (and sexualities) will never be able to catch up. Forced equity is the only answer, and one way to pave the way for that to happen is to force Whites to remove themselves from society, from the economy, from politics, and from any other area in which they can be seen to have an advantage.”
Celebrating the ascent of symbolism, not the skill-set of politicians such as Barack Obama (and the removal of statues) is how whites willingly remove themselves from the economy and society. As Rufo tweets, “@LockheedMartin, the nation’s largest defense contractor, sent key executives to a three-day white male reeducation camp in order to deconstruct their “white male culture” and atone for their “white male privilege.”
To the surprise of the Marxists, their old enemies on Wall Street are enthusiastically taking the bait. Now they have only the rump opposition of libertarians and stubborn conservatives left to hammer into shape and the Bernie Sanders revolution, begun in the ‘60s, will be complete.
Calgary will be so proud.
Bruce Dowbiggin @dowbboy is the editor of Not The Public Broadcaster (http://www.notthepublicbroadcaster.com). The best-selling author of Cap In Hand is also a regular contributor to Sirius XM Canada Talks Ch. 167. A two-time winner of the Gemini Award as Canada’s top television sports broadcaster, his new book with his son Evan is called InExact Science: The Six Most Compelling Draft Years In NHL History is now available on http://brucedowbigginbooks.ca/book-personalaccount.aspx

From LifeSiteNews
‘I think the court was in error,’ Alberta Premier Danielle Smith has said. ‘There will be irreparable harm to children who get sterilized.’
LGBT activists have won an injunction that prevents the Alberta government from restricting “gender transitions” for children.
On June 27, Alberta King’s Court Justice Allison Kuntz granted a temporary injunction against legislation that prohibited minors under the age of 16 from undergoing irreversible sex-change surgeries or taking puberty blockers.
“The evidence shows that singling out health care for gender diverse youth and making it subject to government control will cause irreparable harm to gender diverse youth by reinforcing the discrimination and prejudice that they are already subjected to,” Kuntz claimed in her judgment.
Kuntz further said that the legislation poses serious Charter issues which need to be worked through in court before the legislation could be enforced. Court dates for the arguments have yet to be set.
READ: Support for traditional family values surges in Alberta
Alberta’s new legislation, which was passed in December, amends the Health Act to “prohibit regulated health professionals from performing sex reassignment surgeries on minors.”
The legislation would also ban the “use of puberty blockers and hormone therapies for the treatment of gender dysphoria or gender incongruence” to kids 15 years of age and under “except for those who have already commenced treatment and would allow for minors aged 16 and 17 to choose to commence puberty blockers and hormone therapies for gender reassignment and affirmation purposes with parental, physician and psychologist approval.”
Just days after the legislation was passed, an LGBT activist group called Egale Canada, along with many other LGBT organizations, filed an injunction to block the bill.
In her ruling, Kuntz argued that Alberta’s legislation “will signal that there is something wrong with or suspect about having a gender identity that is different than the sex you were assigned at birth.”
She further claimed that preventing minors from making life-altering decisions could inflict emotional damage.
However, the province of Alberta argued that these damages are speculative and the process of gender-transitioning children is not supported by scientific evidence.
“I think the court was in error,” Alberta Premier Danielle Smith said on her Saturday radio show. “That’s part of the reason why we’re taking it to court. The court had said there will be irreparable harm if the law goes ahead. I feel the reverse. I feel there will be irreparable harm to children who get sterilized at the age of 10 years old – and so we want those kids to have their day in court.”
READ: Canadian doctors claim ‘Charter right’ to mutilate gender-confused children in Alberta
Overwhelming evidence shows that persons who undergo so-called “gender transitioning” procedures are more likely to commit suicide than those who are not given such irreversible surgeries. In addition to catering to a false reality that one’s sex can be changed, trans surgeries and drugs have been linked to permanent physical and psychological damage, including cardiovascular diseases, loss of bone density, cancer, strokes and blood clots, and infertility.
Meanwhile, a recent study on the side effects of “sex change” surgeries discovered that 81 percent of those who have undergone them in the past five years reported experiencing pain simply from normal movements in the weeks and months that followed, among many other negative side effects.
Alberta
Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

Alberta’s Chief Electoral Officer, Gordon McClure, has issued a Notice of Initiative Petition.
This confirms a Citizen Initiative application has been received and the Chief Electoral Officer has determined the requirements of section 2(3) of the Citizen Initiative Act have been met.
Approved Initiative Petition Information
The approved citizen initiative application is for a policy proposal with the following proposed question:
Do you agree that Alberta should remain in Canada?
The Notice of Initiative Petition, application, and statement provided by the proponent are available on Elections Alberta’s website on the Current Initiatives Petition page.
As the application was received and approved prior to coming into force of Bill 54: Election Statutes Amendment Act, the Citizen Initiative process will follow requirements set out in the Citizen Initiative Act as of June 30, 2025.
Next Steps
- The proponent must appoint a chief financial officer within 30 days (by July 30, 2025).
- Once the 30-day publication period is complete and a chief financial officer has been appointed, Elections Alberta will:
- issue the citizen initiative petition,
- publish a notice on the Current Initiatives Petition page of our website indicating the petition has been issued, specifying the signing period dates, and the number of signatures required for a successful petition, and
- issue the citizen initiative petition signature sheets and witness affidavits. Signatures collected on other forms will not be accepted.
More information on the process, the status of the citizen initiative petition, financing rules, third party advertising rules, and frequently asked questions may be found on the Elections Alberta website.
Elections Alberta is an independent, non-partisan office of the Legislative Assembly of Alberta responsible for administering provincial elections, by-elections, and referendums.

So Alberta, what’s next?

The Physics Behind The Spanish Blackout

War over after 12 days? Ceasefire reached between Israel, Iran

Canada should already be an economic superpower. Why is Canada not doing better?

Alberta Next Takes A Look At Alberta Provincial Police Force

‘Transgender’ males have 51% higher death rate than general population: study

President Xi Skips Key Summit, Adding Fuel to Ebbing Power Theories
-
 Brownstone Institute2 days ago
Brownstone Institute2 days agoFDA Exposed: Hundreds of Drugs Approved without Proof They Work
-
 Energy1 day ago
Energy1 day agoChina undermining American energy independence, report says
-
 Business1 day ago
Business1 day agoTrump on Canada tariff deadline: ‘We can do whatever we want’
-
 Automotive1 day ago
Automotive1 day agoElectric vehicle sales are falling hard in BC, and it is time to recognize reality.
-
 Business1 day ago
Business1 day agoEurope backs off greenwashing rules — Canada should take note
-
 Automotive1 day ago
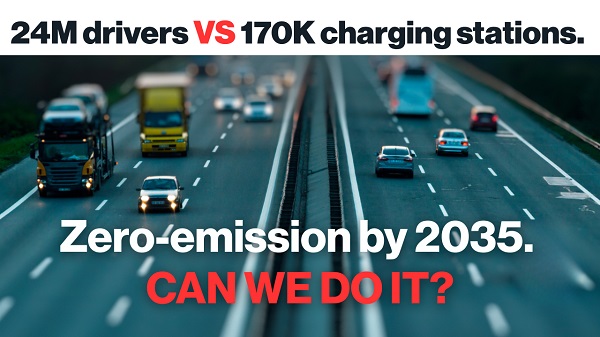
Automotive1 day agoPower Struggle: Electric vehicles and reality
-
 Business10 hours ago
Business10 hours agoCanada Caves: Carney ditches digital services tax after criticism from Trump
-
 Bruce Dowbiggin9 hours ago
Bruce Dowbiggin9 hours agoThe Game That Let Canadians Forgive The Liberals — Again