Frontier Centre for Public Policy
The Destructive Legacy of Gender Theory’s Popular Pioneer


From the Frontier Centre for Public Policy
By Lee Harding

The idea that gender is disconnected from sex was popularized by psychologist John Money. Perverted minds produce perverted ideas. Unfortunately, Money’s legacy of destruction continues.
The idea that sex drives come out of nowhere and have nothing to do with biology should be dismissed out of hand, given the countless generations of procreated human and even animal species. Yet, in 1961, Money claimed that “erotic outlook and orientation is an autonomous psychological phenomenon independent of genes and hormones.”
Money later said that “like hermaphrodites, all the human race follow the same pattern, namely, of psychological undifferentiation at birth.”
In other words, no one is born heterosexual, and there are no biology-based differences in how men and women act. By 1973, even Money had to acknowledge a wide body of research that showed “fetal gonadal hormones . . . have an influence on neural pathways in the brain.” Still, he emphasized nurture over nature.
Money had a chance to test his theories after the birth of Winnipeg twin brothers Bruce and Ron Reimer, born in 1965. A botched circumcision left Bruce’s penis almost severed, seemingly damaged beyond function. Their parents saw Money on TV in 1967 and went to his gender clinic at Johns Hopkins University.
The clinic was the first of its kind and specialized in cross-sex surgeries. Money convinced the parents to have Bruce’s penis and testes removed, rename him Brenda, and raise him as a girl. Both twins visited Money annually, and Money used their example on a lecture circuit to insist that gender roles were instilled and not innate.
This was complete fiction, but the truth didn’t come out until it was exposed by psychologist H. Keith Sigmundson and biologist Milton Diamond in a medical journal in 1997.
The twins’ mother Janet recalled how Brenda hated dresses, sewing, and dolls. Instead, the child preferred to play soldier, dress in men’s clothes, tinker with tools and gadgets, and even stand up to pee. When Brenda told doctors “she” felt she wasn’t a girl, they discounted it.
It turns out Money made the twins inspect each other’s genitals. His therapy involved forcing the twins into a simulation of sexual positions and motions, something Money justified as healthy childhood sexual exploration. Money photographed this while as many as six colleagues looked in person. If either child resisted orders, the doctor responded with anger and verbal abuse.
This disturbing account is not entirely surprising. Money participated in nudism and group sex as part of the Society for the Scientific Study of Sexuality. He advocated open marriages and even compiled a pornographic presentation for students at Johns Hopkins Medical School called “Pornography in the Home.”
In his 1975 book Sexual Signatures, Money wrote, “[E]xplicit sexual pictures can and should be used as part of a child’s sex education…. [to] reinforce his or her own gender identity/role,” Money explained.
By the age of 13, Brenda so dreaded the annual visit to Money that she threatened suicide. Her parents sent her anyway. Consultants at the Baltimore clinic recruited male-to-female transsexuals to convince Reimer it was better to be female and have a vagina. This so disturbed Reimer, that she ran away from the hospital and hid on the roof of a nearby building.
In 1980, Reimer begged her father to know the truth and he finally admitted her birth as a male. The family moved and the child took the name David. Next, endocrinologists, psychologists, and surgeons did their best to reconstruct Reimer’s manliness. Money stopped talking about the twins on the lecture circuit but did not confess how woefully wrong he was.
In 1979, Dr. Paul McHugh, chief psychiatrist at Johns Hopkins Hospital, investigated whether their sex reassignment surgeries helped the psycho-social problems of patients. The answer was so clearly “no” that the clinic stopped doing them.
In 2004, McHugh recalled that those operated on “had much the same problems with relationships, work, and emotions as before.” He added, “I concluded that Hopkins was fundamentally cooperating with a mental illness. We psychiatrists, I thought, would do better to concentrate on trying to fix their minds and not their genitalia.”
When the gender clinic was shut down in 1980, Money started another clinic at Johns Hopkins for gender “paraphilias,” a polite term for deviancies. That year, he told Time magazine, “A childhood sexual experience, such as being the partner of a relative or of an older person, need not necessarily affect the child adversely.”
In 1991, Money told Paidika, a pro-pedophilia journal in the Netherlands that a mutually acceptable sexual relationship between a ten-year-old boy and a man in his 30s was not “pathological in any way.” He said efforts to keep children from sexual activity, including sexual consent laws, was “really a diabolically clever ploy to establish anti-sexualism on a big scale.”
David Reimer killed himself in 2004, while Money died in 2006. Too bad the psychologist’s warped ideas didn’t die with him. In practice, they lead to futility and failure.
Lee Harding is a Research Fellow for the Frontier Centre for Public Policy.

From the Frontier Centre for Public Policy
By Ian Madsen
Canada’s growing LNG exports are opening global markets and reducing dependence on U.S. prices, if Ottawa allows the pipelines and export facilities needed to reach those markets
Canada’s LNG advantage is clear, but federal bottlenecks still risk turning a rare opening into another missed opportunity
Canada is finally in a position to profit from global LNG demand. But that opportunity will slip away unless Ottawa supports the pipelines and export capacity needed to reach those markets.
Most major LNG and pipeline projects still need federal impact assessments and approvals, which means Ottawa can delay or block them even when provincial and Indigenous governments are onside. Several major projects are already moving ahead, which makes Ottawa’s role even more important.
The Ksi Lisims floating liquefaction and export facility near Prince Rupert, British Columbia, along with the LNG Canada terminal at Kitimat, B.C., Cedar LNG and a likely expansion of LNG Canada, are all increasing Canada’s export capacity. For the first time, Canada will be able to sell natural gas to overseas buyers instead of relying solely on the U.S. market and its lower prices.
These projects give the northeast B.C. and northwest Alberta Montney region a long-needed outlet for its natural gas. Horizontal drilling and hydraulic fracturing made it possible to tap these reserves at scale. Until 2025, producers had no choice but to sell into the saturated U.S. market at whatever price American buyers offered. Gaining access to world markets marks one of the most significant changes for an industry long tied to U.S. pricing.
According to an International Gas Union report, “Global liquefied natural gas (LNG) trade grew by 2.4 per cent in 2024 to 411.24 million tonnes, connecting 22 exporting markets with 48 importing markets.” LNG still represents a small share of global natural gas production, but it opens the door to buyers willing to pay more than U.S. markets.
LNG Canada is expected to export a meaningful share of Canada’s natural gas when fully operational. Statistics Canada reports that Canada already contributes to global LNG exports, and that contribution is poised to rise as new facilities come online.
Higher returns have encouraged more development in the Montney region, which produces more than half of Canada’s natural gas. A growing share now goes directly to LNG Canada.
Canadian LNG projects have lower estimated break-even costs than several U.S. or Mexican facilities. That gives Canada a cost advantage in Asia, where LNG demand continues to grow.
Asian LNG prices are higher because major buyers such as Japan and South Korea lack domestic natural gas and rely heavily on imports tied to global price benchmarks. In June 2025, LNG in East Asia sold well above Canadian break-even levels. This price difference, combined with Canada’s competitive costs, gives exporters strong margins compared with sales into North American markets.
The International Energy Agency expects global LNG exports to rise significantly by 2030 as Europe replaces Russian pipeline gas and Asian economies increase their LNG use. Canada is entering the global market at the right time, which strengthens the case for expanding LNG capacity.
As Canadian and U.S. LNG exports grow, North American supply will tighten and local prices will rise. Higher domestic prices will raise revenues and shrink the discount that drains billions from Canada’s economy.
Canada loses more than $20 billion a year because of an estimated $20-per-barrel discount on oil and about $2 per gigajoule on natural gas, according to the Frontier Centre for Public Policy’s energy discount tracker. Those losses appear directly in public budgets. Higher natural gas revenues help fund provincial services, health care, infrastructure and Indigenous revenue-sharing agreements that rely on resource income.
Canada is already seeing early gains from selling more natural gas into global markets. Government support for more pipelines and LNG export capacity would build on those gains and lift GDP and incomes. Ottawa’s job is straightforward. Let the industry reach the markets willing to pay.
Ian Madsen is a senior policy analyst at the Frontier Centre for Public Policy.

From the Frontier Centre for Public Policy
At what point does Ottawa admit its EV plan isn’t working?
Electric vehicles produce more pollution than the gas-powered cars they’re replacing.
This revelation, emerging from life-cycle and supply chain audits, exposes the false claim behind Ottawa’s more than $50 billion experiment. A Volvo study found that manufacturing an EV generates 70 per cent more emissions than building a comparable conventional vehicle because battery production is energy-intensive and often powered by coal in countries such as China. Depending on the electricity grid, it can take years or never for an EV to offset that initial carbon debt.
Prime Minister Mark Carney paused the federal electric vehicle (EV) mandate for 2026 due to public pressure and corporate failures while keeping the 2030 and 2035 targets. The mandate requires 20 per cent of new vehicles sold in 2026 to be zero-emission, rising to 60 per cent in 2030 and 100 per cent in 2035. Carney inherited this policy crisis but is reluctant to abandon it.
Industry failures and Trump tariffs forced Ottawa’s hand. Northvolt received $240 million in federal subsidies for a Quebec battery plant before filing for bankruptcy. Lion Electric burned through $100 million before announcing layoffs. Arrival, a U.K.-based electric van and bus manufacturer, collapsed entirely. Stellantis and LG Energy Solution extracted $15 billion for Windsor. Volkswagen secured $13 billion for St. Thomas.
The federal government committed more than $50 billion in subsidies and tax credits to prop up Canada’s EV industry. Ottawa defended these payouts as necessary to match the U.S. Inflation Reduction Act, which offers major incentives for EV and battery manufacturing. That is twice Manitoba’s annual operating budget. Every Manitoban could have had a two-year tax holiday with the public money Ottawa wasted on EVs.
Even with incentives, EVs reached only 15 per cent of new vehicle sales in 2024, far short of the mandated levels for 2026 and 2030. When federal subsidies ended in January 2025, sales collapsed to nine per cent, revealing the true level of consumer demand. Dealer lots overflowed with unsold inventory. EV sales also slowed in the U.S. and Europe in 2024, showing that cooling demand is a broader trend.
As economist Friedrich Hayek observed, “The curious task of economics is to demonstrate to men how little they really know about what they imagine they can design.” Politicians and bureaucrats cannot know what millions of Canadians know about their own needs. When federal ministers mandate which vehicles Canadians must buy and which companies deserve billions, they substitute the judgment of a few hundred officials for the collective wisdom of an entire market.
Bureaucrats draft regulations that determine the vehicles Canadians must purchase years from now, as if they can predict technology and consumer preferences better than markets.
Green ideology provided perfect cover. Invoke a climate emergency and fiscal responsibility vanishes. Question more than $50 billion in subsidies and you are labelled a climate denier. Point out the environmental costs of battery production, and you are accused of spreading misinformation.
History repeatedly teaches that central planning always fails. Soviet five-year plans, Venezuela’s resource nationalization and Britain’s industrial policy failures all show the same pattern. Every attempt to run economies from political offices ends in misallocation, waste and outcomes opposite to those promised. Concentrated political power cannot ever match the intelligence of free markets responding to real prices and constraints.
Markets collect information that no central planner can access. Prices signal scarcity and value. Profits and losses reward accuracy and punish error. When governments override these mechanisms with mandates and subsidies, they impair the information system that enables rational economic decisions.
The EV mandate forced a technological shift and failed. Billions in subsidies went to failing companies. Taxpayers absorbed losses while corporations walked away. Workers lost their jobs.
Canada needs a full repeal of the EV mandate and a retreat from PMO planners directing market decisions. The law must be struck, not paused. The contrived 2030 and 2035 targets must be abandoned.
Markets, not cabinet ministers, must determine what technologies Canadians choose.
Marco Navarro-Genie is vice-president of research at the Frontier Centre for Public Policy and co-author, with Barry Cooper, of Canada’s COVID: The Story of a Pandemic Moral Panic (2023).


Carney’s Toronto cabinet meetings cost $530,000

Health Canada report finds euthanasia now accounts for over 5% of deaths nationwide

What the Data Shows About the New Canada-Alberta Pipeline Opportunity

While Trump has southern border secure, hundreds of thousands of illegal immigrants still flooding in from Canada

Integration Or Indignation: Whose Strategy Worked Best Against Trump?

A Democracy That Can’t Take A Joke Won’t Tolerate Dissent

Alberta Sports Hall of Fame Announces Class of 2026 Inductees
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoUS Condemns EU Censorship Pressure, Defends X
-
 Bruce Dowbiggin1 day ago
Bruce Dowbiggin1 day agoWayne Gretzky’s Terrible, Awful Week.. And Soccer/ Football.
-
 Opinion2 days ago
Opinion2 days agoThe day the ‘King of rock ‘n’ roll saved the Arizona memorial
-
 Focal Points2 days ago
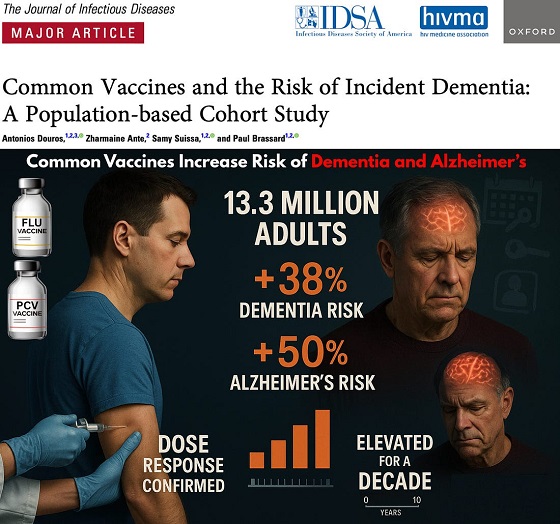
Focal Points2 days agoCommon Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s
-
 espionage1 day ago
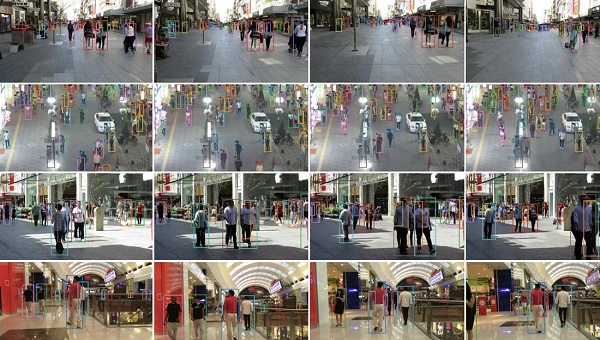
espionage1 day agoWestern Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns
-
 Business22 hours ago
Business22 hours agoCanada invests $34 million in Chinese drones now considered to be ‘high security risks’
-
 Agriculture1 day ago
Agriculture1 day agoCanada’s air quality among the best in the world
-
 Health1 day ago
Health1 day agoCDC Vaccine Panel Votes to End Universal Hep B Vaccine for Newborns