COVID-19
BREAKING: Days before Trump Inauguration HHS fires doctor in charge of gain of function research project

Dr. Daszak will likely be protected by the DoD & CIA from additional penalties.

By John Leake
HHS Formally Debars EcoHealth Alliance, President Peter Daszak Fired.
On January 17, 2025—just three days before President Trump is to be sworn in—Congress issued a press release with the following statement:
Today, after an eight-month investigation, the U.S. Department of Health and Human Services (HHS) cut off all funding and formally debarred EcoHealth Alliance Inc. (EcoHealth) and its former President, Dr. Peter Daszak, for five years based on evidence uncovered by the Select Subcommittee on the Coronavirus Pandemic.
As far as I can tell, the New York Times did not report this story, though the New York Post did.
More interesting than the superficial news reporting is the HHS ACTION REFERRAL MEMORANDUM recommending that Dr. Peter Daszak be barred from participating in United States Federal Government procurement and nonprocurement programs.
The Memorandum also states:
Dr. Peter Daszak was the President and Chief Executive Officer of EHA from 2009 until his termination, effective January 6, 2025. Dr. Daszak was the Project Director (PD)/Principal Investigator (PI) for Grant Number 1R01AI110964-01.
I am not sure what to make of this document, which is written in such an arcane and convoluted style that it challenges the attention span of even the most focused reader.
I have been researching this story for four years, and I found the following paragraphs the most intriguing:
9. In a letter dated May 28, 2016, the NIAID contacted EHA concerning possible GoF research based on information submitted in its most recent Year 2 RPPR. The NIAID notified EHA that GoF research conducted under Grant Number 5R01AI110964-03 would be subject to the October 17, 2014, United States Federal Government funding pause, and that per the funding pause announcement, new United States Federal Government funding would not be released for GoF research projects that may be reasonably anticipated to confer attributes to influenza, MERS, or SARS viruses such that the virus would have enhanced pathogenicity and/or transmissibility in mammals via the respiratory route. In the letter, the NIAID requested that EHA provide a determination within 15 days of the date of the letter as to whether EHA’s research under Grant Number 5R01AI110964-03 did or did not include GoF work subject to the funding pause.
10. In a letter dated June 8, 2016, EHA provided a response to the NIAID’s May 28, 2016 letter. EHA explained that the goal of its proposed work was to construct MERS and MERS-like chimeric CoVs in order to understand the potential origins of MERSCoV in bats by studying bat MERS-like CoVs in detail. EHA stated that it believed it was highly unlikely that the proposed work would have any pathogenic potential, but that should any of these recombinants show evidence of enhanced virus growth greater than certain specified benchmarks involving log growth increases, or grow more efficiently in human airway epithelial cells, EHA would immediately: (1) stop all experiments with the mutant, (2) inform the NIAID Program Officer of these results, and (3) participate in decision-making trees to decide appropriate paths forward.
11. Based on the information provided by EHA, the NIAID concluded that the proposed work was not subject to the GoF research pause. In a letter dated July 7, 2016, however, the NIAID informed EHA that should any of the MERS-like or SARS-like chimeras generated under the grant show evidence of enhanced virus growth greater than 1 log over the parental backbone strain, EHA must stop all experiments with these viruses and provide the NIAID Program Officer and Grants Management Specialist, and WIV Institutional Biosafety Committee, with the relevant data and information related to these unanticipated outcomes.
Note that various statements in the above paragraphs are inconsistent with what Baric et al. state in their 2015 paper A SARS-like cluster of circulating bat coronavirus shows potential for human emergence—a research paper funded by the NIAID EcoHealth Grant “Understanding the Risk of Bat Coronavirus Emergence.”
As the authors state in the section on Biosafety and biosecurity:
Reported studies were initiated after the University of North Carolina Institutional Biosafety Committee approved the experimental protocol (Project Title: Generating infectious clones of bat SARS-like CoVs; Lab Safety Plan ID: 20145741; Schedule G ID: 12279). These studies were initiated before the US Government Deliberative Process Research Funding Pause on Selected Gain-of-Function Research Involving Influenza, MERS and SARS Viruses (http://www.phe.gov/s3/
dualuse/Documents/gain-of- function.pdf). This paper has been reviewed by the funding agency, the NIH. Continuation of these studies was requested, and this has been approved by the NIH.
As I noted in my series of essays titled The Great SARS-CoV-2 Charade, one of the silliest lies told by Dr. Anthony Fauci has been his insistence that NIAID did not approve Gain-of-Function work by EcoHealth.
Fauci has repeatedly asserted this in a loud and vexed tone, as though he is outraged by the mere proposition. And yet, Ralph Baric and his colleagues—including Zhengli-Li Shi at the Wuhan Institute of Virology—plainly state in their 2015 paper that their Gain-of-Function experiments, performed in Baric’s UNC lab and Zhengli-Li Shi’s lab in Wuhan, were grandfathered in, given that they were funded before the 2014 Pause.
Another statement (in paragraph 11 of the recent HHS Action Referral Memo) that deserves special scrutiny is the following:
In a letter dated July 7, 2016, however, the NIAID informed EHA that should any of the MERS-like or SARS-like chimeras generated under the grant show evidence of enhanced virus growth greater than 1 log over the parental backbone strain, EHA must stop all experiments with these viruses and provide the NIAID Program Officer and Grants Management Specialist, and WIV Institutional Biosafety Committee, with the relevant data and information related to these unanticipated outcomes.
Again, it’s tough to interpret this statement, given that Baric et al. had, by the own admission, already generated chimeras that “replicate efficiently in primary human airway cells and achieve in vitro titers equivalent to epidemic strains of SARS-CoV.”
Let’s review what Baric et al. state in their Abstract about the functionality of the chimeric virus (named SHCOI4-MA15) they claimed to have generated. Using humanized mice (genetically modified to have primary human airway cells) as their experimental animals, the authors state:
Using the SARS-CoV reverse genetics system2, we generated and characterized a chimeric virus expressing the spike of bat coronavirus SHC014 in a mouse-adapted SARS-CoV backbone.
The results indicate that group 2b viruses encoding the SHC014 spike in a wild-type backbone can efficiently use multiple orthologs of the SARS receptor human angiotensin converting enzyme II (ACE2), replicate efficiently in primary human airway cells and achieve in vitro titers equivalent to epidemic strains of SARS-CoV. Additionally, in vivo experiments demonstrate replication of the chimeric virus in mouse lung with notable pathogenesis.
To this day, no legal authority that I am aware of has investigated the question: What became of the the chimeras SHC014-MA15 and WIV1-MA15? The latter chimera was documented by Baric et al. in their March 2016 paper titled SARS-like WIV1-CoV poised for human emergence—a chimera “that replaced the SARS spike with the WIV1 spike within the mouse-adapted backbone.”
What did the Wuhan Institute of Virology do with these chimeras? Did its researchers continue to modify and experiment with these chimeras?
Another exceedingly silly claim made by U.S. government officials—including members of Congress—is that the true origin of SARS-CoV-2 is likely to remain a mystery, given that the Chinese government and military will almost certainly never agree to perform a full and transparent investigation of their Wuhan Institute of Virology.
What did the U.S. government expect when it agreed to share cutting edge American biotechnology with the Wuhan Institute of Virology, which has long been known to be run by the Chinese military?
One grows weary of our U.S. government officials evading responsibility by pretending to be imbeciles or by revealing themselves to be true imbeciles.
If you found this post informative, please consider becoming a paid subscriber to our Substack. Penetrating the smoke and mirror show performed by the abominable U.S. government requires a great deal of time and effort.

From LifeSiteNews
Pfizer and Moderna’s mRNA COVID shots must now include warnings that they cause ‘extremely high risk’ of heart inflammation and irreversible damage in males up to age 24.
The Trump administration’s Food and Drug Administration (FDA) announced it will now require updated safety warnings on mRNA COVID-19 shots to include the “extremely high risk” of myocarditis/pericarditis and the likelihood of long-term, irreversible heart damage for teen boys and young men up to age 24.
The required safety updates apply to Comirnaty, the mRNA COVID shot manufactured by Pfizer Inc., and Spikevax, the mRNA COVID shot manufactured ModernaTX, Inc.
According to a press release, the FDA now requires each of those manufacturers to update the warning about the risks of myocarditis and pericarditis to include information about:
- the estimated unadjusted incidence of myocarditis and/or pericarditis following administration of the 2023-2024 Formula of mRNA COVID-19 shots and
- the results of a study that collected information on cardiac magnetic resonance imaging (cardiac MRI) in people who developed myocarditis after receiving an mRNA COVID-19 injection.
The FDA has also required the manufacturers to describe the new safety information in the adverse reactions section of the prescribing information and in the information for recipients and caregivers.
Additionally, the fact sheets for healthcare providers and for recipients and caregivers for Moderna COVID-19 shot and Pfizer-BioNTech COVID-19 shot, which are authorized for emergency use in individuals 6 months through 11 years of age, have also been updated to include the new safety information in alignment with the Comirnaty and Spikevax prescribing information and information for recipients and caregivers.
In a video published on social media, Dr. Vinay Prasad, director of the Center for Biologics Evaluation & Research Chief Medical and Scientific Officer, explained the alarming reasons for the warning updates.
While heart problems arose in approximately 8 out of 1 million persons ages 6 months to 64 years following reception of the cited shots, that number more than triples to 27 per million for males ages 12 to 24.
Prasad noted that multiple studies have arrived at similar findings.
COVID-19
Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

![]()
The Justice Centre for Constitutional Freedoms announces that a judge of the Ontario Court of Justice has ordered the RCMP and TD Bank to produce records relating to the freezing of Mr. Evan Blackman’s bank accounts during the 2022 Freedom Convoy protest.
Mr. Blackman was arrested in downtown Ottawa on February 18, 2022, during the federal government’s unprecedented use of the Emergencies Act. He was charged with mischief and obstruction, but he was acquitted of these charges at trial in October 2023.
However, the Crown appealed Mr. Blackman’s acquittal in 2024, and a new trial is scheduled to begin on August 14, 2025.
Mr. Blackman is seeking the records concerning the freezing of his bank accounts to support an application under the Charter at his upcoming retrial.
His lawyers plan to argue that the freezing of his bank accounts was a serious violation of his rights, and are asking the court to stay the case accordingly.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” says constitutional lawyer Chris Fleury.
“These records will hopefully reveal exactly how and why Mr. Blackman’s accounts were frozen,” he says.
Mr. Blackman agreed, saying, “I’m delighted that we will finally get records that may reveal why my bank accounts were frozen.”
This ruling marks a significant step in what is believed to be the first criminal case in Canada involving a proposed Charter application based on the freezing of personal bank accounts under the Emergencies Act.

Elon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump

RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate
CBS settles with Trump over doctored 60 Minutes Harris interview

Why it’s time to repeal the oil tanker ban on B.C.’s north coast
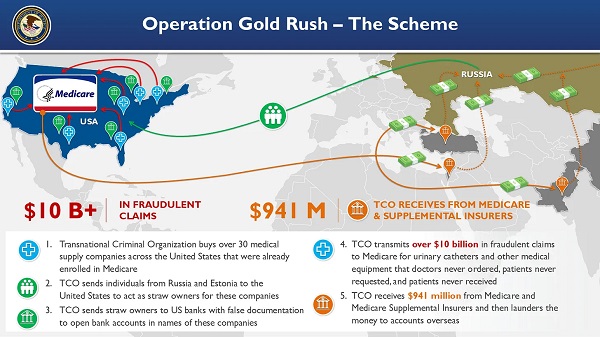
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud

Alberta Provincial Police – New chief of Independent Agency Police Service
-
 Carbon Tax2 days ago
Carbon Tax2 days agoCanada’s Carbon Tax Is A Disaster For Our Economy And Oil Industry
-
 Disaster2 days ago
Disaster2 days agoTexas flood kills 43 including children at Christian camp
-
 Daily Caller2 days ago
Daily Caller2 days agoTrump’s One Big Beautiful Bill Resets The Energy Policy Playing Field
-
 Alberta1 day ago
Alberta1 day agoAlberta Next: Immigration
-
 Business2 days ago
Business2 days agoThe Digital Services Tax Q&A: “It was going to be complicated and messy”
-
 International2 days ago
International2 days agoElon Musk forms America Party after split with Trump
-
 Crime14 hours ago
Crime14 hours agoNews Jeffrey Epstein did not have a client list, nor did he kill himself, Trump DOJ, FBI claim
-
COVID-1912 hours ago
FDA requires new warning on mRNA COVID shots due to heart damage in young men