COVID-19
Free speech victory: Charges against nurse who opposed vaccine mandates defeated

News release from the Justice Centre for Constitutional Freedom
The Justice Centre is pleased to announce that the College of Registered Nurses of Saskatchewan (CRNS) has ruled in favour of nurse Leah McInnes following an October and November 2023 disciplinary hearing. The Investigation Committee of the CRNS had charged Ms. McInnes with spreading “misinformation” because she had voiced her concerns about vaccine mandates. The outcome vindicates her right to professionally advocate for medical ethics and evidence-based health policy.“This is a significant victory for free expression and democratic participation. Nurses, doctors, psychologists, teachers, lawyers, engineers and all Canadians who work in a regulated profession have the freedom to advocate for their beliefs and should not face threats from their own professional association or professional regulator,” stated John Carpay, President of the Justice Centre. Ms. McInnes had been charged by the CRNS’s Investigation Committee, which investigates and prosecutes professional misconduct complaints, for her social media advocacy and for protesting vaccine mandates. The Investigation Committee’s broad allegation against Ms. McInnes was that her advocacy, including her use of the common term “vaccine mandate,” amounted to “misinformation.” Ms. McInnes is a mother of two and has been a Registered Nurse in Saskatchewan since 2013. Ms. McInnes’s advocacy was measured and balanced. She had supported vaccines as an important tool in Covid-management efforts while also pointing to emerging scientific evidence regarding viral loads and transmission, which showed that Covid vaccines did not eliminate transmission. Ms. McInnes opposed vaccine mandates as a violation of basic ethical principles of autonomy and informed and voluntary consent of each and every patient. When Covid vaccines were introduced and voluntarily received in the spring and summer of 2021, the question of vaccine mandates was publicly debated across Canada. On June 30, 2021, the Saskatchewan Government indicated that it would not enforce a vaccine mandate because doing so would pose a “potential violation of health information privacy,” and, later, that it would “infringe on people’s personal rights.” The Saskatchewan Government also stated that a vaccine mandate for provincial employees was not being considered and, on September 10, 2021, rejected a proof-of-vaccination system, stating that mandates create “two classes of citizens based on… vaccination status,” and would be a “divisive path for a government to take.” Similar sentiments were echoed by Alberta’s Jason Kenney and Ontario’s Doug Ford, who claimed it would lead to a “split society.”Around the same time, the Saskatchewan Union of Nurses was calling for the “mandatory immunization” of all healthcare workers–a demand repeated by many, including Saskatchewan NDP leader Ryan Meili and a group of Saskatchewan Health Authority’s Medical Health Officers. Guided by her conscience and professional ethics, notably, her respect for bodily autonomy and informed consent, Ms. McInnes vocally opposed vaccine mandates. She protested vaccine mandates by holding a sign that read, “RN against Mandates and Vax Passports.” According to the Investigation Committee of the College, this sign amounted to “misinformation” with an intention to deceive. Shortly after Ms. McInnes’s advocacy began, the Saskatchewan Government changed course and imposed a vaccine mandate.

A fellow Registered Nurse filed a complaint, calling Ms. McInnes, “Leah aka anti-vaxxer.”The complaint resulted in charges, including the charge that Ms. McInnes knowingly spread misinformation on the basis that, purportedly, no “vaccination mandates” had ever been implemented. It appeared that, according to the Investigation Committee, only a policy of “restrain and vaccinate” qualified as a “vaccine mandate.”After an initial investigation, the Investigation Committee proposed an agreement that would have Ms. McInnes admit to professional misconduct, but she rejected this offer, choosing instead to stand up for her professional and Charter rights. The Investigation Committee charged her on March 28, 2023, and filed a Notice of Hearing, the details of which were later expanded after counsel for Ms. McInnes demanded clarity from the College as to what exactly the College alleged to be “misinformation”, “disinformation” or “misleading” information.Ms. McInnes’s expert witness, former Chief Medical Officer of Health of Ontario Dr. Richard Schabas, confirmed that the term “vaccine mandate” had, in the medical profession, no special meaning beyond its meaning in everyday language. In all contexts, “vaccine mandate” refers to a requirement to either get injected or lose certain rights or freedoms. “Ms. McInnes used the term ‘vaccine mandate’ just as nearly everyone else did in public discourse, including the Toronto Star, the CBC, CTV, the Saskatoon Star Phoenix, CKOM, the Saskatchewan Union of Nurses, academia, Occupational Health and Safety, Saskatchewan Health Authority, the Saskatchewan NDP, and governments,” stated Andre Memauri, co-counsel for Ms. McInnes. “But the Investigation Committee nevertheless forced Ms. McInnes through this painful process, causing her needless grief,” continued Memauri.The Investigation Committee also alleged that Ms. McInnes knowingly spread misinformation about Covid vaccines. Ms. McInnes had posted that vaccines did not provide sterilizing immunity, i.e., that vaccinated people could contract and transmit the virus. During the hearings that took place in 2023, experts, including the Investigation Committee’s own expert, testified that vaccines do not provide sterilizing immunity, vindicating Ms. McInnes. Co-counsel to Ms. McInnes, Glenn Blackett, says, “It’s chilling to recall that this vitally important fact, that the Covid vaccine did not provide sterilizing immunity, was broadly censored while Canadians were supposedly debating the wisdom of vaccine mandates. Poor information makes for poor decisions.”Thankfully for Ms. McInnes and all Canadians who depend on an informed and ethical nursing profession, the Discipline Committee of the College accepted the evidence presented to them and found that Ms. McInnes had, in no way, misinformed the public.Mr. Blackett continued, “This is a hugely important decision, not just for Ms. McInnes, who embodies the ‘moral courage’ Canadians should expect of all health professionals. It is perhaps most important for upholding a nurse’s right to voice ethical and scientific dissent and to participate in democratic discourse. The importance of professional freedom of speech and conscience can hardly be overstated. Science, ethics and democracy simply do not operate without freedom to think and speak. If you can’t trust a professional, be it a nurse, doctor or lawyer, to tell you what they think is true, you can’t trust them at all.”As for Ms. McInnes, she sees this as a victory for free speech in the medical community which will only lead to better outcomes. “I very much value the right of my colleagues to express opinions different than mine and support them in their endeavours to seek change in healthcare and government policy they perceive to be in the public interest. I’m grateful that the CRNS Discipline Committee recognized my right to do the same, as it’s only in the collection of our opinions that the public truly benefits,” she stated. After hearings and submissions in October and November 2023, the College’s Discipline Committee published their decision on January 12, 2024, dismissing all charges against Ms. McInnes. In their decision, the Discipline Committee stated that the case against Ms. McInnes should not have even proceeded to a hearing.
COVID-19
Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

![]()
The Justice Centre for Constitutional Freedoms announces that a judge of the Ontario Court of Justice has ordered the RCMP and TD Bank to produce records relating to the freezing of Mr. Evan Blackman’s bank accounts during the 2022 Freedom Convoy protest.
Mr. Blackman was arrested in downtown Ottawa on February 18, 2022, during the federal government’s unprecedented use of the Emergencies Act. He was charged with mischief and obstruction, but he was acquitted of these charges at trial in October 2023.
However, the Crown appealed Mr. Blackman’s acquittal in 2024, and a new trial is scheduled to begin on August 14, 2025.
Mr. Blackman is seeking the records concerning the freezing of his bank accounts to support an application under the Charter at his upcoming retrial.
His lawyers plan to argue that the freezing of his bank accounts was a serious violation of his rights, and are asking the court to stay the case accordingly.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” says constitutional lawyer Chris Fleury.
“These records will hopefully reveal exactly how and why Mr. Blackman’s accounts were frozen,” he says.
Mr. Blackman agreed, saying, “I’m delighted that we will finally get records that may reveal why my bank accounts were frozen.”
This ruling marks a significant step in what is believed to be the first criminal case in Canada involving a proposed Charter application based on the freezing of personal bank accounts under the Emergencies Act.

Chris Carbert (right) and Anthony Olienick, two of the Coutts Four were jailed for over two years for mischief and unlawful possession of a firearm for a dangerous purpose.
From LifeSiteNews
The “Coutts Four” were painted as dangerous terrorists and their arrest was used as justification for the invocation of the Emergencies Act by the Trudeau government, which allowed it to use draconian measures to end both the Coutts blockade and the much larger Freedom Convoy
COVID protestor Chris Carbert has been granted bail pending his appeal after spending over two years in prison.
On June 30, Alberta Court of Appeal Justice Jo-Anne Strekaf ordered the release of Chris Carbert pending his appeal of charges of mischief and weapons offenses stemming from the Coutts border blockade, which protested COVID mandates in 2022.
“[Carbert] has demonstrated that there is no substantial likelihood that he will commit a criminal offence or interfere with the administration of justice if released from detention pending the hearing of his appeals,” Strekaf ruled.
“If the applicant and the Crown are able to agree upon a release plan and draft order to propose to the court, that is to be submitted by July 14,” she continued.
Carbert’s appeal is expected to be heard in September. So far, Carbert has spent over two years in prison, when he was charged with conspiracy to commit murder during the protest in Coutts, which ran parallel to but was not officially affiliated with the Freedom Convoy taking place in Ottawa.
Later, he was acquitted of the conspiracy to commit murder charge but still found guilty of the lesser charges of unlawful possession of a firearm for a dangerous purpose and mischief over $5,000.
In September 2024, Chris Carbert was sentenced to six and a half years for his role in the protest. However, he is not expected to serve his full sentence, as he was issued four years of credit for time already served. Carbert is also prohibited from owning firearms for life and required to provide a DNA sample.
Carbert was arrested alongside Anthony Olienick, Christopher Lysak and Jerry Morin, with the latter two pleading guilty to lesser charges to avoid trial. At the time, the “Coutts Four” were painted as dangerous terrorists and their arrest was used as justification for the invocation of the Emergencies Act by the Trudeau government, which allowed it to use draconian measures to end both the Coutts blockade and the much larger Freedom Convoy occurring thousands of kilometers away in Ottawa.
Under the Emergency Act (EA), the Liberal government froze the bank accounts of Canadians who donated to the Freedom Convoy. Trudeau revoked the EA on February 23 after the protesters had been cleared out. At the time, seven of Canada’s 10 provinces opposed Trudeau’s use of the EA.
Since then, Federal Court Justice Richard Mosley ruled that Trudeau was “not justified” in invoking the Emergencies Act, a decision that the federal government is appealing.
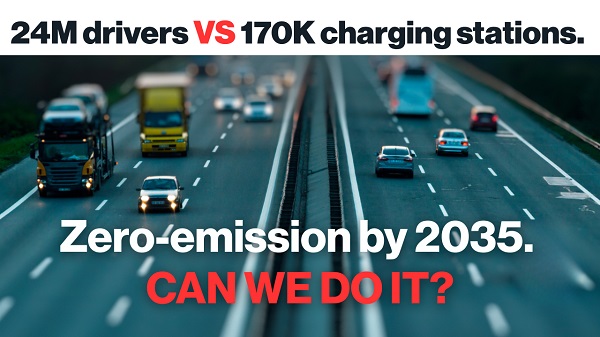
Power Struggle: Electric vehicles and reality

Elon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party

Alberta judge sides with LGBT activists, allows ‘gender transitions’ for kids to continue

China undermining American energy independence, report says
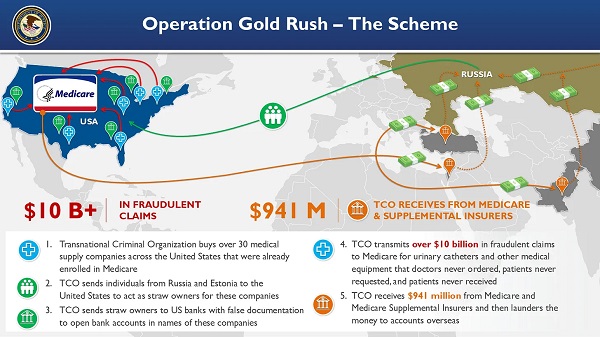
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
Trump on Canada tariff deadline: ‘We can do whatever we want’

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
-
 armed forces1 day ago
armed forces1 day agoCanada’s Military Can’t Be Fixed With Cash Alone
-
Alberta1 day ago
COVID mandates protester in Canada released on bail after over 2 years in jail
-
 International1 day ago
International1 day agoTrump transportation secretary tells governors to remove ‘rainbow crosswalks’
-
 Business1 day ago
Business1 day agoCanada’s loyalty to globalism is bleeding our economy dry
-
 Business1 day ago
Business1 day agoCarney’s spending makes Trudeau look like a cheapskate
-
 Alberta1 day ago
Alberta1 day agoAlberta Next: Alberta Pension Plan
-
 Crime2 days ago
Crime2 days agoProject Sleeping Giant: Inside the Chinese Mercantile Machine Linking Beijing’s Underground Banks and the Sinaloa Cartel
-
 C2C Journal23 hours ago
C2C Journal23 hours agoCanada Desperately Needs a Baby Bump