Health
Hundreds of Studies Show DMSO Transforms The Treatment of Cancer

The Forgotten Side of Medicine by A Midwestern Doctor
It might not be something your doctor wants to talk about, but it certainly is something we should all know more about. The video from an old 60 Minutes episode is a must see.
Dimethyl Sulfoxide (DMSO)
Exactly six months ago, I used this newsletter to bring the public’s attention to DMSO, a simple naturally occurring compound that has a number of immense therapeutic benefits and virtually no toxicity (detailed here). In turn, when it was discovered in the 1960s, it quickly became America’s most desired drug (as it cured many incurable ailments). A lot of the scientific community promptly got behind it and before long, thousands of papers had been published on every conceivable medical application for it. Consider for example this 1980 program 60 Minutes aired on DMSO:
As such, throughout this series, I’ve presented the wealth of evidence that DMSO effectively treats:
Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
In turn, when I published this series (because of both how effective and easily accessible DMSO is) it caught on like wildfire, this publication went from being the ninth to top ranked newsletter in the genre, there was a nationwide DMSO shortage, and I’ve received almost two thousand testimonials from people who benefitted from DMSO (and often had remarkable results—particularly for chronic pain).
That response was quite surprising and in my eyes, a testament not only to how well DMSO works, but more importantly, how effectively DMSO’s story was erased from history (e.g., many long-time enthusiasts of natural health shared that they were blown away they’d never heard of it). This sadly illustrates how effectively the medical industry can bury anything threatening its bottom line (e.g., the FDA—for rather petty reasons—used everything at their disposal to make sure DMSO was forgotten).
In turn, within the DMSO story, I believe one of the least appreciated (or even known) facets of it are the remarkable contributions DMSO makes to the treatment of cancer—which is even more remarkable given that far more research has been done with DMSO and cancer than all the other topics I just listed. Consequently, for months I’ve wanted to publish an article on this (particularly since one incredible natural cancer therapy utilizes DMSO), but simultaneously, it just wasn’t feasible to as there was so much literature to go through.
That’s been weighing on me considerably (e.g. many readers have asked me to prioritize this article over everything else), so over the last three months (and particularly the last three weeks), I shifted my responsibilities to focus on the topic thoroughly. While it took a bit of a toll on me, the article is now done. As such, I greatly hope some of what’s in here can benefit you and I likewise thank each of you who has supported this newsletter and made it possible for me to spend so much time delving into these critical forgotten sides of medicine.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber. To see how others have benefitted from this newsletter, click here!
Story at a Glance:
- Dimethyl sulfoxide (DMSO) effectively treats a broad spectrum of conditions, including strokes, pain, tissue injuries, autoimmune inflammation, and cancer.
- DMSO inhibits cancer growth and consistently reverts cancer cells to their normal state.
- DMSO enhances cancer visibility to immune cells, enabling the body to eliminate tumors previously undetected by the immune system.
- DMSO effectively mitigates major challenges in conventional cancer care, such as radiation damage, chemotherapy toxicity, and pain from “incurable” metastatic cancer.
- DMSO markedly boosts the efficacy of many chemotherapy drugs, allowing safer, lower doses to achieve the same results.
- When paired with certain natural therapies, DMSO often produces highly effective cancer treatments, revolutionizing cancer care.
Cancer is one of the most challenging conditions to deal with in medicine, as two seemingly identical cancers can have very different causes. As a result, any standardized (holistic or conventional) protocol will inevitably fail some of the patients it is meant to treat.
Furthermore, since there is so much fear surrounding cancer (e.g., from what the primal fear brings up inside you, from how your social circle reacts to it and from how the medical system uses all of that to push cancer therapies) it is often very difficult to have a clear head about the ordeal or find the right source of advice.
Likewise, since so much money is involved (e.g. 65% of oncologist’s revenues comes from chemotherapy drugs and cancer drugs are by far the most profitable drug market), there is significant pushback (e.g. from medical boards or unhappy relatives) against anyone who attempts alternative cancer therapies making it very difficult to practice unconventional cancer care—particularly since no alternative treatment works all the time.
Note: in a recent article, I highlighted how urologists initially would not touch Lupron (which is now also used as a the puberty blocker) because of how unsafe and ineffective it was, but once they started being paid a lot of money to prescribe it for prostate cancer, it rapidly became their number one drug.
In contrast, while the conventional cancer therapies often have serious issues that make them far worse than any benefit they offer, some conventional cancer therapies are frequently the only available option which can save someone’s life (which has led to me at different times having fights with close friends or relatives either not to do chemotherapy or to get them to start it in cases where I felt it was absolutely necessary).
Given all of this, I presently believe that no “ideal” cancer treatment exists, but if it can be done (e.g., it’s effective for the cancer and feasible to implement), the most ideal to least ideal treatments are as follows:
•Identifying the root cause of a cancer, removing it, and having it quickly and permanently go away on its own (which is sometimes possible).
•Have enough time to rebalance the body so that its terrain no longer supports the cancer and the cancer can fade away on its own (which is often doable but a fairly involved process many have difficulty carrying out).
•Significantly enhance the function of the immune system so that it will eliminate the cancer.
•Find a treatment that is toxic to the cancer but relatively benign to the rest of the body.
•Find a treatment with an acceptable toxicity level and find ways to mitigate its effects.
•Accept a moderately toxic treatment with significant side effects.
•Focus on living with the cancer rather than curing it and then finding ways to mitigate the symptoms you experience both from it and any existing treatment protocols.
•Use a costly conventional therapy that is unlikely to work and live with all the side effects until your life ends (which in more extreme treatment regimens can be quite severe).
If we take a step back, what’s truly remarkable about DMSO, depending on how it is used, is that it can effectively provide most of the benefits listed above with the least amount of collateral damage (e.g., side-effects, toxicity, etc.).

Quick Hit:
President Trump announced Wednesday that Coca-Cola will start using real cane sugar in its U.S. beverages, calling the decision “a very good move.” In a Truth Social post, Trump said he had spoken directly with the company and thanked its leadership for the change.
Key Details:
- Trump wrote, “I have been speaking to Coca-Cola about using REAL Cane Sugar in Coke in the United States, and they have agreed to do so.”
- He praised the company’s leadership, saying, “This will be a very good move by them — You’ll see. It’s just better!”
- U.S. Coca-Cola currently uses high fructose corn syrup, unlike versions in Mexico and the UK that use cane sugar.
Diving Deeper:
President Donald Trump on Wednesday said that Coca-Cola is set to bring real cane sugar back into its U.S. soft drinks — a switch many longtime Coke fans have long desired. Posting on Truth Social, Trump wrote: “I have been speaking to Coca-Cola about using REAL Cane Sugar in Coke in the United States, and they have agreed to do so.”
The president continued, “I’d like to thank all of those in authority at Coca-Cola. This will be a very good move by them — You’ll see. It’s just better!”
Coca-Cola has used high fructose corn syrup in the United States since the 1980s, largely due to domestic corn subsidies and the higher cost of imported sugar. However, the cane sugar version — still available in Mexico and much of Europe — remains popular among American consumers, with many saying it offers a cleaner, smoother flavor.
Trump’s comments immediately drew attention both for the policy implication and the personal touch. Though the president is known for his affinity for Diet Coke, which contains no sugar at all, his interest in restoring cane sugar to the classic formula taps into a broader nostalgia many Americans have for pre-1980s Coke.
No formal announcement has yet been made by Coca-Cola itself, and it remains unclear if the reported agreement pertains to all Coke products or specific regional lines. But Trump’s declaration is already generating buzz among fans of the brand and supporters.
(AP Photo/Lynne Sladky)

By Alexandra Keeler
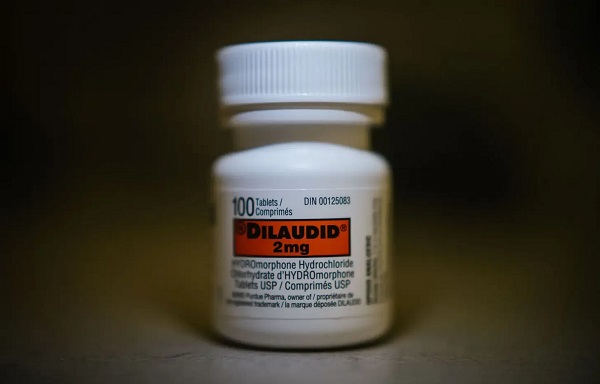
Canada has spent more than $100 million on safer supply programs, but has failed to research their long-term effects
Canada lacks long-term data on safer supply programs, despite funding these programs for years.
Safer supply programs dispense pharmaceutical opioids as a replacement for toxic street drugs.
There is a growing body of research on safer supply’s short-term health effects. But there are no Canadian studies that evaluate program participants’ health impacts beyond 18 months.
The absence of research into long-term data on safer supply means policymakers do not understand how safer supply affects participants’ health, substance use or social outcomes over time.
“Long-term data is important because it helps us understand not just short-term health outcomes like reduced overdoses, but also broader impacts on quality of life, stability and health care use,” said Farihah Ali, scientific lead at the Institute for Mental Health Policy Research at CAMH. The Centre for Addiction and Mental Health is one of Canada’s leading centres for addiction research and clinical care.
Pilot projects
Canada’s first safer supply programs were introduced in Ontario in 2016. Those programs were initially small in scope, intended for a small group of high-risk individuals.
In 2020, the federal government began funding safer supply pilot programs across the country. Provinces are responsible for the delivery and regulation of these programs.
B.C. introduced provincewide programs in 2021. Other provinces, such as Alberta, have restricted safer supply access to a very small number of clinics, and have generally shifted away from harm reduction models in favour of recovery-oriented approaches.
According to the Canadian Public Health Association, an advocacy organization, the original goal for safer supply was to reduce deaths and harms associated with the unregulated toxic drug supply. It was not meant to replace addiction treatment, but to rather act as a bridge to further care.
However, a 2023 report by researchers at McMaster University and Simon Fraser University noted safer supply “does not principally operate toward goals of treatment or recovery.” The report describes safer supply instead as an emergency intervention focused on stabilization and survival.
Evidence gaps
There is a small but growing body of short-term studies on the health effects of Canada’s safer supply programs. Most only track participants’ outcomes for up to 12 months.
Some of those studies suggest safer supply may reduce the immediate harms associated with drug use.
A 2024 study found a 91 per cent reduction in the risk of death among high-risk individuals receiving safer supply in B.C. Critics have raised concerns about the study’s methodology, sample size and confounding variables.
In contrast, a March study suggested B.C.’s safer supply and decriminalization policies may be associated with increased hospitalizations. These findings also sparked controversy, with experts debating how well the data isolate causal impacts.
And a comparative study released in April also showed some positive outcomes from safer supply. It too sparked significant expert debate.
‘Arms-length’
Of all the provinces, B.C. has implemented safer supply most broadly. The province’s health ministry did not directly respond when asked about the long-term goals of its safer supply program, or whether B.C. collects longitudinal data on program participants’ health outcomes.
“Evidence shows [safer supply] helps separate people from the unregulated drug supply, manage their substance use and withdrawal symptoms with regulated medications, and helps connect them to voluntary health and social supports,” a Ministry of Health spokesperson told Canadian Affairs in an email.
The ministry did not provide the evidence it referenced.
At the federal level, Health Canada confirmed that, to date, it has funded just two evaluations of safer supply programs, despite spending more than $100 million on safer supply since April 2023.
The first was a short-term study, funded by the federal government’s Substance Use and Addictions Program program. Conducted over four months, that study assessed 10 safer supply programs in Ontario, B.C., and New Brunswick. It documented initial impacts on participants’ lives and program delivery, primarily through qualitative methods such as interviews and surveys.
The second study is an ongoing, “arms-length evaluation” of 11 safer supply pilot programs funded by the Canadian Institutes of Health Research (CIHR), Canada’s federal health research agency.
When asked about long-term research on safer supply, Health Canada referred Canadian Affairs to a 2022 funding announcement about this multi-year evaluation. While the evaluation is being conducted over several years, it is unclear if it includes long-term tracking of patients’ outcomes.
Barriers and resistance
There are a number of factors that make it challenging to evaluate safer supply programs over long periods.
Ali, of CAMH, says unstable, short-term funding can disrupt long-term research.
“When programs are shut down or scaled back, we lose contact with participants and the ability to track outcomes over time,” she said.
Program participants can also be difficult to track over long periods, she says. Many struggle with housing insecurity, health instability and criminalization.
Frontline staff also face burnout and high turnover, she says, limiting support for such research activities.
Additionally, there are tradeoffs between the anonymity needed to encourage patients to access safer supply programs and the ability to collect detailed data.
“Ethical concerns — like not wanting to burden participants or risk their safety or confidentiality — require us to design studies that are trauma-informed and flexible, which adds complexity to long-term data collection,” Ali said.
Julian Somers, a clinical psychologist and professor at Simon Fraser University, says B.C.’s failure to conduct long-term evaluations of its safer supply programs is not just an oversight, but an act of negligence.
“B.C. has some of the best pharmaceutical data systems in the world,” Somers said, referring to PharmaCare and PharmaNet — databases that capture every prescription drug transaction in the province.
Somers says his team previously used PharmaNet data to examine prescribed opioids’ effects on health and social outcomes. In 2017, he proposed a long-term safer supply evaluation using these tools.
In 2017, he proposed a long-term evaluation of B.C.’s safer supply programs.
The province declined.
According to Ali, “Future research should explore how safer supply impacts people’s long-term health, stability and connection to care.”
“We also need to listen to people’s experiences, how safer supply affects their daily lives, their sense of dignity, and their relationships with care providers through qualitative mechanisms.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
‘We’re Going To Lose’: Steve Bannon Warns Withholding Epstein Files Would Doom GOP

Median workers in Alberta could receive 72% more under Alberta Pension Plan compared to Canada Pension Plan

CNN’s Shock Climate Polling Data Reinforces Trump’s Energy Agenda

CBC six-figure salaries soar

Trump slaps Brazil with tariffs over social media censorship

Net Zero: The Mystery of the Falling Fertility

FBI’s Dan Bongino may resign after dispute about Epstein files with Pam Bondi
-
 Energy2 days ago
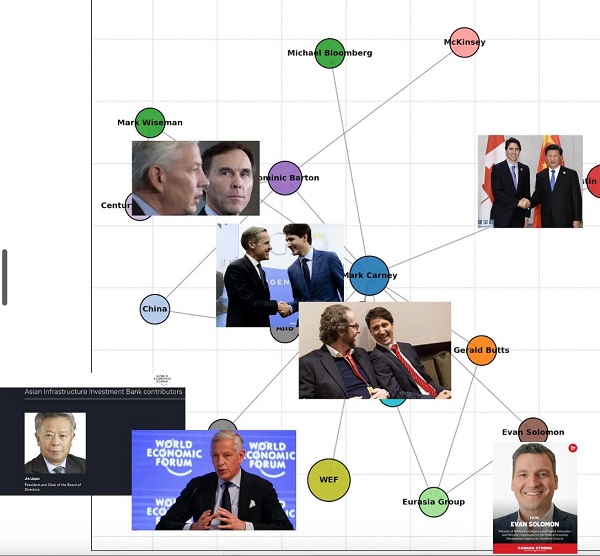
Energy2 days agoIs The Carney Government Making Canadian Energy More “Investible”?
-
 Business2 days ago
Business2 days agoDemocracy Watchdog Says PM Carney’s “Ethics Screen” Actually “Hides His Participation” In Conflicted Investments
-
 Business2 days ago
Business2 days agoCompetition Bureau is right—Canada should open up competition in the air
-
 Immigration2 days ago
Immigration2 days agoUnregulated medical procedures? Price Edward Islanders Want Answers After Finding Biomedical Waste From PRC-Linked Monasteries
-
 Business2 days ago
Business2 days agoIt’s Time To End Canada’s Protectionist Supply Management Regime
-
 COVID-192 days ago
COVID-192 days agoFreedom Convoy leaders’ sentencing hearing to begin July 23 with verdict due in August
-
Addictions2 days ago
After eight years, Canada still lacks long-term data on safer supply
-
 National1 day ago
National1 day agoLiberals push to lower voting age to 16 in federal elections