Health
UK pediatrician who led review of child ‘transitions’ says US medical groups ‘misleading the public’


Dr. Hilary Cass, author of the Cass Review
From LifeSiteNews

The American Academy of Pediatrics’ support for surgically and chemically mutilating gender-confused children ‘is now demonstrated to be out of date by multiple systematic reviews,’ Dr. Hilary Cass told the New York Times.
The typically left-wing New York Times published an interview on Monday with consultant pediatrician Dr. Hilary Cass on her comprehensive review of so-called “gender medicine” in the United Kingdom, indicating that awareness of the damage due to surgical and chemical “transitioning” continues to spread despite the best efforts of LGBT activists.
Released in April, 366-page Cass Review was commissioned by National Health Service (NHS) England following ongoing scandals about the practices of British “gender clinics” such as the Gender Identity Development Service (GIDS), operated by the Tavistock and Portman NHS Foundation Trust. The four-year project consisted of comprehensive reviews of current research and international standards, as well as extensive interviews with gender-confused children and adults, family members, detransitioners, doctors, and activists.
It found that “gender medicine” is “built on shaky foundations” and that while such interventions require a great deal of caution, “quite the reverse happened in the field of [so-called] gender care for children,” and that “[w]hile a considerable amount of research has been published in this field, systematic evidence reviews demonstrated the poor quality of the published studies, meaning there is not a reliable evidence base upon which to make clinical decisions, or for children and their families to make informed choices.” Her findings led NHS to stop prescribing puberty blockers to children with gender confusion earlier this year.
Speaking to the Times, Cass explained that she was planning her retirement when she was first asked to tackle the project and was initially apprehensive about wading into the controversy.
“The most important concern for me is just how poor the evidence base is in this area,” she said. “Some people have questioned, ‘Did we set a higher bar for this group of young people?’ We absolutely didn’t. The real problem is that the evidence is very weak compared to many other areas of pediatric practice.”
The Times acknowledged that her “findings are in line with several European countries that have limited the treatments [sic] after scientific reviews. But in America, where nearly two dozen states have banned the care outright, medical groups have endorsed the treatments as evidence-based and necessary,” including groups the paper contacted for its latest story. Cass described American medical consensus as “out of date” on the issue.
“When I was president of the Royal College of Pediatrics and Child Health, we did some great work with the A.A.P. [American Academy of Pediatrics],” she elaborated. “They are an organization that I have enormous respect for. But I respectfully disagree with them on holding on to a position that is now demonstrated to be out of date by multiple systematic reviews.”
“It wouldn’t be too much of a problem if people were saying ‘This is clinical consensus and we’re not sure,” she added. “But what some organizations are doing is doubling down on saying the evidence is good. And I think that’s where you’re misleading the public. You need to be honest about the strength of the evidence and say what you’re going to do to improve it.”
A significant body of evidence shows that “affirming” gender confusion carries serious harms, especially when done with impressionable children who lack the mental development, emotional maturity, and life experience to consider the long-term ramifications of the decisions being pushed on them.
Studies find that more than 80% of children experiencing gender dysphoria outgrow it on their own by late adolescence, and that even full “reassignment” surgery often fails to resolve gender-confused individuals’ heightened tendency to engage in self-harm and suicide — and may even exacerbate it, including by reinforcing their confusion and neglecting the actual root causes of their mental strife.
Yet while mounting evidence against youth “gender transitions” is prompting European nations such as the United Kingdom and France, which are normally to the left of America, to move away from the practice, in America, the medical establishment and the Biden administration continues to dig in their heels, despite Biden’s own Substance Abuse & Mental Health Services Administration (SAMHSA) releasing a since-deleted report last year acknowledging that “lesbian, gay, and bisexual adults are more likely than straight adults to use substances, experience mental health conditions including major depressive episodes, and experience serious thoughts of suicide.”
The White House’s comprehensive pursuit of the transgender agenda has included reopening the military to recruits afflicted with gender dysphoria, promoting gender ideology within the military (including “diversity” and drag events on military bases), holding White House events to “affirm transgender kids,” condemning state laws against underage “transitions” as “close to sinful,” promoting underage “transitions” (potentially at taxpayer expense) as a “best practice,” and trying to force federally funded schools to let males into female athletic competitions and restrooms.

From the Brownstone Institute
Every morning, hundreds of millions of people perform a socially approved ritual. They line up for coffee. They joke about not being functional without caffeine. They openly acknowledge dependence and even celebrate it. No one calls this addiction degenerate. It is framed as productivity, taste, wellness—sometimes even virtue.
Now imagine the same professional discreetly using a nicotine pouch before a meeting. The reaction is very different. This is treated as a vice, something vaguely shameful, associated with weakness, poor judgment, or public health risk.
From a scientific perspective, this distinction makes little sense.
Caffeine and nicotine are both mild psychoactive stimulants. Both are plant-derived alkaloids. Both increase alertness and concentration. Both produce dependence. Neither is a carcinogen. Neither causes the diseases historically associated with smoking. Yet one has become the world’s most acceptable addiction, while the other remains morally polluted even in its safest, non-combustible forms.
This divergence has almost nothing to do with biology. It has everything to do with history, class, marketing, and a failure of modern public health to distinguish molecules from mechanisms.
Two Stimulants, One Misunderstanding
Nicotine acts on nicotinic acetylcholine receptors, mimicking a neurotransmitter the brain already uses to regulate attention and learning. At low doses, it improves focus and mood. At higher doses, it causes nausea and dizziness—self-limiting effects that discourage excess. Nicotine is not carcinogenic and does not cause lung disease.
Caffeine works differently, blocking adenosine receptors that signal fatigue. The result is wakefulness and alertness. Like nicotine, caffeine indirectly affects dopamine, which is why people rely on it daily. Like nicotine, it produces tolerance and withdrawal. Headaches, fatigue, and irritability are routine among regular users who skip their morning dose.
Pharmacologically, these substances are peers.
The major difference in health outcomes does not come from the molecules themselves but from how they have been delivered.
Combustion Was the Killer
Smoking kills because burning organic material produces thousands of toxic compounds—tar, carbon monoxide, polycyclic aromatic hydrocarbons, and other carcinogens. Nicotine is present in cigarette smoke, but it is not what causes cancer or emphysema. Combustion is.
When nicotine is delivered without combustion—through patches, gum, snus, pouches, or vaping—the toxic burden drops dramatically. This is one of the most robust findings in modern tobacco research.
And yet nicotine continues to be treated as if it were the source of smoking’s harm.
This confusion has shaped decades of policy.
How Nicotine Lost Its Reputation
For centuries, nicotine was not stigmatized. Indigenous cultures across the Americas used tobacco in religious, medicinal, and diplomatic rituals. In early modern Europe, physicians prescribed it. Pipes, cigars, and snuff were associated with contemplation and leisure.
The collapse came with industrialization.
The cigarette-rolling machine of the late 19th century transformed nicotine into a mass-market product optimized for rapid pulmonary delivery. Addiction intensified, exposure multiplied, and combustion damage accumulated invisibly for decades. When epidemiology finally linked smoking to lung cancer and heart disease in the mid-20th century, the backlash was inevitable.
But the blame was assigned crudely. Nicotine—the named psychoactive component—became the symbol of the harm, even though the damage came from smoke.
Once that association formed, it hardened into dogma.
How Caffeine Escaped
Caffeine followed a very different cultural path. Coffee and tea entered global life through institutions of respectability. Coffeehouses in the Ottoman Empire and Europe became centers of commerce and debate. Tea was woven into domestic ritual, empire, and gentility.
Crucially, caffeine was never bound to a lethal delivery system. No one inhaled burning coffee leaves. There was no delayed epidemic waiting to be discovered.
As industrial capitalism expanded, caffeine became a productivity tool. Coffee breaks were institutionalized. Tea fueled factory schedules and office routines. By the 20th century, caffeine was no longer seen as a drug at all but as a necessity of modern life.
Its downsides—dependence, sleep disruption, anxiety—were normalized or joked about. In recent decades, branding completed the transformation. Coffee became lifestyle. The stimulant disappeared behind aesthetics and identity.
The Class Divide in Addiction
The difference between caffeine and nicotine is not just historical. It is social.
Caffeine use is public, aesthetic, and professionally coded. Carrying a coffee cup signals busyness, productivity, and belonging in the middle class. Nicotine use—even in clean, low-risk forms—is discreet. It is not aestheticized. It is associated with coping rather than ambition.
Addictions favored by elites are rebranded as habits or wellness tools. Addictions associated with stress, manual labor, or marginal populations are framed as moral failings. This is why caffeine is indulgence and nicotine is degeneracy, even when the physiological effects are similar.
Where Public Health Went Wrong
Public health messaging relies on simplification. “Smoking kills” was effective and true. But over time, simplification hardened into distortion.
“Smoking kills” became “Nicotine is addictive,” which slid into “Nicotine is harmful,” and eventually into claims that there is “No safe level.” Dose, delivery, and comparative risk disappeared from the conversation.
Institutions now struggle to reverse course. Admitting that nicotine is not the primary harm agent would require acknowledging decades of misleading communication. It would require distinguishing adult use from youth use. It would require nuance.
Bureaucracies are bad at nuance.
So nicotine remains frozen at its worst historical moment: the age of the cigarette.
Why This Matters
This is not an academic debate. Millions of smokers could dramatically reduce their health risks by switching to non-combustion nicotine products. Countries that have allowed this—most notably Sweden—have seen smoking rates and tobacco-related mortality collapse. Countries that stigmatize or ban these alternatives preserve cigarette dominance.
At the same time, caffeine consumption continues to rise, including among adolescents, with little moral panic. Energy drinks are aggressively marketed. Sleep disruption and anxiety are treated as lifestyle issues, not public health emergencies.
The asymmetry is revealing.
Coffee as the Model Addiction
Caffeine succeeded culturally because it aligned with power. It supported work, not resistance. It fit office life. It could be branded as refinement. It never challenged institutional authority.
Nicotine, especially when used by working-class populations, became associated with stress relief, nonconformity, and failure to comply. That symbolism persisted long after the smoke could be removed.
Addictions are not judged by chemistry. They are judged by who uses them and whether they fit prevailing moral narratives.
Coffee passed the test. Nicotine did not.
The Core Error
The central mistake is confusing a molecule with a method. Nicotine did not cause the smoking epidemic. Combustion did. Once that distinction is restored, much of modern tobacco policy looks incoherent. Low-risk behaviors are treated as moral threats, while higher-risk behaviors are tolerated because they are culturally embedded.
This is not science. It is politics dressed up as health.
A Final Thought
If we applied the standards used against nicotine to caffeine, coffee would be regulated like a controlled substance. If we applied the standards used for caffeine to nicotine, pouches and vaping would be treated as unremarkable adult choices.
The rational approach is obvious: evaluate substances based on dose, delivery, and actual harm. Stop moralizing chemistry. Stop pretending that all addictions are equal. Nicotine is not harmless. Neither is caffeine. But both are far safer than the stories told about them.
This essay only scratches the surface. The strange moral history of nicotine, caffeine, and acceptable addiction exposes a much larger problem: modern institutions have forgotten how to reason about risk.
Author


From the Frontier Centre for Public Policy
By Conrad Eder
Conrad Eder supports universal health care, but not Canada’s broken version. Despite massive spending, Canadians face brutal wait times. He argues it’s time to allow private options, as other countries do, without abandoning universality.
It’s not about money. It’s about the rules shaping how Canada’s health care system works
Canada’s health care system isn’t failing because it lacks funding or public support. It’s failing because governments have tied it to restrictive rules that block private medical options used in other developed countries to deliver timely care.
Canada spends close to $400 billion a year on health care, placing it among the highest-spending countries in the Organization for Economic Co-operation and Development (OECD). Yet the system continues to struggle with some of the longest waits for care, the fewest doctors per capita and among the lowest numbers of hospital beds in the OECD. This is despite decades of spending increases, including growth of 4.5 per cent in 2023 and 5.7 per cent in 2024, according to estimates from the Canadian Institute for Health Information.
Canadians are losing confidence that government spending is the solution. In fact, many don’t even think it’s making a difference.
And who could blame them? Median health care wait times reached 30 weeks in 2024, up from 27.7 weeks in 2023, which was up from 27.4 weeks in 2022, according to annual surveys by the Fraser Institute.
Nevertheless, politicians continue to tout our universal health care system as a source of national pride and, according to national surveys, 74 per cent of Canadians agree. Yet only 56 per cent are satisfied with it. This gap reveals that while Canadians value universal health care in principle, they are frustrated with it in practice.
But it isn’t universal health care that’s the problem; it’s Canada’s uniquely restrictive version of it. In most provinces, laws restrict physicians from working simultaneously in public and private systems and prohibit private insurance for medically necessary services covered by medicare, constraints that do not exist in most other universal health care systems.
The United Kingdom, France, Germany and the Netherlands all maintain universal health care systems. Like Canada, they guarantee comprehensive insurance coverage for essential health care services. Yet they achieve better access to care than Canada, with patients seeing doctors sooner and benefiting from shorter surgical wait times.
In Germany, there are both public and private hospitals. In France, universal insurance covers procedures whether patients receive them in public hospitals or private clinics. In the Netherlands, all health insurance is private, with companies competing for customers while coverage remains guaranteed. In the United Kingdom, doctors working in public hospitals are allowed to maintain private practices.
All of these countries preserved their commitment to universal health care while allowing private alternatives to expand choice, absorb demand and deliver better access to care for everyone.
Only 26 per cent of Canadians can get same-day or next-day appointments with their family doctor, compared to 54 per cent of Dutch and 47 per cent of English patients. When specialist care is needed, 61 per cent of Canadians wait more than a month, compared to 25 per cent of Germans. For elective surgery, 90 per cent of French patients undergo procedures within four months, compared to 62 per cent of Canadians.
If other nations can deliver timely access to care while preserving universal coverage, so can Canada. Two changes, inspired by our peers, would preserve universal coverage and improve access for all.
First, allow physicians to provide services to patients in both public and private settings. This flexibility incentivizes doctors to maximize the time they spend providing patient care, expanding service capacity and reducing wait times for all patients. Those in the public system benefit from increased physician availability, as private options absorb demand that would otherwise strain public resources.
Second, permit private insurance for medically necessary services. This would allow Canadians to obtain coverage for private medical services, giving patients an affordable way to access health care options that best suit their needs. Private insurance would enable Canadians to customize their health coverage, empowering patients and supporting a more responsive health care system.
These proposals may seem radical to Canadians. They are not. They are standard practice everywhere else. And across the OECD, they coexist with universal health care. They can do the same in Canada.
Alberta has taken an important first step by allowing some physicians to work simultaneously in public and private settings through its new dual-practice model. More Canadian provinces should follow Alberta’s lead and go one step further by removing legislative barriers that prohibit private health insurance for medically necessary services. Private insurance is the natural complement to dual practice, transforming private health care from an exclusive luxury into a viable option for Canadian families.
Canadians take pride in their health care system. That pride should inspire reform, not prevent it. Canada’s health care crisis is real. It’s a crisis of self-imposed constraints preventing our universal system from functioning at the level Canadians deserve.
Policymakers can, and should, preserve universal health care in this country. But maintaining it will require a willingness to learn from those who have built systems that deliver universality and timely access to care, something Canada’s current system does not.
Conrad Eder is a policy analyst at the Frontier Centre for Public Policy.


Remembering Afghanistan and the sacrifices of our military families

How to talk about housing at the holiday dinner table

US Under Secretary of State Slams UK and EU Over Online Speech Regulation, Announces Release of Files on Past Censorship Efforts

Sweden Fixed What Canada Won’t Even Name
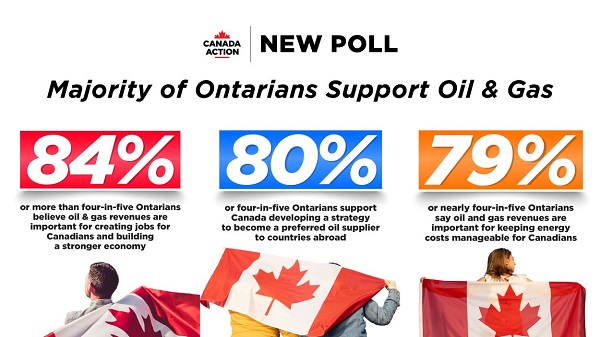
New Poll Shows Ontarians See Oil & Gas as Key to Jobs, Economy, and Trade

Alberta Next Panel calls for less Ottawa—and it could pay off

“Magnitude cannot be overstated”: Minnesota aid scam may reach $9 billion
-
 Alberta2 days ago
Alberta2 days agoThe Canadian Energy Centre’s biggest stories of 2025
-
 Business2 days ago
Business2 days agoResurfaced Video Shows How Somali Scammers Used Day Care Centers To Scam State
-
 Business17 hours ago
Business17 hours agoDark clouds loom over Canada’s economy in 2026
-
Addictions13 hours ago
Coffee, Nicotine, and the Politics of Acceptable Addiction
-
 Business2 days ago
Business2 days agoOttawa Is Still Dodging The China Interference Threat
-
 Business2 days ago
Business2 days agoMinneapolis day care filmed empty suddenly fills with kids
-
 Business2 days ago
Business2 days agoDisclosures reveal Minnesota politician’s husband’s companies surged thousands-fold amid Somali fraud crisis
-
Business16 hours ago
Federal funds FROZEN after massive fraud uncovered: Trump cuts off Minnesota child care money