COVID-19
Health researcher calls government promotion of Covid mRNA vaccines “confusing”
From (2079) Dr. John Campbell – YouTube
British Health researcher John Campbell has uncovered sobering and disturbing statistics regarding serious adverse events connected to covid vaccines.
As Campbell outlines in this presentation, multiple previous vaccines producing far fewer adverse events, have been withdrawn from public use while governments continue to promote covid vaccines.
(Campbell is well known for his meticulous research and he always includes links to the studies he is calling attention to. His presentation notes are below the video)
John Campbell’s research notes and links to relevant studies
Swine flu vaccine (1976), 1 serious event per 100,000 vaccinees,
Vaccine withdrawn Rotavirus vaccine
Rotashield, (1999),1 to 2 serious events per 10,000 vaccinees,
Vaccine withdrawn
Covid mRNA vaccines, 1 serious event per 800 vaccinees,
Vaccine officially promoted
Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults https://pubmed.ncbi.nlm.nih.gov/36055…
Free full text available https://www.ncbi.nlm.nih.gov/pmc/arti…
Why We Question the Safety Profile of mRNA COVID-19 Vaccines (Robert M Kaplan and Sander Greenland) https://sensiblemed.substack.com/p/wh…
Using publicly available data from Pfizer and Moderna studies, we found one serious adverse event for each 800 vaccinees. That translates to about 1,250 serious events for each million vaccine recipients.
US, Spain, Australia
Study to evaluate serious adverse events of special interest observed in mRNA COVID-19 vaccine trials.
Secondary analysis of serious adverse events reported in the placebo-controlled, phase III randomized clinical trials, of Pfizer and Moderna mRNA COVID-19 vaccines
Results Pfizer and Moderna mRNA COVID-19 vaccines were associated with an excess risk of serious adverse events
of special interest
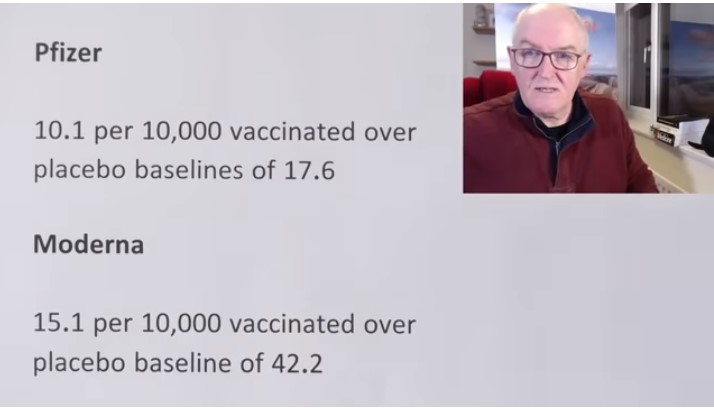
Pfizer
10.1 per 10,000 vaccinated over placebo baselines of 17.6
Moderna
15.1 per 10,000 vaccinated over placebo baseline of 42.2
Combined, the mRNA vaccines Associated with an excess risk of serious adverse events of special interest of 12.5 per 10,000 vaccinated
Pfizer trial
Pfizer vaccine group 52 serious AESI (27.7 per 10,000) were reported
Pfizer placebo group 33 serious AESI (17.6 per 10,000) were reported
36 % higher risk of serious adverse events in the vaccine group
Risk difference 18.0 per 10,000 vaccinated
Moderna trial
Moderna trial, vaccine group 87 serious AESI (57.3 per 10,000) were reported
Moderna trial, placebo group 64 serious AESI (42.2 per 10,000) were reported
6 % higher risk of serious adverse events in the vaccine group
Risk difference 7.1 per 10,000 vaccinated
Discussion
The excess risk of serious adverse events found in our study points to the need for formal harm-benefit analyses, particularly those that are stratified according to risk of serious COVID-19 outcomes. These analyses will require public release of participant level datasets. Full transparency of the COVID-19 vaccine clinical trial data is needed, to properly evaluate these questions.
Unfortunately, as we approach 2 years after release of COVID-19 vaccines, participant level data remain inaccessible.
Level of adverse reactions in the past
The 1976 swine flu vaccine
Small increased risk of Guillain-Barré Syndrome
The increased risk was approximately 1 additional case of GBS for every 100,000 people who got the swine flu vaccine. When over 40 million people were vaccinated against swine flu, federal health officials decided that the possibility of an association of GBS with the vaccine, however small, necessitated stopping immunization until the issue could be explored.
The Institute of Medicine (2003) https://www.ncbi.nlm.nih.gov/books/NB…
Concluded that people who received the 1976 swine influenza vaccine had an increased risk for developing GBS. Exact reason for this association remains unknown.
Rotavirus vaccine Rotashield, (1999) https://www.cdc.gov/vaccines/vpd-vac/…
The U.S. Advisory Committee on Immunization Practices (ACIP) October 22, 1999 to no longer recommend use of the RotaShield® vaccine for infants, because of an association between the vaccine and intussusception. The results of the investigations showed that RotaShield® vaccine caused intussusception in some healthy infants Within 2 weeks Intussusception increased 20 to 30 times over the expected risk (Less after the second and third dose) CDC estimated that one or two additional cases of intussusception would be caused among each 10,000 infants vaccinated with RotaShield® vaccine.
COVID-19
Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

![]()
The Justice Centre for Constitutional Freedoms announces that a judge of the Ontario Court of Justice has ordered the RCMP and TD Bank to produce records relating to the freezing of Mr. Evan Blackman’s bank accounts during the 2022 Freedom Convoy protest.
Mr. Blackman was arrested in downtown Ottawa on February 18, 2022, during the federal government’s unprecedented use of the Emergencies Act. He was charged with mischief and obstruction, but he was acquitted of these charges at trial in October 2023.
However, the Crown appealed Mr. Blackman’s acquittal in 2024, and a new trial is scheduled to begin on August 14, 2025.
Mr. Blackman is seeking the records concerning the freezing of his bank accounts to support an application under the Charter at his upcoming retrial.
His lawyers plan to argue that the freezing of his bank accounts was a serious violation of his rights, and are asking the court to stay the case accordingly.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” says constitutional lawyer Chris Fleury.
“These records will hopefully reveal exactly how and why Mr. Blackman’s accounts were frozen,” he says.
Mr. Blackman agreed, saying, “I’m delighted that we will finally get records that may reveal why my bank accounts were frozen.”
This ruling marks a significant step in what is believed to be the first criminal case in Canada involving a proposed Charter application based on the freezing of personal bank accounts under the Emergencies Act.

Chris Carbert (right) and Anthony Olienick, two of the Coutts Four were jailed for over two years for mischief and unlawful possession of a firearm for a dangerous purpose.
From LifeSiteNews
The “Coutts Four” were painted as dangerous terrorists and their arrest was used as justification for the invocation of the Emergencies Act by the Trudeau government, which allowed it to use draconian measures to end both the Coutts blockade and the much larger Freedom Convoy
COVID protestor Chris Carbert has been granted bail pending his appeal after spending over two years in prison.
On June 30, Alberta Court of Appeal Justice Jo-Anne Strekaf ordered the release of Chris Carbert pending his appeal of charges of mischief and weapons offenses stemming from the Coutts border blockade, which protested COVID mandates in 2022.
“[Carbert] has demonstrated that there is no substantial likelihood that he will commit a criminal offence or interfere with the administration of justice if released from detention pending the hearing of his appeals,” Strekaf ruled.
“If the applicant and the Crown are able to agree upon a release plan and draft order to propose to the court, that is to be submitted by July 14,” she continued.
Carbert’s appeal is expected to be heard in September. So far, Carbert has spent over two years in prison, when he was charged with conspiracy to commit murder during the protest in Coutts, which ran parallel to but was not officially affiliated with the Freedom Convoy taking place in Ottawa.
Later, he was acquitted of the conspiracy to commit murder charge but still found guilty of the lesser charges of unlawful possession of a firearm for a dangerous purpose and mischief over $5,000.
In September 2024, Chris Carbert was sentenced to six and a half years for his role in the protest. However, he is not expected to serve his full sentence, as he was issued four years of credit for time already served. Carbert is also prohibited from owning firearms for life and required to provide a DNA sample.
Carbert was arrested alongside Anthony Olienick, Christopher Lysak and Jerry Morin, with the latter two pleading guilty to lesser charges to avoid trial. At the time, the “Coutts Four” were painted as dangerous terrorists and their arrest was used as justification for the invocation of the Emergencies Act by the Trudeau government, which allowed it to use draconian measures to end both the Coutts blockade and the much larger Freedom Convoy occurring thousands of kilometers away in Ottawa.
Under the Emergency Act (EA), the Liberal government froze the bank accounts of Canadians who donated to the Freedom Convoy. Trudeau revoked the EA on February 23 after the protesters had been cleared out. At the time, seven of Canada’s 10 provinces opposed Trudeau’s use of the EA.
Since then, Federal Court Justice Richard Mosley ruled that Trudeau was “not justified” in invoking the Emergencies Act, a decision that the federal government is appealing.
Power Struggle: Electric vehicles and reality

Elon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump

Electric vehicle sales are falling hard in BC, and it is time to recognize reality.

Canada Caves: Carney ditches digital services tax after criticism from Trump

Alberta judge sides with LGBT activists, allows ‘gender transitions’ for kids to continue

China undermining American energy independence, report says
-
 armed forces1 day ago
armed forces1 day agoCanada’s Military Can’t Be Fixed With Cash Alone
-
Alberta1 day ago
COVID mandates protester in Canada released on bail after over 2 years in jail
-
 International1 day ago
International1 day agoTrump transportation secretary tells governors to remove ‘rainbow crosswalks’
-
 Business1 day ago
Business1 day agoCarney’s spending makes Trudeau look like a cheapskate
-
 Business1 day ago
Business1 day agoCanada’s loyalty to globalism is bleeding our economy dry
-
 Alberta1 day ago
Alberta1 day agoAlberta Next: Alberta Pension Plan
-
 Crime2 days ago
Crime2 days agoProject Sleeping Giant: Inside the Chinese Mercantile Machine Linking Beijing’s Underground Banks and the Sinaloa Cartel
-
 C2C Journal24 hours ago
C2C Journal24 hours agoCanada Desperately Needs a Baby Bump