Uncategorized
Horror difficult to erase for Indonesians as toll tops 1,400

PALU, Indonesia — For some who survived the massive earthquake and tsunami on Indonesia’s Sulawesi island last week, the memories and the horror of experiencing a disaster that has left more than 1,400 people dead are both hard to erase and understand.
Furniture maker Khairul Hassan recalled working at a shop near the beach in front of a row of warehouses when the ground came alive and shook violently. He ran to a nearby hill and watched as the ocean heaved up and hurled forward. Now he can’t forget.
“I saw the waves come and sweep out everything — buildings, factories, warehouses and some people who were lost, racing from the waves, some of them women and children,” he said Wednesday. “Also, warehouse workers who were trapped under goods, all swept by the sea. It’s so tragic. It’s so scary to remember.”
Five days later, aid was slowly creeping into areas where victims have become increasingly desperate after being left without food, water, fuel and medicine. In one
“I’m so happy,” said Heruwanto, 63, who goes by one name. He was clutching a box of instant noodles. “I really haven’t eaten for three days.”
The official death toll increased to 1,407 on Wednesday, with thousands injured and more than 70,000 displaced from their homes, said national disaster agency spokesman Sutopo Purwo Nugroho. He said the number of dead would increase, but that rescue crews had reached all affected areas.
The U.N. humanitarian office estimated that some 200,000 people need assistance in the disaster zone and announced a $15 million allocation to bolster relief efforts. Help has been slow to reach many victims, especially those living in areas cut off by impassable roads. But large fuel and food conveys, guarded by security forces, have been making their way in.
Miles (
All that remained of many beachside homes was their foundations. Wrecked houses still standing were spray painted with appeals for aid. On the wall of one dwelling, “Help us Mr. President” was scrawled in big lettering.
The town of Donggala to the northwest of Palu was relatively unscathed. A few houses had collapsed and a couple of large boats were beached. Residents were relaxed and smiling in contrast to the anguish and tension evident across Palu.
In addition to the quake and tsunami, Indonesia also demonstrated Wednesday what it means to sit on the Pacific “Ring of Fire” when a volcano erupted in another part of Sulawesi island about 940
Experts said it’s possible the quake accelerated the eruption, but there is no concrete evidence to prove that. Activity at the volcano had been increasing since August and began surging on Monday, Kasbani, who heads Indonesia’s Volcanology and Geology Disaster Mitigation Agency and uses one name, told an online news portal.
More than 25 countries offered assistance after President Joko “Jokowi” Widodo appealed for international help. He visited the disaster zone Wednesday, saying there’s still work to be done, but that conditions were improving with businesses starting to reopen, helping people to start returning their lives to normal.He said U.S. President Donald Trump called him Tuesday night, offering assistance.
“We are going in phases. There are lots of things happening related to evacuation, as aid and fuel are also coming in,” he said, noting that 30 people remain buried under rubble at the Roa Roa Hotel in Palu.
Some homeless residents weren’t waiting for help. Dozens sifted through what remained of the flattened complex of warehouses along Palu’s ravaged coastline, looking for anything they could salvage to eat, sell or help them rebuild. They carted away corrugated metal, wood, piping and other items.
Others pulled out small cartons of milk, soft drinks, rice, sweets and painkillers. They were young and old, middle class and poor, university students and sullen young men.
“We have to do this because there’s no assistance from the government,” said Zaitun Rajamangili, 41, adding that his home was swept away but his family survived.
Following widespread looting and aid vehicles being stopped and surrounded by people on roads, Indonesian military chief Hadi Tjahyanto said one soldier and one police officer would be placed on every aid truck and soldiers would be sent to secure markets, the airport and fuel depots to maintain order. He added that a Singaporean military transport plane will help evacuate victims from the airport in Palu. In addition, aircraft from South Korea, the United Kingdom and Japan were expected to ferry aid.
Australia announced it will send 50 medical professionals as part of a $3.6 million aid package.
The U.N. said the Indonesian Ministry of Social Affairs has asked the U.N. children’s agency, UNICEF, to send social workers to support vulnerable children who are alone or became separated from their families. It said the World Health Organization is warning that a lack of shelter and damaged water sanitation facilities could lead to outbreaks of communicable diseases.
Indonesia, a vast archipelago of 260 million people, is frequently struck by earthquakes, volcanic eruptions and tsunamis because of its location on the “Ring of Fire,” an arc of volcanoes and fault lines in the Pacific Basin. A powerful quake on the island of Lombok killed 505 people in August.
___
Associated Press writers Niniek Karmini in Palu, Indonesia; Margie Mason and Eileen Ng in Jakarta, Indonesia; Rod McGuirk in Canberra, Australia; and Edith M. Lederer at the United Nations contributed to this report.
Stephen Wright, The Associated Press

![]()
Energy security, resilience and affordability have long been protected by a continentally integrated energy sector.
The G7 summit in Kananaskis, Alberta, offers a key platform to reassert how North American energy cooperation has made the U.S. and Canada stronger, according to a joint statement from The Heritage Foundation, the foremost American conservative think tank, and MEI, a pan-Canadian research and educational policy organization.
“Energy cooperation between Canada, Mexico and the United States is vital for the Western World’s energy security,” says Diana Furchtgott-Roth, director of the Center for Energy, Climate and Environment and the Herbert and Joyce Morgan Fellow at the Heritage Foundation, and one of America’s most prominent energy experts. “Both President Trump and Prime Minister Carney share energy as a key priority for their respective administrations.
She added, “The G7 should embrace energy abundance by cooperating and committing to a rapid expansion of energy infrastructure. Members should commit to streamlined permitting, including a one-stop shop permitting and environmental review process, to unleash the capital investment necessary to make energy abundance a reality.”
North America’s energy industry is continentally integrated, benefitting from a blend of U.S. light crude oil and Mexican and Canadian heavy crude oil that keeps the continent’s refineries running smoothly.
Each day, Canada exports 2.8 million barrels of oil to the United States.
These get refined into gasoline, diesel and other higher value-added products that furnish the U.S. market with reliable and affordable energy, as well as exported to other countries, including some 780,000 barrels per day of finished products that get exported to Canada and 1.08 million barrels per day to Mexico.
A similar situation occurs with natural gas, where Canada ships 8.7 billion cubic feet of natural gas per day to the United States through a continental network of pipelines.
This gets consumed by U.S. households, as well as transformed into liquefied natural gas products, of which the United States exports 11.5 billion cubic feet per day, mostly from ports in Louisiana, Texas and Maryland.
“The abundance and complementarity of Canada and the United States’ energy resources have made both nations more prosperous and more secure in their supply,” says Daniel Dufort, president and CEO of the MEI. “Both countries stand to reduce dependence on Chinese and Russian energy by expanding their pipeline networks – the United States to the East and Canada to the West – to supply their European and Asian allies in an increasingly turbulent world.”
Under this scenario, Europe would buy more high-value light oil from the U.S., whose domestic needs would be back-stopped by lower-priced heavy oil imports from Canada, whereas Asia would consume more LNG from Canada, diminishing China and Russia’s economic and strategic leverage over it.
* * *
The MEI is an independent public policy think tank with offices in Montreal, Ottawa, and Calgary. Through its publications, media appearances, and advisory services to policymakers, the MEI stimulates public policy debate and reforms based on sound economics and entrepreneurship.
As the nation’s largest, most broadly supported conservative research and educational institution, The Heritage Foundation has been leading the American conservative movement since our founding in 1973. The Heritage Foundation reaches more than 10 million members, advocates, and concerned Americans every day with information on critical issues facing America.
Uncategorized
Poilievre on 2025 Election Interference – Carney sill hasn’t fired Liberal MP in Chinese election interference scandal
From Conservative Party Communications
“Yes. He must be disqualified. I find it incredible that Mark Carney would allow someone to run for his party that called for a Canadian citizen to be handed over to a foreign government on a bounty, a foreign government that would almost certainly execute that Canadian citizen.
“Think about that for a second. We have a Liberal MP saying that a Canadian citizen should be handed over to a foreign dictatorship to get a bounty so that that citizen could be murdered. And Mark Carney says he should stay on as a candidate. What does that say about whether Mark Carney would protect Canadians?
“Mark Carney is deeply conflicted. Just in November, he went to Beijing and secured a quarter-billion-dollar loan for his company from a state-owned Chinese bank. He’s deeply compromised, and he will never stand up for Canada against any foreign regime. It is another reason why Mr. Carney must show us all his assets, all the money he owes, all the money that his companies owe to foreign hostile regimes. And this story might not be entirely the story of the bounty, and a Liberal MP calling for a Canadian to be handed over for execution to a foreign government might not be something that the everyday Canadian can relate to because it’s so outrageous. But I ask you this, if Mark Carney would allow his Liberal MP to make a comment like this, when would he ever protect Canada or Canadians against foreign hostility?
“He has never put Canada first, and that’s why we cannot have a fourth Liberal term. After the Lost Liberal Decade, our country is a playground for foreign interference. Our economy is weaker than ever before. Our people more divided. We need a change to put Canada first with a new government that will stand up for the security and economy of our citizens and take back control of our destiny. Let’s bring it home.”

It’s not enough to just make military commitments—we must also execute them

Alberta Next Takes A Look At Alberta Provincial Police Force

The permanent CO2 storage site at the end of the Alberta Carbon Trunk Line is just getting started

President Xi Skips Key Summit, Adding Fuel to Ebbing Power Theories

Federal government should finally cut Trudeau-era red tape

Canadian Oil Sands Production Expected to Reach All-time Highs this Year Despite Lower Oil Prices

Ontario man launches new challenge against province’s latest attempt to ban free expression on roadside billboards
-
 Alberta1 day ago
Alberta1 day agoAlberta judge sides with LGBT activists, allows ‘gender transitions’ for kids to continue
-
 Crime20 hours ago
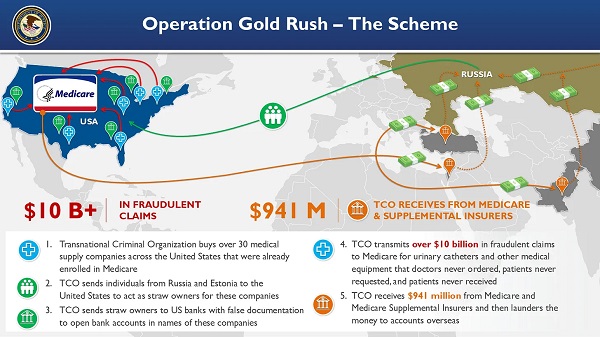
Crime20 hours agoNational Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Business8 hours ago
Business8 hours agoElon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party
-
 Business2 days ago
Business2 days agoCanada Caves: Carney ditches digital services tax after criticism from Trump
-
 Business2 days ago
Business2 days agoMassive government child-care plan wreaking havoc across Ontario
-
 Alberta1 day ago
Alberta1 day agoAlberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued
-
 Health19 hours ago
Health19 hours agoRFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
-
 Censorship Industrial Complex8 hours ago
Censorship Industrial Complex8 hours agoGlobal media alliance colluded with foreign nations to crush free speech in America: House report