Alberta
The Awed Couple: Can Ottawa Force Alberta To Stay In Its Lane?

Fact: Alberta and Saskatchewan were to enter Confederation in 1905 as a province named Buffalo. But Sir Wilfrid Laurier feared a landmass that big would threaten the domination of Quebec and Ontario in Canada. And so Buffalo was split into the two provinces we know today.
Of all the riddles that make up Canada’s current prime minister one of the most intriguing is how the grandson of a man, Charles-Émile Trudeau, who made his fortune in Montreal gas stations is now hellbent on destroying the same industry.
In this obsession to end fossil fuels, Trudeau does have the company of many other heirs to fortunes created by oil and its products. The ranks of Green NGOs and political movements are thick with names like Rockefeller, Getty, Morgan, Flagler and more, heirs with a guilty conscience about perceived climate-change destruction.
But while most of these families have chosen discreet roles in their quest, Trudeau’s climate infatuation has propelled him to prime minister of Canada since 2015. In that time “Sunny Ways” Justin has obsessively pursued his goal of transitioning Canada from the fossil-fuel giant to an imagined Shangri-la of gentle breezes and warm sunshine.
Nothing can shake him of his messianic role as saviour of the Frozen North. Likewise, no public disgrace or controversy can shake his loyal supporters who supported his father in the same manner. Buttressed by the lapdog NDP caucus he spouts buckets of enviro-nonsense to a docile media (which he has bribed to stay quiet).
Because subtlety is not a strong suit he even named a former Greenpeace zealot and convicted felon as his Environment minister. Which has naturally put him directly at odds with that portion of the country that exploits fossil fuels and (don’t tell anybody) floats the boat of federal budgets.
So when Justin proposed a Canadian Sustainable Jobs Act to turn energy workers into code writers and social workers by 2035 there was a degree of pushback amongst those who would lose their livelihoods. That plan was revealed last week by EnerCan (who makes up this dreck?) minister Jonathan Wilkinson.
Promising to convert Calgary’s public transit to all-electric, Wilkinson (former leader of the New Democratic Party‘s youth wing in Saskatchewan) proposed the ‘Sustainable Jobs Act’ advisory council that will provide the federal government with recommendations on how to support the Canadian workforce during transition to a ‘net-zero economy.” You can guess who’ll be on the advisory council, but don’t count on any Ford F-150 drivers.

Enter Danielle Smith, newly re-elected premier of Alberta. Smith and her advisors have declared as unworkable the federal government’s unilateral prescription for a carbon-neutral society by 2050. While they recognize the need for transition the Alberta solution is predictably less draconian than Trudeau’s Pol Pot prescription for moving the population back to a more bucolic lifestyle.
Specifically, Alberta wants “to achieve a carbon-neutral energy economy by 2050, primarily through investment in emissions-reduction technologies and the increased export of Alberta LNG to replace higher-emitting fuels internationally.” (Presumably Alberta will be joined by Saskatchewan in this pushback.)
Then came the hammer. “As the development of Alberta’s natural resources and the regulation of our energy sector workforce are constitutional rights and the responsibility of Alberta, any recommendations provided by this new federal advisory council must align with Alberta’s Emissions Reduction and Energy Development Plan.”
Translation: Federal legislation has to be in synch with provincial plans, not the other way around. In short, try to impose some Michael Mann fantasy on the province and it’s a no-go. Don’t like it? See you in court. In Alberta. Not Ottawa.
Will this constitutional gambit work? While Smith’s mandate from the recent election is hardly rock-solid, she does have the benefit of time in her four-year term. Trudeau has no such luxury, and launching a court case in Alberta would likely stretch past his mandate ending next year. Yes, the impertinence of Alberta would play well with his base in the 514/613/416. But let’s be honest, they are voting Trudeau even if he (in the words of Donald Trump) grabs them by the privates.
One thing you can be assured of when it comes to the PM. He will not be forcing any Canadian Sustainable Jobs Act on the Ontario auto industry to aid its transition to EV vehicles. There will be no helpful suggestions on the death of the automobile for the new mutlti-billion dollar VW battery plants cashing federal cheques in Windsor. He knows his voting base won’t buy it. But those Alberta saps?
The telling impact of this jurisdictional fight will be where Trudeau’s rival, Pierre Poilievre, comes down on the transition issue. With his election depending on the swaths of voters in the GTA shoulder ridings— where Trudeau’s mooting about crybaby Alberta will get a full airing— does he lend his support to Smith’s pushback?

Put simply, is backing Alberta sovereignty in the oil patch a vote-loser for a party still looking past “Hate Trudeau” as an election platform? You could see Poilievre rationalizing that he’ll get the seats in the West no matter what, so why not leave Trudeau to wrassle the Alberta bear alone?
Risky for sure. But if he gets the PMO seat in 2024 Poilievre can always play kiss-and-make-up later with Smith and her government. Can’t wait.
Sign up today for Not The Public Broadcaster newsletters. Hot takes/ cool slants on sports and current affairs. Have the latest columns delivered to your mail box. Tell your friends to join, too. Always provocative, always independent. https://share.hsforms.com/16edbhhC3TTKg6jAaRyP7rActsj5
Bruce Dowbiggin @dowbboy is the editor of Not The Public Broadcaster A two-time winner of the Gemini Award as Canada’s top television sports broadcaster, he’s a regular contributor to Sirius XM Canada Talks Ch. 167. Inexact Science: The Six Most Compelling Draft Years In NHL History, his new book with his son Evan, was voted the seventh-best professional hockey book of all time by bookauthority.org . His 2004 book Money Players was voted sixth best on the same list, and is available via http://brucedowbigginbooks.ca/book-personalaccount.aspx
Alberta
Alberta school boards required to meet new standards for school library materials with regard to sexual content

Alberta’s government has introduced new standards to ensure school library materials are age-appropriate.
School libraries should be safe and supportive places where students can learn and explore without being exposed to inappropriate sexual content. However, in the absence of a consistent standard for selecting age-appropriate library materials, school boards have taken different approaches, leading to concerns about safeguards in place.
In response to these concerns, and informed by feedback from education partners and the public, Alberta’s government has created standards to provide school boards with clear direction on the selection, availability and access to school library materials, such as books.
“Our actions to ensure that materials in school libraries don’t expose children to sexual content were never about banning books. These new standards are to ensure that school boards have clear guidance to ensure age-appropriate access to school library materials, while reflecting the values and priorities of Albertans.”
The new standards set clear expectations for school library materials with regard to sexual content and require school boards to implement policies to support these standards.
Standards for school library materials
Under the new standards, school libraries are not permitted to include library materials containing explicit sexual content. Non-explicit sexual content may be accessible to students in Grade 10 and above, provided it is age-appropriate.
“Protecting kids from explicit content is common sense. LGBTQ youth, like all children, deserve to see themselves in stories that are age-appropriate, supportive and affirming – not in material that sexualizes or confuses them.”
School boards must also regularly review their school library collections, publish a full list of available materials and ensure that a staff member supervises students’ access to school library materials. School boards will have to remove any materials with explicit sexual content from their school libraries by October 1.
School board policies and procedures
All school boards must have publicly available policies that align with the new standards for selecting and managing library materials by January 1, 2026. School boards can either create new policies or update existing ones to meet these requirements.
These policies must outline how school library materials are selected and reviewed, how staff supervise students’ access throughout the school day, and how a student, parent, school board employee or other member of the school community can request a review or removal of materials in the school library. School boards are also required to clearly communicate these policies to employees, students and parents before January 2026.
“A robust, grade- and age-appropriate library catalogue is vital for student success. We welcome the ministry’s initiative to establish consistent standards and appreciate the ongoing consultation to help craft a plan that will serve our families and communities well.”
“Red Deer Public Schools welcomes the new provincial standards for school library materials. Our division is committed to maintaining welcoming, respectful learning spaces where students can grow and thrive. Under the new standards for school libraries, we remain dedicated to providing learning resources that reflect our values and support student success.”
Quick facts
- The new standards will apply to public, separate, francophone, charter and independent schools.
- The ministerial order does not apply to municipal libraries located within schools or materials selected for use by teachers as learning and teaching resources.
- From May 26 to June 6, almost 80,000 people completed an online survey to provide feedback on the creation of consistent standards to ensure the age-appropriateness of materials available to students in school libraries.
Related information
- Ministerial Order
- School library standards engagement
- Reference Materials: Content warning: this document contains graphic content that may be disturbing to viewers and is not appropriate for young viewers. Viewer discretion is advised.

Regional health councils give Albertans a voice
Albertans want a health care system that reflects where they live and adapts to the unique needs of their communities. As part of the province’s health care refocus, Alberta’s government committed to strengthening community voices by providing more opportunities for Albertans to bring forward their local priorities and offer input on how to improve the system.
The regional advisory councils, made up of 150 members from 71 communities, will advise Alberta’s four health ministries and the newly refocused health agencies: Primary Care Alberta, Acute Care Alberta, Assisted Living Alberta and Recovery Alberta. Each council will explore solutions to local challenges and identify opportunities for the health system to better support community decision-making.
“By hearing first-hand community feedback directly, we can build a system that is more responsive, more inclusive and ultimately more effective for everyone. I am looking forward to hearing the councils’ insights, perspectives and solutions to improve health care in all corners of our province.”
“Regional advisory councils will strengthen acute care by giving communities a direct voice. Their insights will help us address local needs, improve patient outcomes and ensure timely access to hospital services.”
“A ‘one-size-fits-all’ approach does not address unique regional needs when it comes to mental health and addiction challenges. These councils will help us hear directly from communities, allowing us to tailor supports and services to meet the needs of Albertans where they are.”
“Every community has unique needs, especially when it comes to seniors and vulnerable populations. These regional advisory councils will help us better understand those needs and ensure that assisted living services are shaped by the people who rely on them.”
Members include Albertans from all walks of life, health care workers, community leaders, Indigenous and municipal representatives, and others with a strong tie to their region. About one-third of members work in health care, and more than half of the council chairs are health professionals. Almost one-quarter are elected municipal officials, including 10 serving as chairs or vice-chairs. Ten councils also include a representative from a local health foundation.
Council members will share local and regional perspectives on health care services, planning and priorities to help ensure decisions reflect the realities of their communities. By engaging with residents, providers and organizations, they will gather feedback, identify challenges and bring forward ideas that may not otherwise reach government.
Through collaboration and community-informed solutions, members will help make the health system more responsive, accessible and better able to meet the needs of Albertans across the province.
“As Primary Care Alberta works to improve access to primary health care services and programs across Alberta, we are grateful to have the opportunity to tap into a dedicated group of community leaders and representatives. These people know their communities and local needs, and we look forward to learning from their experiences and knowledge as we shape the future of primary care in Alberta.”
“The regional advisory councils will help to bring forward the voices of patients, families and front-line providers from every corner of Alberta. Their insights will help us plan smarter and deliver care that’s timely, effective and truly local. We look forward to working closely with them to strengthen hospital and surgical services across the province.”
“Nobody understands the health care challenges unique to a community better than the people who live there. The regional health advisory councils are made up of those living and working on the front lines across the province, ensuring we are getting the perspective of Albertans most affected by our health care system.”
“Alongside Recovery Alberta’s staff and physician team, these regional advisory councils will build upon the high standard of mental health, addiction and correctional health services delivered in Alberta.”
Indigenous Advisory Council
Alberta’s government continues to work directly with Indigenous leaders across the province to establish the Indigenous Advisory Council to strengthen health care services for First Nation, Métis and Inuit communities.
With up to 22 members, including Indigenous health care workers, community leaders and individuals receiving health care services, the council will represent diverse perspectives across Alberta. Members will provide community perspectives about clinical service planning, capital projects, workforce development and cultural integration in health care.
Related information

Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

Canada Desperately Needs a Baby Bump
US airstrike on Iran’s nuclear facilities. Was it obliteration?

Dallas mayor invites NYers to first ‘sanctuary city from socialism’
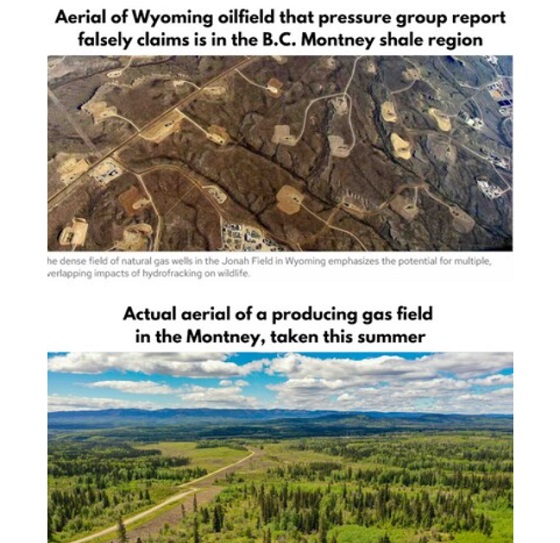
B.C. Residents File Competition Bureau Complaint Against David Suzuki Foundation for Use of False Imagery in Anti-Energy Campaigns

Lacombe meat processor scores $1.2 million dollar provincial tax credit to help expansion

The Left Thinks Drug Criminalization Is Racist. Minorities Disagree
-
 Business2 days ago
Business2 days agoWEF-linked Linda Yaccarino to step down as CEO of X
-
 Freedom Convoy2 days ago
Freedom Convoy2 days agoCourt Orders Bank Freezing Records in Freedom Convoy Case
-
 Crime2 days ago
Crime2 days agoTucker Carlson: US intelligence is shielding Epstein network, not President Trump
-
 Business2 days ago
Business2 days ago‘Experts’ Warned Free Markets Would Ruin Argentina — Looks Like They Were Dead Wrong
-
 Automotive2 days ago
Automotive2 days agoAmerica’s EV Industry Must Now Compete On A Level Playing Field
-
 International2 days ago
International2 days agoSecret Service suspends six agents nearly a year after Trump assassination attempt
-
 Bruce Dowbiggin1 day ago
Bruce Dowbiggin1 day agoThe Covid 19 Disaster: When Do We Get The Apologies?
-
Alberta1 day ago
Fourteen regional advisory councils will shape health care planning and delivery in Alberta