Health
RFK Jr. appoints Robert Malone, Martin Kulldorff, other COVID shot critics to overhauled CDC vaccine panel

From LifeSiteNews
By Robert Jones

Health and Human Services Secretary Robert F. Kennedy Jr. has announced eight appointments for the CDC’s top vaccine advisory panel, following his dismissal of all 17 previous members, citing a need to rebuild public trust in the federal immunization process.
On Monday, I took a major step towards restoring public trust in vaccines by reconstituting the Advisory Committee for Immunization Practices (ACIP). I retired the 17 current members of the committee. I’m now repopulating ACIP with the eight new members who will attend ACIP’s…
— Secretary Kennedy (@SecKennedy) June 11, 2025
RFK Jr. said the new Advisory Committee on Immunization Practices (ACIP) will demand “definitive safety and efficacy data” before issuing any new vaccine recommendations and will re-evaluate existing guidance. The restructured panel is set to convene on June 25.
The appointees include several prominent physicians and scientists, including former Harvard epidemiologist Martin Kulldorff and mRNA researcher Robert Malone, both known for their criticism of COVID-19-era public health policy and the COVID-19 shots.
Kulldorff helped draft the Great Barrington Declaration with Jay Bhattacharya and Sunetra Gupta, which called for focused protection rather than mass lockdowns – a position widely debated among epidemiologists. He also spoke out strongly against vaccine passports and mandates, as well as mask mandates and contact tracing. He was dismissed from Harvard in 2024 because of his refusal to receive the COVID-19 injections.
Malone, who conducted early work on mRNA vaccine delivery systems, was banned from several platforms for posts deemed “misleading” during the COVID crisis. He has given related interviews on The Joe Rogan Experience and elsewhere and was reinstated on X following Elon Musk’s revision of COVID-19 policies.
Retsef Levi, a professor at MIT, has raised concerns about potential cardiovascular risks linked to COVID-19 mRNA shots and has called for stricter safety monitoring. In 2023, a petition circulated opposing his work, though it did not gain traction.
Other appointees include:
- Joseph Hibbeln, an NIH psychiatrist and nutrition researcher focused on immune and neurodevelopmental health.
- Cody Meissner, a pediatric infectious disease expert with previous experience on both FDA and CDC vaccine panels.
- James Pagano, a veteran emergency physician with decades of clinical experience.
- Vicky Pebsworth, a nurse-scientist with prior FDA vaccine advisory roles and Pacific Region Director of the National Association of Catholic Nurses. She is also a Lay Dominican.
- Michael Ross, an OB-GYN and clinical researcher with a background in immunology and women’s health policy.
Joseph R. Hibbeln, MD, is a psychiatrist and neuroscientist with a career in clinical research, public health policy, and federal service. As former Acting Chief of the Section on Nutritional Neurosciences at the National Institutes of Health, he led research on immune regulation, neurodevelopment, and mental health. His work has informed U.S. public health guidelines, particularly in maternal and child health. With more than 120 peer-reviewed publications and extensive experience in federal advisory roles, Dr. Hibbeln brings expertise in immune-related outcomes, psychiatric conditions, and evidence-based public health strategies.
Martin Kulldorff, MD, PhD, is a biostatistician and epidemiologist formerly at Harvard Medical School and a leading expert in vaccine safety and infectious disease surveillance. He has served on the Food and Drug Administration’s Drug Safety and Risk Management Advisory Committee and the CDC’s Vaccine Safety Subgroup of the Advisory Committee on Immunization Practices, where he contributed to national vaccine safety monitoring systems. Dr. Kulldorff developed widely used tools such as SaTScan and TreeScan for detecting disease outbreaks and vaccine adverse events. His expertise includes statistical methods for public health surveillance, immunization safety, and infectious disease epidemiology. He has also been an influential voice in public health policy, advocating for evidence-based approaches to pandemic response.
Retsef Levi, PhD, is the Professor of Operations Management at the MIT Sloan School of Management and a leading expert in healthcare analytics, risk management, and vaccine safety. He has served as Faculty Director of MIT Sloan’s Food Supply Chain Analytics and Sensing Initiative and co-led the Leaders for Global Operations Program. Dr. Levi has collaborated with public health agencies to evaluate vaccine safety, including co-authoring studies on mRNA COVID-19 vaccines and their association with cardiovascular risks. His research has contributed to discussions on vaccine manufacturing processes, safety surveillance, and public health policy. Dr. Levi has also served on advisory committees and engaged in policy discussions concerning vaccine safety and efficacy. His expertise spans healthcare systems optimization, epidemiologic modeling, and the application of AI and data science in public health. Dr. Levi’s work continues to inform national and international debates on immunization safety and health system resilience.
Robert W. Malone, MD, is a physician-scientist and biochemist known for his early contributions to mRNA vaccine technology. He conducted foundational research in the late 1980s on lipid-mediated mRNA delivery, which laid the groundwork for later developments in mRNA-based therapeutics. Dr. Malone has held academic positions at institutions including the University of California, Davis, and the University of Maryland, and has served in advisory roles for the U.S. Department of Health and Human Services and the Department of Defense. His expertise spans molecular biology, immunology, and vaccine development.
Cody Meissner, MD, is a Professor of Pediatrics at the Geisel School of Medicine at Dartmouth and a nationally recognized expert in pediatric infectious diseases and vaccine policy. He has served as Section Chief of Pediatric Infectious Disease at Dartmouth-Hitchcock Medical Center and has held advisory roles with both the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA). Dr. Meissner has been a voting member of the CDC’s Advisory Committee on Immunization Practices and the FDA’s Vaccines and Related Biological Products Advisory Committee, where he has contributed to national immunization guidelines and regulatory decisions. His expertise spans vaccine development, immunization safety, and pediatric infectious disease epidemiology. Dr. Meissner has also been a contributing author to American Academy of Pediatrics policy statements and immunization schedules, helping shape national standards for pediatric care.
James Pagano, MD, is a board-certified Emergency Medicine physician with over 40 years of clinical experience following his residency at UCLA. He has worked in diverse emergency settings, from Level 1 trauma centers to small community hospitals, caring for patients across all age groups, including infants, pregnant women, and the elderly. Dr. Pagono served on multiple hospital committees, including utilization review, critical care, and medical executive boards. He is strong advocate for evidence-based medicine.
Vicky Pebsworth, OP, PhD, RN, earned a doctorate in public health and nursing from the University of Michigan. She has worked in the healthcare field for more than 45 years, serving in various capacities, including critical care nurse, healthcare administrator, health policy analyst, and research scientist with a focus on public health policy, bioethics, and vaccine safety. She is the Pacific Region Director of the National Association of Catholic Nurses. She is a former member of the Food and Drug Administration’s Vaccine and Related Biological Products Advisory Committee and the National Vaccine Advisory Committee’s 2009 H1N1 Vaccine Safety Risk Assessment Working Group and Vaccine Safety Working Group (Epidemiology and Implementation Subcommittees).
Michael A. Ross, MD, is a Clinical Professor of Obstetrics and Gynecology at George Washington University and Virginia Commonwealth University, with a career spanning clinical medicine, research, and public health policy. He has served on the CDC’s Advisory Committee for the Prevention of Breast and Cervical Cancer, where he contributed to national strategies for cancer prevention and early detection, including those involving HPV immunization. With research experience in hormone therapies, antibiotic trials, and immune-related conditions such as breast cancer prevention, Dr. Ross has engaged in clinical investigations with immunologic relevance. He has advised major professional organizations, including the American College of Obstetricians and Gynecologists, and contributed to federal advocacy efforts around women’s health and preventive care. His continued service on biotech and healthcare boards reflects his commitment to advancing innovation in immunology, reproductive medicine, and public health.
Kennedy framed the move as part of a broader campaign to remove conflicts of interest and restore credibility to federal vaccine recommendations. Just a few days ago, he accused the panel of having been “little more than a rubber stamp for any vaccine” and pledged that the new members would not have direct ties with the vaccine industry.
The new ACIP, he said, will be focused on what RFK called “gold-standard science” and “common sense.” The June meeting will mark the beginning of its work.

From LifeSiteNews
Jolene Van Alstine was approved for euthanasia after tiring of waiting years for surgery in Canada
A Canadian woman is looking to die by state-sanctioned euthanasia because she has had to endure long wait times to get what she considers to be proper care for a rare parathyroid disease.
The woman is Jolene Van Alstine, whose condition, normocalcemic primary hyperparathyroidism (nPHPT), causes her to experience vomiting, nausea, and bone pain.
As noted in a recent CBC report, Van Alstine claims she is not able to get proper surgery to remove her parathyroid in her home province of Saskatchewan, as there are no surgeons in that province who can perform that type of surgery.
She has said her “friends have stopped visiting me” and she is “isolated” and living “alone lying on the couch for eight years, sick and curled up in a ball, pushing for the day to end.”
“I go to bed at six at night because I can’t stand to be awake anymore,” she said.
As a result of her frustrations with the healthcare system, Van Alstine applied for Canada’s Medical Assistance in Dying (MAiD). She was approved for the procedure on January 7, 2026.
Saskatchewan Health Minister Jeremy Cockrill met with Van Alstine last month to try to see if he could help her, but what they talked about remains confidential.
“The Government of Saskatchewan expresses its sincere sympathy for all patients who are suffering with a difficult health diagnosis,” the government said.
As reported by LifeSiteNews, over 23,000 Canadians have died while on wait lists for medical care as Prime Minister Mark Carney’s Liberal government is focused on euthanasia expansions.
A new Euthanasia Prevention Coalition report revealed that Canada has euthanized 90,000 people since 2016, the year it was legalized.
Americans offering Jolene surgery help now say they have made contact with her
Van Alstine’s story has gone viral on the social media platform X, catching the attention of well-known American personalities, some who have claimed they can help her.
“If there is any surgeon in America who can do this, I’ll pay for this patient to come down here for treatment,” Glenn Beck wrote Tuesday on X.
“THIS is the reality of ‘compassionate’ progressive healthcare. Canada must END this insanity and Americans can NEVER let it spread here.”
According to Beck in a subsequent X post, he has had “surgeons who emailed us standing by to help her.”
“We are in contact with Jolene and her husband! Please continue to pray for her health,” he wrote on X.
“Will update more soon.”
As reported by LifeSiteNews recently, a Conservative MP’s private member’s bill that, if passed, would ban euthanasia for people with mental illness received the full support of the Euthanasia Prevention Coalition.
Lobby groups have pushed for MAiD to be expanded to minors.
Desiring to expand the procedure to even more Canadians, former Prime Minister Justin Trudeau’s government sought to expand from just the chronically and terminally ill to those suffering solely from mental illness. The current Liberal government appears to want to continue with the MAiD regime.
However, in February, after pushback from pro-life, medical, and mental health groups as well as most of Canada’s provinces, the federal government delayed the mental illness expansion until 2027.


ACIP voted to un-recommend the Hep B birth dose, but here’s the problem: they still can’t weigh the other side of the ledger
Sunday, something happened that has never happened in the history of American public health: ACIP voted 8-3 to un-recommend the universal birth dose of hepatitis B for babies born to mothers who test negative for the virus. After 34 years of jabbing every American newborn within hours of taking their first breath—regardless of whether their mother had hepatitis B—the committee finally acknowledged what 25 European countries figured out decades ago: it doesn’t make sense.
But watching this vote unfold, I couldn’t help but notice the absurdity of the debate itself. Committee members who opposed the change kept saying variations of the same thing: “We’ve heard ‘do no harm’ as a moral imperative. We are doing harm by changing this wording.” Another said “no rational science has been presented” to support the change.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
And therein lies the fundamental problem with ACIP—and with the entire vaccine regulatory apparatus in America. They literally cannot weigh risk versus benefit because they only have data on one side of the scale.
The Missing Side of the Ledger
When ACIP debates adding or removing a vaccine from the schedule, they can produce endless data on disease incidence. They can show you charts demonstrating how hepatitis B cases in infants dropped from thousands to single digits after 1991. They can model projected infections if vaccination rates decline. They have this data at their fingertips because tracking infectious disease is something our public health apparatus actually does.
But ask them to produce equivalent data on vaccine injury, and you’ll get silence. Not “the data shows injuries are rare.” Not “here’s our comprehensive tracking of adverse events.” Just… nothing. A void where information should be.
This is not an accident. This is by design.
The safety trials for Engerix-B and Recombivax HB—the two hepatitis B vaccines given to American newborns—monitored adverse events for four to five days after injection. That’s it. If your baby developed seizures on day six, or regressed into autism over the following months, or developed autoimmune disease in the following year—none of that would appear in the pre-licensure safety data.
And the post-market surveillance? VAERS is a voluntary reporting system that the CDC itself acknowledges captures only a tiny fraction of adverse events. A Harvard-funded study found it captures perhaps 1% of actual vaccine injuries. Vaccine court has paid out over $5 billion in claims while simultaneously being structured to make filing nearly impossible for average families.
So when Dr. Cody Meissner voted against removing the Hep B birth dose and said he saw “clear evidence of the benefits” but “not the harms,” he was accidentally revealing the entire rotten structure. Of course he doesn’t see the harms. Nobody is systematically looking for them.
The Invisibility of Vaccine Injury
Here’s what most people don’t understand about vaccine injury: it’s nothing like a gunshot wound.
If you shoot someone, the cause is obvious. There’s a bullet, a wound, blood, a clear mechanism of action visible to any observer. Even a medical examiner who’s never seen the victim before can determine cause of death.
Vaccine injury doesn’t work that way. When aluminum nanoparticles from a vaccine cross the blood-brain barrier via macrophages, when they lodge in brain tissue and trigger chronic neuroinflammation, when a child slowly regresses over weeks or months—there’s no bullet. There’s no smoking gun. There’s just a before and an after, and a desperate parent trying to explain to doctors that something changed.
This invisibility is the vaccine program’s greatest protection. Because the injury mechanism is complex and delayed, because it doesn’t leave an obvious wound, because it requires actually looking to find—and because no one in authority is looking—the injuries simply don’t exist in the official record.
I watched my own son Jamie regress after his vaccines. A healthy, developing toddler who lost his words, stopped making eye contact, and retreated into a world we couldn’t reach. My wife and I know what happened. Thousands of other parents know the same thing happened to their children. But because this type of injury doesn’t show up on a simple blood test, because there’s no autopsy finding that says “vaccine-induced encephalopathy,” ACIP members can sit in a room and say with straight faces that they don’t see evidence of harm.
They’re not lying. They literally can’t see it. Because no one is measuring it.
The Chicken Pox Conundrum
Here’s an example that illustrates the insanity of our current approach.
The varicella (chicken pox) vaccine was added to the schedule in 1995. It definitely reduces chicken pox cases. The data is clear on that front. Mission accomplished, right?
But what about the other side of the ledger?
Emerging research suggests that wild chicken pox infection provides some protective effect against brain cancers—particularly glioma, the most common type of primary brain tumor. Multiple studies have found that people who had chicken pox as children have significantly lower rates of brain cancer later in life. The hypothesis is that the immune response to wild varicella provides lasting immunological benefits that extend far beyond preventing itchy spots.
Meanwhile, the vaccine itself has been associated with increased rates of autoimmune conditions. Studies have linked varicella vaccination to higher rates of herpes zoster (shingles) outbreaks in younger age groups, to autoimmune disorders, to various adverse events that weren’t captured in the original short-term safety trials.
So what’s the true risk-benefit of the chicken pox vaccine? Does preventing a week of itchy discomfort in childhood justify potentially increased rates of brain cancer and autoimmune disease later in life?
ACIP can’t answer this question. They literally don’t have the data. They can show you chicken pox cases going down. They cannot show you a comprehensive analysis of long-term neurological and immunological outcomes in vaccinated versus unvaccinated populations, because that study has never been done.
And so they keep recommending the vaccine based on the only data they have—the disease prevention data—while remaining willfully blind to consequences they’ve never bothered to measure.
The ACIP Paradox
Sunday’s vote was historic, but it also revealed the fundamental paradox of vaccine regulation in America.
The committee members who voted to remove the universal Hep B birth dose recommendation did so largely based on comparative evidence from Europe, parental concerns, and the basic logic that vaccinating a 12-hour-old baby for a sexually transmitted disease their mother doesn’t have makes no medical sense. They were right to do so.
But the committee members who voted against the change weren’t wrong either, from their perspective. They looked at the only data they have—disease prevention data—and concluded that removing the recommendation could lead to more hepatitis B cases. And within their limited framework, they’re correct.
The problem is the framework itself.
True risk-benefit analysis requires data on both risks AND benefits. ACIP has comprehensive data on benefits (disease prevention) and virtually no data on risks (vaccine injury). So every decision they make is fundamentally flawed from the start.
When Dr. Joseph Hibbeln complained that “no rational science has been presented” to support changing the recommendations, he was inadvertently indicting the entire system. Of course no comprehensive vaccine injury data was presented—such data doesn’t exist because no one has been willing to collect it.
This is like asking someone to make an informed financial decision while only showing them potential profits and hiding all possible losses. Of course the decision will be skewed. Of course you’ll end up with a bloated portfolio of high-risk investments that look great on paper.
The Real Reform
If RFK Jr. and the new HHS leadership want to actually fix the vaccine program, they need to understand that removing individual vaccines or making them “optional” is just rearranging deck chairs on the Titanic.
The real reform is creating the data infrastructure that should have existed from the beginning.
We need a comprehensive, long-term, vaccinated-versus-unvaccinated health outcomes study. Not a five-day safety trial. A multi-decade tracking of neurological, immunological, and developmental outcomes across populations with varying vaccination status. Florida just eliminated all vaccine mandates—that state alone could provide the data we need within ten years if someone had the courage to actually collect it.
We need a vaccine injury surveillance system that actually captures adverse events. Not a voluntary reporting system that misses 99% of injuries. An active surveillance system with trained clinicians looking for the kinds of delayed, complex injuries that vaccines actually cause.
We need accountability for manufacturers. The 1986 National Childhood Vaccine Injury Act removed all liability from vaccine makers—and predictably, the vaccine schedule exploded afterward while safety research stagnated. Why would any company invest in safety when they can’t be sued for injuries?
Without this data, every ACIP meeting will be the same performance we watched this week: members confidently citing disease prevention data while admitting they can’t see evidence of harm—not because harm doesn’t exist, but because no one is looking for it.
What Comes Next
Sunday’s vote was a crack in the wall. For the first time, an American regulatory body acknowledged that perhaps vaccinating every newborn within hours of birth for a disease primarily transmitted through sex and IV drug use doesn’t make sense when the mother has already tested negative.
But the forces of institutional inertia are already mobilizing. The American Academy of Pediatrics is “disappointed.” The American Medical Association is calling for the CDC to reject the recommendation. The pharmaceutical industry—which collects over $225 million annually from Hep B birth doses alone—will fight to restore the universal recommendation.
They will cite the same data they always cite: disease prevention data. Cases prevented. Infections avoided. Lives saved—theoretically.
They will not cite vaccine injury data, because that data doesn’t exist in any comprehensive form. They will not present long-term health outcomes in vaccinated versus unvaccinated children, because those studies have been actively avoided for decades. They will not acknowledge the thousands of families who have watched their children regress after vaccination, because those injuries aren’t captured in any official database.
And this is why ACIP will always be hamstrung. Until we build the data infrastructure to actually measure vaccine injury—to put real numbers on the other side of the ledger—every vaccine decision will be based on incomplete information. Every “risk-benefit analysis” will be a fraud, because we’re only measuring half the equation.
The hepatitis B birth dose vote was a small victory. But the larger battle—for actual science, for complete data, for true informed consent—that battle is just beginning.
And until we win it, ACIP will continue making decisions in the dark, confidently citing evidence of benefits while remaining deliberately blind to the harms they’ve never bothered to measure.
About the author
 |
J.B. Handley is the proud father of a child with Autism. He spent his career in the private equity industry and received his undergraduate degree with honors from Stanford University. His first book, How to End the Autism Epidemic, was published in September 2018. The book has sold more than 75,000 copies, was an NPD Bookscan and Publisher’s Weekly Bestseller, broke the Top 40 on Amazon, and has more than 1,000 Five-star reviews. Mr. Handley and his nonspeaking son are also the authors of Underestimated: An Autism Miracle and co-produced the film SPELLERS, available now on YouTube.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


US Condemns EU Censorship Pressure, Defends X
The day the ‘King of rock ‘n’ roll saved the Arizona memorial

Canada invests $34 million in Chinese drones now considered to be ‘high security risks’
Western Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns

CDC Vaccine Panel Votes to End Universal Hep B Vaccine for Newborns
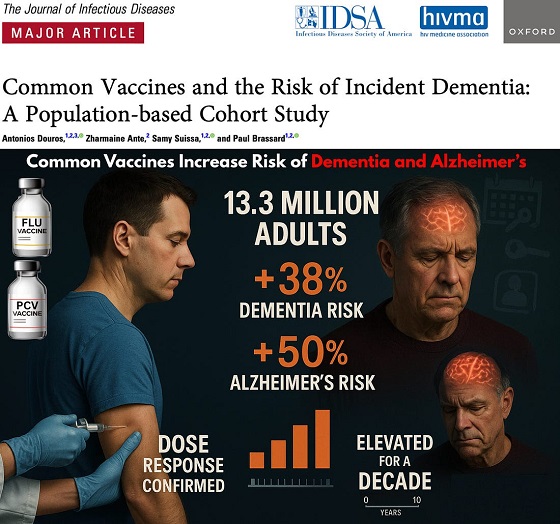
Common Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s

Wayne Gretzky’s Terrible, Awful Week.. And Soccer/ Football.
-
 Alberta1 day ago
Alberta1 day agoThe Recall Trap: 21 Alberta MLA’s face recall petitions
-
 illegal immigration1 day ago
illegal immigration1 day agoUS Notes 2.5 million illegals out and counting
-
 International1 day ago
International1 day agoTyler Robinson shows no remorse in first court appearance for Kirk assassination
-
 Energy2 days ago
Energy2 days agoCanada’s future prosperity runs through the northwest coast
-
 Business14 hours ago
Business14 hours agoInflation Reduction Act, Green New Deal Causing America’s Energy Crisis
-
 Daily Caller24 hours ago
Daily Caller24 hours ago‘There Will Be Very Serious Retaliation’: Two American Servicemen, Interpreter Killed In Syrian Attack
-
 Crime7 hours ago
Crime7 hours agoTerror in Australia: 12 killed after gunmen open fire on Hanukkah celebration
-
 Media7 hours ago
Media7 hours agoReporters determined to drive their industry and its reputation into the abyss one Tweet at a time