Health
‘Transgender’ males have 51% higher death rate than general population: study

From LifeSiteNews
Research found that men who underwent a ‘gender transition’ using hormones have a 51% higher mortality rate than the general population and a ‘threefold’ greater risk of cardiovascular deaths.
A newly published study has found that males’ use of estrogen to present as “female” triples their risk of cardiovascular disease, while also heightening the risk of stroke, blood clots, depression, and cognitive impairment.
The journal Discover Mental Health on June 12 released a variety of findings regarding the negative impacts of estrogen use in males attempting to transition to “female.” One of the most significant was that current estrogen use “was associated with a threefold increased risk of death from cardiovascular events.”
In fact, a study of 966 “female transitioned” males were found to have a mortality rate 51 percent higher than that of the general population. Their main causes of death included cardiovascular disease (21 percent), cancer (32 percent), suicide (7.5 percent), and infection-related disease (five percent).
Estrogen use by males amplified other cardiovascular risks, especially with prolonged use. One meta-analysis found a 30 percent higher rate of stroke among gender-confused men who took estrogen compared with men who did not.
A review also found “strong evidence” that estrogen use by men increases their risk for vein blood clots “over fivefold.”
Estrogen use was also found to have a detrimental cognitive impact on men. For example, so-called “female transitioned” males were found to have lower scores than both their other male counterparts and women in “information-processing speed and episodic memory.”
In addition, elevated symptoms of depression were “associated with increased serum levels of estradiol” for men under the age of 60.
This recent study confirms 2023 study that found that all gender-confused individuals, whether men attempting to present themselves as women or women attempting to present themselves as men, were at significantly increased risk for a range of deadly cardiovascular conditions, including strokes, heart attacks, high blood pressure, and elevated cholesterol levels.
A 2019 study published by the National Institutes of Health (NIH) National Library of Medicine also found:
Cardiovascular disease (CVD) is the leading disease-specific cause of death for [so-called] transgender people undergoing [transgender procedures], with only suicide claiming more lives as the leader of all cause mortality.
However, for [gender-confused males], the risk of death from CVD is 3-fold higher than for all other groups.
Research reported by both the British Heart Association and the American Heart Association that same year arrived at similar findings:
“We already know sex hormones are important to cardiovascular health, and now we have people being exposed to high levels of sex hormones they normally would not have, which could be associated with cardiovascular benefit or risk,” said Dr. Christian Delles, a professor at the Institute of Cardiovascular and Medical Sciences at the University of Glasgow.
Business
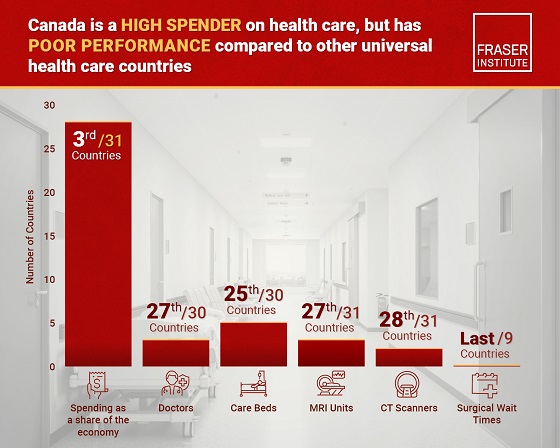
Canada has fewer doctors, hospital beds, MRI machines—and longer wait times—than most other countries with universal health care
From the Fraser Institute
Despite a relatively high level of spending, Canada has significantly fewer doctors, hospital beds, MRI machines and CT scanners compared to other countries with universal health care, finds a new study released today by the Fraser Institute, an independent, non-partisan Canadian public policy think-tank.
“There’s a clear imbalance between the high cost of Canada’s health-care system and the actual care Canadians receive in return,” said Mackenzie Moir, senior policy
analyst at the Fraser Institute and author of Comparing Performance of Universal Health-Care Countries, 2025.
In 2023, the latest year of available comparable data, Canada spent more on health care (as a percentage of the economy/GDP, after adjusting for population age) than
most other high-income countries with universal health care (ranking 3rd out of 31 countries, which include the United Kingdom, Australia and the Netherlands).
And yet, Canada ranked 27th (of 30 countries) for the availability of doctors and 25th (of 30) for the availability of hospital beds.
In 2022, the latest year of diagnostic technology data, Canada ranked 27th (of 31 countries) for the availability of MRI machines and 28th (of 31) for CT scanners.
And in 2023, among the nine countries with universal health-care systems included in the Commonwealth Fund’s International Health Policy Survey, Canada ranked last for the percentage of patients able to make same- or next-day appointments when sick (22 per cent) and had the highest percentage of patients (58 per cent) who waited two months or more for non-emergency surgery. For comparison, the Netherlands had much higher rates of same- or next-day appointments (47 per cent) and much lower waits of two months or more for non-emergency surgery (20 per cent).
“To improve health care for Canadians, our policymakers should learn from other countries around the world with higher-performing universal health-care systems,”
said Nadeem Esmail, director of health policy at the Fraser Institute.
Comparing Performance of Universal Health Care Countries, 2025
- Of the 31 high-income universal health-care countries, Canada ranks among the highest spenders, but ranks poorly on both the availability of most resources and access to services.
- After adjustments for differences in the age of the population of these 31 countries, Canada ranked third highest for spending as a percentage of GDP in 2023 (the most recent year of comparable data).
- Across 13 indictors measured, the availability of medical resources and timely access to medical services in Canada was generally below that of the average OECD country.
- In 2023, Canada ranked 27th (of 30) for the relative availability of doctors and 25th (of 30) for hospital beds dedicated to physical care. In 2022, Canada ranked 27th (of 31) for the relative availability of Magnetic Resonance Im-aging (MRI) machines, and 28th (of 31) for CT scanners.
- Canada ranked last (or close to last) on three of four indicators of timeliness of care.
- Notably, among the nine countries for which comparable wait times measures are available, Canada ranked last for the percentage of patients reporting they were able to make a same- or next-day appointment when sick (22%).
- Canada also ranked eighth worst for the percentage of patients who waited more than one month to see a specialist (65%), and reported the highest percentage of patients (58%) who waited two months or more for non-emergency surgery.
- Clearly, there is an imbalance between what Canadians get in exchange for the money they spend on their health-care system.

Mackenzie Moir
Senior Policy Analyst, Fraser Institute

From the Frontier Centre for Public Policy
By Ian Madsen
Doctors waste millions of hours on useless admin. It’s enough to end Canada’s doctor shortage. Ian Madsen says slashing red tape, not just recruiting, is the fastest fix for the clogged system.
Doctors spend more time on paperwork than on patients and that’s fueling Canada’s health care wait lists
Canada doesn’t just lack doctors—it squanders the ones it has. Mountains of paperwork and pointless admin chew up tens of millions of physician hours every year, time that could erase the so-called shortage and slash wait lists if freed for patient care.
Recruiting more doctors helps, but the fastest cure for our sick system is cutting the bureaucracy that strangles the ones already here.
The Canadian Medical Association found that unnecessary non-patient work consumes millions of hours annually. That’s the equivalent of 50.5 million patient visits, enough to give every Canadian at least one appointment and likely erase the physician shortage. Meanwhile, the Canadian Institute for Health Information estimates more than six million Canadians don’t even have a family doctor. That’s roughly one in six of us.
And it’s not just patients who feel the shortage—doctors themselves are paying the price. Endless forms don’t just waste time; they drive doctors out of the profession. Burned out and frustrated, many cut their hours or leave entirely. And the foreign doctors that health authorities are trying to recruit? They might think twice once they discover how much time Canadian physicians spend on paperwork that adds nothing to patient care.
But freeing doctors from forms isn’t as simple as shredding them. Someone has to build systems that reduce, rather than add to, the workload. And that’s where things get tricky. Trimming red tape usually means more Information Technology (IT), and big software projects have a well-earned reputation for spiralling in cost.
Bent Flyvbjerg, the global guru of project disasters, and his colleagues examined more than 5,000 IT projects in a 2022 study. They found outcomes didn’t follow a neat bell curve but a “power-law” distribution, meaning costs don’t just rise steadily, they explode in a fat tail of nasty surprises as variables multiply.
Oxford University and McKinsey offered equally bleak news. Their joint study concluded: “On average, large IT projects run 45 per cent over budget and seven per cent over time while delivering 56 per cent less value than predicted.” If that sounds familiar, it should. Canada’s Phoenix federal payroll fiasco—the payroll software introduced by Ottawa that left tens of thousands of federal workers underpaid or unpaid—is a cautionary tale etched into the national memory.
The lesson isn’t to avoid technology, but to get it right. Canada can’t sidestep the digital route. The question is whether we adapt what others have built or design our own. One option is borrowing from the U.S. or U.K., where electronic health record (EHR) systems (the digital patient files used by doctors and hospitals) are already in place. Both countries have had headaches with their systems, thanks to legal and regulatory differences. But there are signs of progress.
The U.K. is experimenting with artificial intelligence to lighten the administrative load, and a joint U.K.-U.S. study gives a glimpse of what’s possible:
“… AI technologies such as Robotic Process Automation (RPA), predictive analytics, and Natural Language Processing (NLP) are transforming health care administration. RPA and AI-driven software applications are revolutionizing health care administration by automating routine tasks such as appointment scheduling, billing, and documentation. By handling repetitive, rule-based tasks with speed and accuracy, these technologies minimize errors, reduce administrative burden, and enhance overall operational efficiency.”
For patients, that could mean fewer missed referrals, faster follow-up calls and less time waiting for paperwork to clear before treatment. Still, even the best tools come with limits. Systems differ, and customization will drive up costs. But medicine is medicine, and AI tools can bridge more gaps than you might think.
Run the math. If each “freed” patient visit is worth just $20—a conservative figure for the value of a basic appointment—the payoff could hit $1 billion in a single year.
Updating costs would continue, but that’s still cheap compared to the human and financial toll of endless wait lists. Cost-sharing between provinces, Ottawa, municipalities and even doctors themselves could spread the risk. Competitive bidding, with honest budgets and realistic timelines, is non-negotiable if we want to dodge another Phoenix-sized fiasco.
The alternative—clinging to our current dysfunctional patchwork of physician information systems—isn’t really an option. It means more frustrated doctors walking away, fewer new ones coming in, and Canadians left to languish on wait lists that grow ever longer.
And that’s not health care—it’s managed decline.
Ian Madsen is a senior policy analyst at the Frontier Centre for Public Policy.

Canada’s privacy commissioner says he was not consulted on bill to ban dissidents from internet

Enbridge CEO says ‘there’s a good reason’ for Alberta to champion new oil pipeline

Former Trump Advisor Says US Must Stop UN ‘Net Zero’ Climate Tax On American Ships

Poland’s president signs new zero income tax law for parents with two children

Democracy Watch Renews Push for Independent Prosecutor in SNC-Lavalin Case

Long-Distance Field Goals Have Flipped The Field. Will The NFL Panic?

“Nation Building,” Liberal Style: We’re Fixing a Sewer, You’re Welcome, Canada
-
 Business7 hours ago
Business7 hours agoQuebecers want feds to focus on illegal gun smuggling not gun confiscation
-
 Uncategorized1 day ago
Uncategorized1 day agoNew report warns WHO health rules erode Canada’s democracy and Charter rights
-
 Business7 hours ago
Business7 hours agoEmission regulations harm Canadians in exchange for no environmental benefit
-
 Energy1 day ago
Energy1 day agoMinus Forty and the Myth of Easy Energy
-
 Courageous Discourse5 hours ago
Courageous Discourse5 hours agoNo Exit Wound – EITHER there was a very public “miracle” OR Charlie Kirk’s murder is not as it appears
-
 Crime1 day ago
Crime1 day agoFrance stunned after thieves loot Louvre of Napoleon’s crown jewels
-
 Frontier Centre for Public Policy2 days ago
Frontier Centre for Public Policy2 days agoOttawa Should Think Twice Before Taxing Churches
-
 Alberta2 days ago
Alberta2 days agoBusting five myths about the Alberta oil sands