Break The Needle
B.C. doubles down on involuntary care despite underinvestment


By Alexandra Keeler
B.C.’s push to replace coercive care with community models never took hold — and experts say province isn’t fixing that problem
Two decades ago, B.C. closed one of the last large mental institutions in the province. The institution, known as Riverview Hospital in Coquitlam, had at its peak housed nearly 5,000 patients across a sprawling campus.
There, patients with mental illnesses were subjected to a range of inhumane treatments, city records show. These included coma therapy, induced seizures, lobotomies and electroshock therapy.
When the province transferred patients out of institutions like Riverview during the 1990s and early 2000s, it promised them access to community-based mental health care instead. But that system never materialized.
“There was not a sustained commitment to seeing [the deinstitutionalization process] through,” said Julian Somers, a professor at Simon Fraser University who specializes in mental health, addiction and homelessness.
“[B.C.] did not put forward a clear vision of what we were trying to achieve and how we were going to get there. So we languished.”
Today, amid a sharp rise in involuntary hospitalizations, experts say B.C. risks repeating the mistakes of the past. The province is using coercive forms of care to treat individuals with mental health and substance use disorders, while failing to build community supports.
“We’re essentially doing the same thing we did with institutions,” said Somers, who began his clinical career at Riverview Hospital in the 1980s.
“[We’re] creating a system that doesn’t actually help people and may make things worse.”
 |
ECT machines and electrodes from the Riverview Hospital Artifact Collection. | City of Coquitlam
Riverview’s legacy
B.C.’s push for deinstitutionalization was driven by growing evidence that large psychiatric institutions were harmful, and that community-based care was more humane and cost effective.
Nationally, advances in antipsychotic medication, rising civil rights concerns and growing financial pressures were also spurring a shift away from institutional care.
A 2006 Senate report showed community care could match institutional care in both effectiveness and cost — provided it was properly funded.
“There was sufficient evidence demonstrating that people with severe mental illness had better outcomes in community settings,” said Somers.
Somers says people who stay long term in institutions can develop “institutionalization syndrome,” characterized by increased dependency, worse mental health outcomes and greater social decline.
At the time, B.C. was restructuring its health system, promising to replace institutions like Riverview with a regional network of mental health services.
The problem was, that network never fully materialized.
Marina Morrow, a professor at York University’s School of Health Policy and Management who tracked B.C.’s deinstitutionalization process, says the province placed patients in alternative care. But these providers were not always well-equipped to manage psychiatric patients.
“Nobody left Riverview directly to the street,” Morrow said. “But some … might have ended up being homeless over time.”
A 2012 study led by Morrow found that older psychiatric Riverview patients who were relocated to remote regional facilities strained overburdened and ill-equipped staff, leading to poor patient outcomes.
Somers says B.C. abandoned its vision of a robust, community-based system.
“We allowed BC Housing to have responsibility for mental health and addiction housing,” he said. “And no one explained to BC Housing how they ought to best fulfill that responsibility.”
Somers says the province’s reliance on group housing was part of the problem. Group housing isolates residents from broader society, instead of integrating them into a community. A 2013 study by Somers shows people tend to have better outcomes if they get to live in “scattered-site housing,” where tenants live in diverse neighbourhoods while still receiving personalized support.
“All of us … are influenced substantially by where we live, what we do, and who we do things with,” he said.
Somers says a greater investment in community care would have emphasized better housing, nutrition, education, work and social connection. “Those are all way more important than medical care in terms of the health of the population,” he said.
“We closed institutions having no [alternative] functioning model.”
Reinstitutionalization
Despite B.C.’s efforts to deinstitutionalize, the practice of institutionalizing certain patients never truly went away.
“We institutionalize way more people now than we ever did, even at peak Riverview population,” said Laura Johnston, legal director at Health Justice, a B.C. non-profit focused on coercive health laws.
Between 2008 and 2018, involuntary hospitalizations rose nearly 66 per cent, while voluntary admissions remained flat.
In the 2023-24 fiscal year, more than 25,000 individuals were involuntarily hospitalized at acute care facilities, down only slightly from 26,600 the previous year, according to B.C.’s health ministry. These admissions involved about 18,000 unique patients, indicating many individuals were detained more than once.
Subscribe for free to get Break The Needle’s latest news and analysis – or donate to our investigative journalism fund.
In September 2024, a string of high-profile attacks in Vancouver by individuals with histories of mental illness reignited public calls to reopen Riverview Hospital.
That month, B.C. Premier David Eby pledged to further expand involuntary care. Currently, B.C. has 75 designated facilities that can hold individuals admitted under the Mental Health Act. The act permits individuals to be involuntarily detained if they have a mental disorder requiring treatment and are significantly impaired. These existing facilities host about 2,000 beds for involuntary patients.
Eby’s pledge was to add another 400 hospital-based mental health beds, and two new secure care facilities within correctional facilities.
Johnston, of Health Justice, says Eby’s announcement merely continues the same flawed approach. It “[ties] access to services with detention and an involuntary care approach, rather than investing in the voluntary, community-based services that we’re so sorely lacking in B.C.”
Kathryn Embacher, provincial executive director of adult mental health and substance use with BC Mental Health & Substance Use Services, says additional resources are needed to support those with complex needs.
“We continue to work with the provincial government to increase the services we are providing,” Embacher said. “Having enough resources to serve the most seriously ill clients is important to provide access to all clients.”
 |
θəqiʔ ɫəwʔənəq leləm’ (the Red Fish Healing Centre for Mental Health and Addiction) is for clients with complex and concurrent mental health and substance use disorders. | BC Mental Health and Substance Use Services website
Inertia
If B.C. wants to avoid repeating the mistakes of its past, it needs to change its approach, sources say.
One concern Johnston has is with Section 32 of the Mental Health Act. Largely unchanged since 1964, it grants broad powers to medical professionals to detain and control patients.
“It grants unchecked authority,” she said.
Data obtained by Health Justice show one in four involuntarily detained patients in B.C. is subjected to seclusion or restraint. And even this figure may understate the problem. B.C. only began reliably tracking its seclusion and restraint practices in 2020, and only collects data on the first three days of detention.
A B.C. health ministry spokesperson told Canadian Affairs that involuntary care is sometimes necessary when individuals in crisis pose a risk to themselves or others.
“It’s in these situations where a patient, who meets very specific criteria, may need to be held involuntarily under the Mental Health Act,” the spokesperson said.
But York University professor Morrow says those “specific criteria” are applied far too broadly. “We have this huge hammer [involuntary care] that sees everything as a nail,” she said. “Involuntary treatment was meant for rare, extreme cases. But that’s not how it’s being used today.”
Morrow advocates for reviving interdisciplinary care that brings psychiatry, psychology and primary care together in community-based settings. She pointed to several promising models, including Toronto’s Gerstein Crisis Centre, which provides community-based crisis services for those with mental health and substance use issues.
Somers sees Alberta’s recovery-oriented model as a potential blueprint. This model prioritizes live-in recovery communities that combine therapeutic support with job training and stable housing, and which permit residents to stay up to one year. Alberta has committed to building 11 such communities across the province.
“They provide people with respite,” Somers said.
“They provide them with the opportunity to practice and gain confidence, waking up each day, going through each day without drugs, seeing other people do it, gaining confidence that they themselves can do it.”
Johnston advocates for safeguards on involuntary treatment.
“There’s nothing in our laws that compels the health system to ensure that they’re offering community-based or voluntary based services wherever possible, and that they are not using involuntary care approaches without exhausting other options,” she said.
“There’s inertia in a system that’s operated this way for so long.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle.
Our content is always free – but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.

A Canadian poll finds that racial minorities don’t believe drug enforcement is bigoted.
By Adam Zivo
[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research]
Is drug prohibition racist? Many left-wing institutions seem to think so. But their argument is historically illiterate—and it contradicts recent polling data, too, which show that minorities overwhelmingly reject that view.
Policies and laws are tools to establish order. Like any tool, they can be abused. The first drug laws in North America, dating back to the late nineteenth and early twentieth centuries, arguably fixated on opium as a legal pretext to harass Asian immigrants, for example. But no reasonable person would argue that laws against home invasion, murder, or theft are “racist” because they have been misapplied in past cases. Absent supporting evidence, leaping from “this tool is sometimes used in racist ways” to “this tool is essentially racist” is kindergarten-level reasoning.
Yet this is precisely what institutions and activist groups throughout the Western world have done. The Drug Policy Alliance, a U.S.-based organization, suggests that drug prohibition is rooted in “racism and fear.” Harm Reduction International, a British NGO, argues for legalization on the grounds that drug prohibition entrenches “racialized hierarchies, which were established under colonial control and continue to dominate today.” In Canada, where I live, the top public health official in British Columbia, our most drug-permissive province, released a pro-legalization report last summer claiming that prohibition is “based on a history of racism, white supremacy, paternalism, colonialism, classism and human rights violations.”
These claims ignore how drug prohibition has been and remains popular in many non-European societies. Sharia law has banned the use of mind-altering substances since the seventh century. When Indigenous leaders negotiated treaties with Canadian colonists in the late 1800s, they asked for “the exclusion of fire water (whiskey)” from their communities. That same century, China’s Qing Empire banned opium amid a national addiction crisis. “Opium is a poison, undermining our good customs and morality,” the Daoguang emperor wrote in an 1810 edict.
Today, Asian and Muslim jurisdictions impose much stiffer penalties on drug offenders than do Western nations. In countries like China, Saudi Arabia, Iran, Singapore, and Thailand, addicts and traffickers are given lengthy prison sentences or executed. Meantime, in Canada and the United States, de facto decriminalization has left urban cores littered with syringes and shrouded in clouds of meth.
The anti-drug backlash building in North America appears to be spearheaded by racial minorities. When Chesa Boudin, San Francisco’s former district attorney, was recalled in 2022, support for his ouster was highest among Asian voters. Last fall, 73 percent of Latinos backed California’s Proposition 36, which heightened penalties for drug crimes, while only 58 percent of white respondents did.
In Canada, the first signs of a parallel trend emerged during Vancouver’s 2022 municipal election, where an apparent surge in Chinese Canadian support helped install a slate of pro-police candidates. Then, in British Columbia’s provincial election last autumn, nonwhite voters strongly preferred the BC Conservatives, who campaigned on stricter drug laws. And in last month’s federal election, within both Vancouver and Toronto’s metropolitan areas, tough-on-crime conservatives received considerable support from South Asian communities.
These are all strong indicators that racial minorities do not, in fact, universally favor drug legalization. But their small population share means there is relatively little polling data to measure their preferences. Since only 7.6 percent of Americans are Asian, for example, a poll of 1,000 randomly selected people will yield an average of only 76 Asian respondents—too small a sample from which to draw meaningful conclusions. You can overcome this barrier by commissioning very large polls, but that’s expensive.
Nonetheless, last autumn, the Centre for Responsible Drug Policy (a nonprofit I founded and operate) did just that. In partnership with the Macdonald-Laurier Institute, we contracted Mainstreet Research to ask over 12,000 British Columbians: “Do you agree or disagree that criminalizing drugs is racist?”
The results undermine progressives’ assumptions. Only 26 percent of nonwhite respondents agreed (either strongly or weakly) that drug criminalization is racist, while over twice as many (56 percent) disagreed. The share of nonwhite respondents who strongly disagreed was three times larger than the share that strongly agreed (43.2 percent versus 14.3 percent). These results are fairly conclusive for this jurisdiction, given the poll’s sample size of 2,233 nonwhite respondents and a margin of error of 2 percent.
Notably, Indigenous respondents seemed to be the most anti-drug ethnic group: only 20 percent agreed (weakly or strongly) with the “criminalization is racist” narrative, while 61 percent disagreed. Once again, those who disagreed were much more vehement than those who agreed. With a sample size of 399 respondents, the margin of error here (5 percent) is too small to confound these dramatic results.
We saw similar outcomes for other minority groups, such as South Asians, Southeast Asians, Latinos, and blacks. While Middle Eastern respondents also seemed to follow this trend, the poll included too few of them to draw definitive conclusions. Only East Asians were divided on the issue, though a clear majority still disagreed that criminalization is racist.
As this poll was limited to British Columbian respondents, our findings cannot necessarily be assumed to hold throughout Canada and the United States. But since the province is arguably the most drug-permissive jurisdiction within the two countries, these results could represent the ceiling of pro-drug, anti-criminalization attitudes among minority communities.
Legalization proponents and their progressive allies take pride in being “anti-racist.” Our polling, however, suggests that they are not listening to the communities they profess to care about.
Our content is always free – but if you want to help us commission more high-quality journalism,
please consider getting a voluntary paid subscription.

City Counsellor Ron Kerr’s Blue Hat Memorial Project at the Tyee Spit in Campbell River, B.C., April 2025. | Courtesy of Ron Kerr
By Alexandra Keeler
The drug crisis is really a men’s mental health crisis, says Ron Kerr, the artist and city councillor behind a visually staggering project
Fifty thousand flags blanket the north end of Tyee Spit in Campbell River, B.C. — a staggering visual memorial to the lives lost in Canada’s opioid crisis since it was declared a public health emergency in 2016.
Called the Blue Hat Memorial Project, the installation spans nearly the length of a football field. It features 36,000 blue flags to represent the men and boys killed by toxic drugs, and 14,000 purple flags for women and girls.
“The actual installation does something you can’t do by just reading [about it],” said Ron Kerr, the artist behind the project. Kerr is also a city councillor in Campbell River, a city of 38,000 on the northeast coast of Vancouver Island.
“You’re visually seeing it, and it’s going right to your heart and creating an emotional response,” he said.
The installation’s name is a reference to the blue hard hats worn by newcomers or trainees on blue-collar job sites. Kerr says one of his aims is to draw attention to how the drug crisis has acutely affected working-class men. Between one-third and half of the individuals who died of opioid poisoning worked in the skilled trades, according to public health data.
Kerr, who has worked closely with tradesmen as an artist and advocate in men’s peer support groups, describes many of these tradesmen as “functional addicts” — employed, seemingly stable individuals who privately use drugs to manage pain or depression without others noticing.
“They are doing drugs at home or in their garage, and people don’t even know that they are [because] they’re functional, they’re working,” he said. “They’re able to control their depression or occupational injury through opiate drugs.”
Tradespeople are especially vulnerable to developing substance use disorders due to the physical demands, long hours and high injury rates associated with their work. Many use stimulants to stay alert or opioids to manage pain or cope with isolation in remote jobs.
“There is an expectation to get out the next day and get to work, no matter how you’re feeling,” said Kerr. “Self-medication is the easiest way to do it — a slippery slope from Tylenol to prescription drugs.”
A 2021 survey by the Construction Industry Rehabilitation Plan found that one in three B.C. construction workers reported problematic substance use. More than two-thirds screened positive for PTSD.
Loneliness is another major driver. Experts say men often avoid seeking help due to stigma, leading to further isolation.
“The opposite of addiction is connection,” said Kerr. “Men don’t have a place to go when they can’t deal with their issues, so they self-medicate.”
A pattern flipped
When Kerr first launched the installation in August 2024, he and a team of volunteers initially planted only blue flags. But in response to questions like, “Where are the women?”, he added purple flags this year.
“It was a blending — to give them their due,” he said.
Kerr’s installation sits on the unceded territory of the Liǧʷiłdax̌ʷ people, including the Wei Wai Kum Nation, a nation of nearly 1,000 people.
Wei Wai Kum’s chief, Chris Roberts, told Canadian Affairs he does not want the project’s focus on men to overshadow other key trends.
In B.C., Indigenous people die from drug poisoning at nearly seven times the rate of the general population. And within many Indigenous communities, the gendered pattern is at odds with national trends: women are dying at even higher rates than men.
“The opioid crisis has significantly affected my community as well, and it continues to — we are overrepresented as Indigenous people,” Roberts said.
“In our case, the gender split is much more balanced,” he added.
 |
An aerial view of the Blue Hat Memorial Project in Campbell River, B.C., April 2025. | Courtesy of Ron Kerr
‘Inadequate recovery’
Currently, Campbell River — the overdose epicentre of northern Vancouver Island — has only one aging recovery centre.
“[The city is] a hub for the whole North Island, but we have very little in terms of recovery,” said Kerr. “[There is] just one inadequate recovery centre in a 50-60 year old house with tiny rooms.”
Kerr is critical of how B.C. has implemented harm reduction strategies. He says policies such as drug decriminalization and safer supply were launched without the recovery infrastructure needed to make them effective.
“[Portugal] legalized drugs too, but the most important thing was that they provided the recovery services for them — they went all in,” said Kerr. “In this province, they just haven’t spent the money and time on doing that.”
Kerr also worries too many resources have gone to safer supply programs, without offering drug users a way out.
“When you get a person in full-blown addiction, and you’re giving them all the drugs they need, the food they need, and the clothes and shelter, what’s going to stop them from carrying on?” he said.
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Kerr wants his installation to draw attention to the need for more recovery-oriented solutions, such as treatment centres and housing. In particular, he points to a lack of affordable or free housing for people to live in after initial recovery.
“What you need is a good, clear off-ramp,” said Kerr. “They need to have recovery options that are either affordable or free so they can get off the road that they’re on.”
Chief Roberts agrees. Wei Wai Kai Nation is currently converting the former Tsạkwạ’lutạn resort into a 40-bed healing centre that will combine medical care with culture-based recovery.
“We’ve made investments to acquire properties and assets where people can go and reconnect with the land, the territory and their identity as a Ligwilda’xw person,” Roberts said.
Kerr says he will consider the Blue Hat Memorial a success if it leads to more funding and momentum for these types of recovery-oriented services.
The Blue Hat Memorial remains in Campbell River until the end of April. But Kerr, who previously re-created the installation in Nanaimo and West Vancouver, says he remains committed to doing more projects.
“I’ve got no expectation of senior government to come along and do this without a groundswell of grassroots people saying ‘we need this,’ and pushing government to do it,” said Kerr.
“I’m going to keep having the installation until that happens.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle.
Our content is always free – but if you want to help us commission more high-quality journalism, consider getting a voluntary paid subscription.

Alberta providing additional $7 million to Grande Prairie to help transition to municipal police service

Federal government’s ‘affordable housing’ strategy doomed without strong income growth
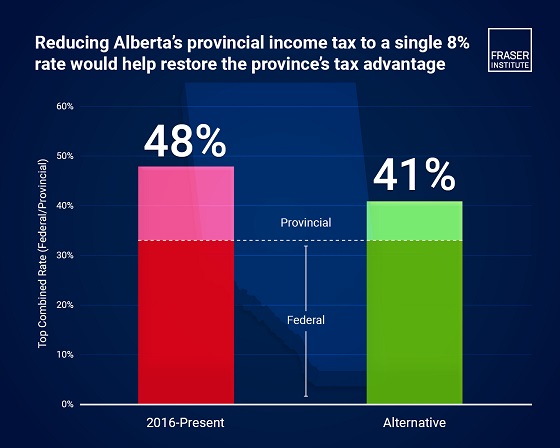
Moving to single 8% provincial personal income tax rate would help restore the Alberta Advantage

Judicial recounts give Conservatives 2 more seats, keeping Liberals short of majority

How Trump and Alberta might just save Canada
CDC no longer recommending COVID shots for healthy pregnant women, children

Dr. Malone: Trump admin takes step in right direction with new COVID shot guidance
-
 Economy15 hours ago
Economy15 hours agoCanada Treats Energy As A Liability. The World Sees It As Power
-
 Addictions1 hour ago
Addictions1 hour agoSaskatchewan launches small fleet of wellness buses to expand addictions care
-
 Indigenous16 hours ago
Indigenous16 hours agoCarney’s Throne Speech lacked moral leadership
-
 Fraser Institute16 hours ago
Fraser Institute16 hours agoAtlantic provinces should focus on growth—despite Carney’s transfer policies
-
 Business15 hours ago
Business15 hours agoBureaucracy balloons while less than 50 per cent of government performance targets are consistently met
-
 conflict10 hours ago
conflict10 hours ago“Will Be in History Books”: Zelensky Hails Long-Range Drone Strike That Hit Dozens of Russian Bombers
-
 Crime9 hours ago
Crime9 hours agoTerror in Boulder: Woman set on fire during pro-Israel hostage walk
-
 conflict2 days ago
conflict2 days agoBeijing ‘Imminent’ Threat to Taiwan: U.S. Defense Secretary Issues Stark Warning