COVID-19
“Focused Protection” instead of COVID Restrictions. Three prominent epidemiologists calling for a new global response to COVID-19


When it comes to COVID-19, one way or another countries around the world are eventually going to achieve herd immunity. The way most countries are approaching the situation currently will stretch out the amount of time it’s going to take. There are good reasons for that. But now that the virus has been with us for close to a year we’ve learned not everyone is at the same risk of a serious outcome. Some leading epidemiologists think it’s time to take another look at the global response to COVID. As businesses close, millions look for work, seniors long for a hug from a loved one, and young people dream of getting back to their favourite sport, a new approach is being recommended.

The first few days of October, a group of epidemiologists headed by Harvard University’s Dr. Martin Kulldorff, Oxford University’s Dr. Sunetra Gupta, and Stanford University’s Dr. Jay Bhattacharya met to discuss the way governments around the world are reacting to the COVID-19 crisis. As a result of their discussions they posted The Great Barrington Declaration, a call for “Focused Protection”. The declaration outlines a new strategy they hope governments around the world will soon adopt. Coming out of their meeting the three co-signers of the declaration were interviewed by Freddie Sayers of UnHerd. Here’s the fascinating discussion of why these leading thinkers are calling for a different global response to the pandemic.
“This is the saner approach, the more scientific approach,” the authors tell Freddie Sayers
The Great Barrington Declaration
As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical, and mental health impacts of the prevailing COVID-19 policies and recommend an approach we call Focused Protection.
Coming from both the left and right, and around the world, we have devoted our careers to protecting people. Current lockdown policies are producing devastating effects on short and long-term public health. The results (to name a few) include lower childhood vaccination rates, worsening cardiovascular disease outcomes, fewer cancer screenings and deteriorating mental health – leading to greater excess mortality in years to come, with the working class and younger members of society carrying the heaviest burden. Keeping students out of school is a grave injustice.
Keeping these measures in place until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.
Fortunately, our understanding of the virus is growing. We know that vulnerability to death from COVID-19 is more than a thousand-fold higher in the old and infirm than the young. Indeed, for children, COVID-19 is less dangerous than many other harms, including influenza.
As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimize mortality and social harm until we reach herd immunity.
The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk. We call this Focused Protection.
Adopting measures to protect the vulnerable should be the central aim of public health responses to COVID-19. By way of example, nursing homes should use staff with acquired immunity and perform frequent PCR testing of other staff and all visitors. Staff rotation should be minimized. Retired people living at home should have groceries and other essentials delivered to their home. When possible, they should meet family members outside rather than inside. A comprehensive and detailed list of measures, including approaches to multi-generational households, can be implemented, and is well within the scope and capability of public health professionals.
Those who are not vulnerable should immediately be allowed to resume life as normal. Simple hygiene measures, such as hand washing and staying home when sick should be practiced by everyone to reduce the herd immunity threshold. Schools and universities should be open for in-person teaching. Extracurricular activities, such as sports, should be resumed. Young low-risk adults should work normally, rather than from home. Restaurants and other businesses should open. Arts, music, sport and other cultural activities should resume. People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity.
Great Barrington, Massachusetts, 4th October 2020
To sign the declaration, follow this link
www.GBdeclaration.org

From LifeSiteNews
A judge ruled that the Ontario Court of Justice is already ‘satisfied’ with Chris Barber’s sentence and taking away his very livelihood would be ‘disproportionate.’
A Canadian judge has dismissed a demand from Canadian government lawyers to seize Freedom Convoy leader Chris Barber’s “Big Red” semi-truck.
On Friday, Ontario Court of Justice Judge Heather Perkins-McVey denied the Crown’s application seeking to forfeit Barber’s truck.
She ruled that the court is already “satisfied” with Barber’s sentence and taking away his very livelihood would be “disproportionate.”
“This truck is my livelihood,” said Barber in a press release sent to LifeSiteNews.
“Trying to permanently seize it for peacefully protesting was wrong, and I’m relieved the court refused to allow that to happen,” he added.
Criminal defense lawyer Marwa Racha Younes was welcoming of the ruling as well, stating, “We find it was the right decision in the circumstances and are happy with the outcome.”
John Carpay, president of the Justice Centre for Constitutional Freedoms (JCCF), said the decision is “good news for all Canadians who cherish their Charter freedom to assemble peacefully.”
READ: Freedom Convoy protester appeals after judge dismissed challenge to frozen bank accounts
“Asset forfeiture is an extraordinary power, and it must not be used to punish Canadians for participating in peaceful protest,” he added in the press release.
As reported recently by LifeSiteNews, the Canadian government claimed that Barber’s truck is an “offence-related property” relating to his involvement in the 2022 protests against Canada’s COVID mandates.
At this time, the court ruling ends any forfeiture proceedings for the time being, however Barber will continue to try and appeal his criminal conviction and house arrest sentence.
Barber’s truck, a 2004 Kenworth long-haul he uses for business, was a focal point in the 2022 protests. He drove it to Ottawa, where it was parked for an extended period of time, but he complied when officials asked him to move it.
On October 7, 2025, after a long trial, Ontario Court Justice Perkins-McVey sentenced Barber and Tamara Lich, the other Freedom Convoy leader, to 18 months’ house arrest. They had been declared guilty of mischief for their roles as leaders of the 2022 protest against COVID mandates, and as social media influencers.
Lich and Barber have filed appeals of their own against their house arrest sentences, arguing that the trial judge did not correctly apply the law on their mischief charges.
Government lawyers for the Crown have filed an appeal of the acquittals of Lich and Barber on intimidation charges.
The pair’s convictions came after a nearly two-year trial despite the nonviolent nature of the popular movement.

From LifeSiteNews
Protestor Evan Blackman’s legal team argues Trudeau’s Emergencies Act-based bank account freezes were punitive state action tied directly to protest participation.
A Freedom Convoy protester whose bank accounts were frozen by the Canadian government says a judge erred after his ruling did not consider the fact that the funds were frozen under the Emergencies Act, as grounds for a stay of proceedings.
In a press release sent out earlier this week, the Justice Centre for Constitutional Freedoms (JCCF) said that Freedom Convoy protestor Evan Blackman will challenge a court ruling in his criminal case via an appeal with the Ontario Superior Court of Justice.
“This case raises serious questions about how peaceful protest is treated in Canada and about the lasting consequences of the federal government’s unlawful use of the Emergencies Act,” noted constitutional lawyer Chris Fleury. “The freezing of protestors’ bank accounts was part of a coordinated effort to suppress dissent, and courts ought to be willing to scrutinize that conduct.”
Blackman was arrested on February 18, 2022, during the police crackdown on Freedom Convoy protests against COVID restrictions, which was authorized by the Emergencies Act (EA). The EA was put in place by former Prime Minister Justin Trudeau’s Liberal government, which claimed the protests were violent, despite no evidence that this was the case.
Blackman’s three bank accounts with TD Bank were frozen due to his participation in the Freedom Convoy, following a directive ordered by Trudeau.
As reported by LifeSiteNews, in November of this year, Blackman was convicted at his retrial even though he had been acquitted at his original trial. In 2023, Blackman’s “mischief” and “obstructing police” charges were dismissed by a judge due to lack of evidence and the “poor memory of a cop regarding key details of the alleged criminal offences.”
His retrial resulted in Blackman getting a conditional discharge along with 12 months’ probation and 122 hours of community service, along with a $200 victim fine surcharge.
After this, Blackman’s application for a stay of proceedings was dismissed by the court. He had hoped to have his stay of proceedings, under section 24(1) of the Charter of Rights and Freedoms, allowed. However, the judge ruled that the freezing of his bank accounts was legally not related to his arrest, and because of this, the stay of proceedings lacked standing.
The JCCF disagreed with this ruling, noting, it “stands in contrast to a Federal Court decision finding that the government’s invocation of the Emergencies Act was unreasonable and violated Canadians’ Charter rights, including those targeted by the financial measures used against Freedom Convoy protestors.”
As of press time, a hearing date has not been scheduled.
In 2024, Federal Court Justice Richard Mosley ruled that Trudeau was “not justified” in invoking the Emergencies Act.
In early 2022, the Freedom Convoy saw thousands of Canadians from coast to coast come to Ottawa to demand an end to COVID mandates in all forms. Despite the peaceful nature of the protest, Trudeau’s federal government enacted the EA in mid-February.
After the protesters were cleared out, which was achieved through the freezing of bank accounts of those involved without a court order as well as the physical removal and arrest of demonstrators, Trudeau revoked the EA on February 23, 2022.


Ottawa-Alberta agreement may produce oligopoly in the oilsands

Warning Canada: China’s Economic Miracle Was Built on Mass Displacement

‘The electric story is over’

The Top News Stories That Shaped Canadian Energy in 2025 and Will Continue to Shape Canadian Energy in 2026

The Climate Argument Against Livestock Doesn’t Add Up
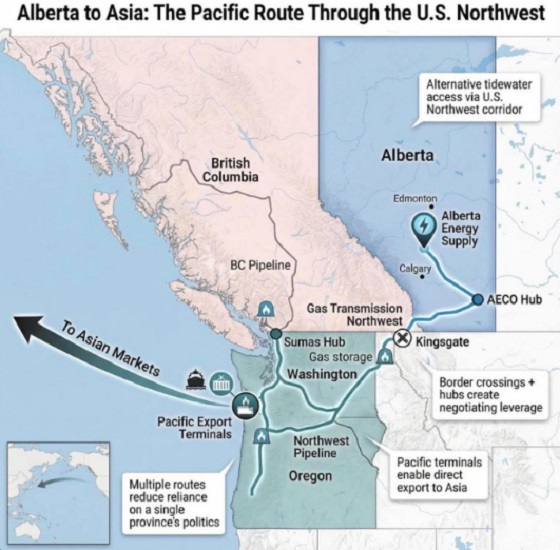
What are the odds of a pipeline through the American Pacific Northwest

Calgary’s new city council votes to ban foreign flags at government buildings
-
 Haultain Research2 days ago
Haultain Research2 days agoSweden Fixed What Canada Won’t Even Name
-
 Business2 days ago
Business2 days agoWhat Do Loyalty Rewards Programs Cost Us?
-
 Business1 day ago
Business1 day agoLand use will be British Columbia’s biggest issue in 2026
-
 International21 hours ago
International21 hours agoChina Stages Massive Live-Fire Encirclement Drill Around Taiwan as Washington and Japan Fortify
-
 Digital ID20 hours ago
Digital ID20 hours agoThe Global Push for Government Mandated Digital IDs And Why You Should Worry
-
 Business18 hours ago
Business18 hours agoFeds pull the plug on small business grants to Minnesota after massive fraud reports
-
 Business7 hours ago
Business7 hours agoDOOR TO DOOR: Feds descend on Minneapolis day cares tied to massive fraud
-
 Bruce Dowbiggin7 hours ago
Bruce Dowbiggin7 hours agoIn Contentious Canada Reality Is Still Six Degrees Of Hockey