COVID-19
Wenstrup Releases Francis Collins’ House Testimony

From the Brownstone Institute
Wenstrup Releases Former NIH Director Francis Collins’ Transcript, Highlights Key Takeaways in New Memo
WASHINGTON — Today, Select Subcommittee on the Coronavirus Pandemic Chairman Brad Wenstrup (R-OH) released the transcript from Dr. Francis Collins’ transcribed interview. Dr. Collins helped lead the government’s Covid-19 pandemic response as the Director of the National Institutes of Health (NIH) until his resignation at the end of 2021. In conjunction with the transcript, the Select Subcommittee also released a new staff memo that highlights the key takeaways from Dr. Collins’ transcribed interview. The memo can be found here.
The full transcript can be found here. Below are important exchanges from Dr. Collins’ transcribed interview:
The hypothesis that the Covid-19 pandemic was the result of a lab leak or lab-related accident is not a conspiracy theory. Despite previously disagreeing with the lab-leak theory — both in public and in private — Dr. Collins testified that the lab-leak hypothesis is indeed not a conspiracy theory.
Majority Counsel: “All it’s calling for is a “yes” or “no.” Is the possibility of a lab leak a conspiracy theory?”
Dr. Collins: “You have to define what you mean by a lab leak.”
Majority Counsel: “Putting aside de novo, the possibility of a laboratory or research-related accident, a researcher doing something in a lab, getting infected with a virus, and then sparking the pandemic. Is that scenario a conspiracy theory”?
Dr. Collins: “Not at this point.”
Majority Counsel: “We have talked about this an awful lot, I think I know the answer to the question, but I want to ask it. Is the origin of Covid-19 still unsettled science?”
Dr. Collins: “Yes.”
The “6-feet apart” social distancing guidance that federal public health officials endorsed was likely not based on any science or data. Dr. Collins agreed with Dr. Fauci that he has not seen any evidence to support the “6-feet apart” directive — which was promoted by public health officials and caused widespread economic and social damage to Americans.
Majority Counsel: “Moving on to social distancing and the various regulations surrounding that. On March 22, 2020, the CDC issued guidance describing social distancing to include remaining out congregant settings, avoiding mass gatherings, and maintaining a distance of approximately six feet from others when possible. We asked Dr. Fauci where the six feet came from and he said it kind of just appeared, is the quote. Do you recall science or evidence that supported the six-feet distance?”
Dr. Collins: “I do not.”
Majority Counsel: “Is that I do not recall or I do not see any evidence supporting six feet?”
Dr. Collins: “I did not see evidence, but I’m not sure I would have been shown evidence at that point.”
Majority Counsel: “Since then, it has been an awfully large topic. Have you seen any evidence since then supporting six feet?”
Dr. Collins: “No.”
NIH often lacks the necessary subject matter expertise to ensure US taxpayer funds are spent safely. Concerningly, Dr. Collins was unaware of any NIH policy that ensures foreign laboratories comply with US standards and are not at odds with U.S. national interests.
Majority Counsel: “Thank you. We’ve asked a number of people regarding the vetting or certifying process of foreign labs that receive U.S. dollars. Do you know what that process is?”
Dr. Collins: “I do not.”
Majority Counsel: “To your knowledge, does NIH certify foreign labs that receive U.S. dollars?”
Dr. Collins: “I don’t know that.”
Majority Counsel: “Again, what we’re trying to figure out is if, like, you get a proposal that has a foreign lab on it, if the NIH would do all the work themselves, or if they would call the State Department, or if they would call some other department to try to determine if that foreign lab is reputable.”
Dr. Collins: “I don’t know.”
The Trump Administration led the charge to rightfully terminate and later suspend EcoHealth Alliance, Inc.’s grant in April 2020. Dr. Collins testified that he supported every enforcement action suggested by the Trump administration and executed by the NIH.
Majority Counsel: “Moving into 2020. Before we start with individual letters, we asked Dr. Lauer and he testified that he would not sign or send a letter that he disagreed with. Do you have any reason to doubt that assertion?”
Dr. Collins: “No.”
Majority Counsel: “Do you agree with every enforcement action the NIH took against EcoHealth?”
Dr. Collins: “Yes.”
Dr. Collins claims that Dr. Fauci invited him to participate in the infamous February 1, 2020 phone call that allegedly “prompted” the public narrative that Covid-19 originated from nature and that vilified the lab-leak hypothesis.
This testimony directly contradicts earlier statements made by Dr. Fauci.
Majority Counsel: “How were you made aware of this call?”
Dr. Collins: “I was, I think – again, it’s four years ago – initially informed by Dr. Fauci that the call was happening. And then, I think I got this email forwarded about what the agenda was going to be from Dr. Farrar, who was clearly the person organizing the call.”
Majority Counsel: “Did Dr. Fauci ask you to join the call?”
Dr. Collins: “Yes.”
There we have it. Ex-director NIH Francis Collins had NO data and has not seen any data to support the social distancing edicts from HHS.
The transcript itself documents that Director Collins had evidence that masking would harm children.
From the transcript:
Q: In the realm of masking, obviously masks became this big to-do during the pandemic. One of the specific aspects that we are interested in is the science and data that supported it for children. So the WHO recommended against masking children less than five because masks are, I’m quoting, not in the overall interest of the child, and against children 6 to 11 from wearing masks because of again, quoting, the potential impact of wearing a mask on learning and psychological development. The United States recommended masking kids as young as two, so directly contradicted the WHO’s recommendation on that.
Do you recall what science or data backed up that recommendation?
Collins: I have no knowledge of that.
Q: Okay. There are now studies coming out regarding learning loss from both school closures and childhood mask wearing — for masks specifically, kids not being able to see adults form words and things like that and it’s causing speech issues. Are you aware of those issues?
Collins: In a general way, yes.
Q: Do you agree that there’s learning loss and other unintended consequences of mask-wearing?
Collins: I have to depend on the experts who assess those things who have evidence, they say, that that’s the case.
This is all the evidence required to conclusively demonstrate that the United States Department of Health and Human Services (HHS) needs a complete overhaul.
Republished from the author’s Substack
Author


From LifeSiteNews
Dr. Theresa Tam received the Order of Canada for her controversial COVID-19 response as the nation’s chief public health officer.
Canada’s former top medical advisor, known for her promotion of masking and COVID vaccines, has received one of Canada’s highest honors.
On June 30, Governor General Mary Simon awarded Dr. Theresa Tam, Canada’s former Chief Public Health Officer (CPHO), the Order of Canada award for her work implementing dangerous COVID regulations, including masking and experimental COVID shots.
“For decades, Theresa Tam has striven to advance global and national public health as a pediatric infectious disease specialist and public servant,” the press release read.
“Her tenure as Canada’s chief public health officer has been characterized by her commitment to health equity and highlighted by her leadership role in the country’s response to the COVID-19 pandemic,” it continued.
The award, given to Canadians who have made extraordinary contributions to the nation, is Canada’s second-highest civilian honor.
Tam’s reception of the award comes just weeks after she stepped down as CPHO, ending her eight-year tenure in the position.
In the early months of 2020, Tam became well-known by Canadians for leading the country’s response to the COVID “pandemic” and pushing arbitrary and dangerous regulations.
Initially, Tam assured Canadians that masking was unnecessary, ineffective, and could even pose health threats.
However, shortly after, Tam changed her policy, telling Canadians that they should even wear masks during sex, a practice which has not been proven to be effective in preventing the spread of COVID and can cause myriad health issues.
Additionally, Tam promoted experimental COVID vaccines for Canadians as young as six months old despite having no long-term studies on its effects and an extensive amount of research proving the dangers of the experimental COVID mRNA jabs that include heart damage and blood clots.
In 2022, after thousands of Canadians reported adverse effects from the vaccine, Tam announced that the federal government was reviewing all federal COVID vaccine mandates, claiming that Canada’s Public Health Agency has never outright endorsed mandatory vaccination.
Tam’s remarks come after more than 1,000 federal workers have been suspended without pay because they chose not to get the COVID jabs or disclose whether they had them per the Privacy Act.
The Order of Canada was also awarded to British Columbia Provincial Health Officer Bonnie Henry, who is known not only for her heavy-handed COVID response, but also for promoting drug use throughout the province.
In 2023, hundreds of British Columbia health care workers sued Henry for ongoing COVID shot mandates preventing them from working. Under Henry, vaccine passports were implemented which required residents to show digital proof of vaccination to enter gyms, restaurants, and other “non-essential” facilities.
Henry also pushed the experimental and dangerous vaccine on children as young as five, despite that fact that clinical trials would not be completed for another two years.
Additionally, in 2024, Henry recommended that British Columbia expand its “safe supply” program to legalize fentanyl and heroin, despite evidence that the program is not working and has worsened the provinces drug crises.


Here’s what the numbers reveal, and what it could mean for humanity
What was once dismissed as a “conspiracy theory” now has hard data behind it.
A new peer-reviewed study out of the Czech Republic has uncovered a disturbing trend: in 2022, women vaccinated against COVID-19 had 33% FEWER successful conceptions per 1,000 women compared to those who were unvaccinated.
A “successful conception” means a pregnancy that led to a live birth nine months later.
The study wasn’t small. It analyzed data from 1.3 million women aged 18 to 39.
Here’s what the numbers reveal, and what it could mean for humanity.
First, let’s talk about the study.
It was published by Manniche and colleagues in the International Journal of Risk & Safety in Medicine, a legitimate, peer-reviewed journal respected for its focus on patient safety and pharmacovigilance.
 |
The study was conducted from January 2021 to December 2023 and examined 1.3 million women aged 18–39. By the end of 2021, approximately 70% of them had received at least one COVID-19 vaccination, with 96% of the vaccinated cohort having received either the Pfizer or Moderna vaccine.
 |
By 2022, a stark difference was clear.
The vaccinated cohort averaged around 4 successful conceptions per 1,000 women per month.
That’s a staggering 33% LESS than the 6 per 1,000 seen in the unvaccinated group.
 |
This means that for every 2 vaccinated women who successfully conceived and delivered a baby, 3 unvaccinated women did the same.
In 2022, unvaccinated women were 1.5 times MORE likely to have a successful conception.
Again, that’s a conception that led to a live birth nine months later.
 |
The authors did not jump to the conclusion that their study proved causation. They cited that other factors may have played a role, such as self-selection bias
However, the researchers noted that self-selection bias does not explain the timing and scale of the observed drop in fertility.
 |
Moreover, birth rates in the Czech Republic dropped from 1.83 per 1,000 women in 2021 to 1.37 in 2024, adding further evidence that the COVID-19 vaccines may be contributing to the decline in fertility.

That downward trend, the researchers argue, supports the hypothesis that something beyond individual decision-making may be affecting conception rates.
As such, they argue that the study’s results warrant a closer and more thorough examination of the impact of mass vaccination.
 |
If this study holds true, and vaccinated women are really much less likely to have successful conceptions, the implications for humanity are massive.
 |
Millions of babies could be missing each year as a result of COVID vaccination, and recent data from Europe and beyond already point to a deeply disturbing trend.
NOTE: Europe experienced a sharper decline in births than usual from 2021 to 2023.
Live births fell from 4.09 million in 2021 to 3.67 million in 2023, marking a 10.3% decline in just two years.

The new Czech study adds to growing evidence that COVID vaccines may be contributing to a dramatic decline in fertility, just as many feared all along.
As Elon Musk warns, “If there are no humans, there’s no humanity.”
Whether the shots are the cause or not, the trend is real—and it’s accelerating.
It’s time to stop dismissing the signals and start investigating the cause.

Thanks for reading. I hope this report gave you real value. This is a critically important topic that deserves attention.
If you appreciate my work and want to help keep it going, consider becoming a paid subscriber.
99% of readers get this content for free. But just $5/month from the 1% keeps it flowing for everyone else.
If this work matters to you, this is the best way to support it.
Be the 1% who makes it possible.
Catch the rest of today’s biggest headlines at VigilantFox.com.

NATO commits to 5% defense floor after Trump pushes allies to step up

It’s not enough to just make military commitments—we must also execute them
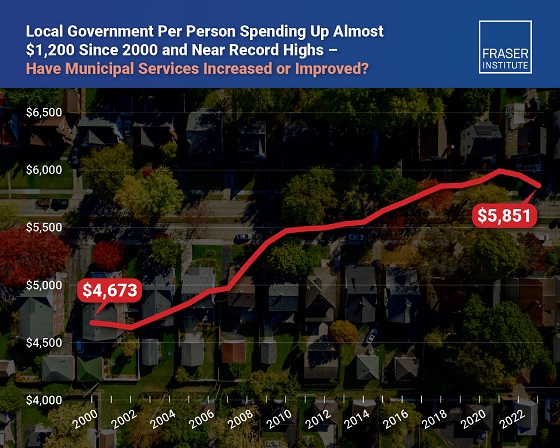
Municipal government per-person spending in Canada hit near record levels

Ottawa Funded the China Ferry Deal—Then Pretended to Oppose It

Red Deer Hospital Lottery 2025 Winners

The Oil Price Spike That Didn’t Happen

Quebec bans gender-confused inmates from requesting prison of their choice
-
 Crime2 days ago
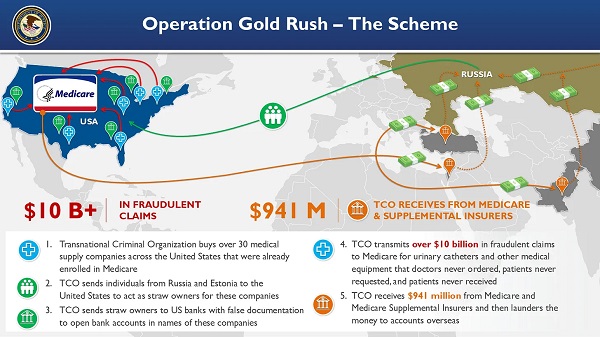
Crime2 days agoNational Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Health2 days ago
Health2 days agoRFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
-
 Business1 day ago
Business1 day agoElon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party
-
 Business12 hours ago
Business12 hours agoWhy it’s time to repeal the oil tanker ban on B.C.’s north coast
-
 Censorship Industrial Complex1 day ago
Censorship Industrial Complex1 day agoGlobal media alliance colluded with foreign nations to crush free speech in America: House report
-
 Business12 hours ago
Business12 hours agoLatest shakedown attempt by Canada Post underscores need for privatization
-
 Energy12 hours ago
Energy12 hours agoIf Canada Wants to be the World’s Energy Partner, We Need to Act Like It
-
 Alberta12 hours ago
Alberta12 hours agoPierre Poilievre – Per Capita, Hardisty, Alberta Is the Most Important Little Town In Canada