Addictions
Reckless: British Columbia’s “safe supply” fentanyl tablet experiment
From the MacDonald Laurier Institute
By Adam Zivo
While safer supply sounds nice in theory, addiction experts have found that drug users are reselling (“diverting”) a significant portion of their free hydromorphone on the black market to purchase harder substances. This has fuelled new addictions while generating handsome profits for organized crime.
Adam Zivo reviews the latest drug protocols adopted by the BC government and reports on their alarming lack of evidence and accountability.
British Columbia’s new drug protocols allow doctors throughout the province to prescribe “safer supply” drugs in a reckless manner.
In a new report titled Reckless: British Columbia’s “safe supply” fentanyl tablet experiment, Adam Zivo reviews the newest drug protocols adopted by the BC government, documenting the evolution of “safe supply” opioid programs in Canada since 2020. Zivo reports on the concerning lack of evidence behind the protocols, how they undermine recovery, drive diversion to the black market, and ruin the lives of young Canadians.
The new protocols not only avoid any requirement for drug users to first try evidence-based recovery programs before receiving high-potency opioids, but also allow minors to receive them, with no reference to the rights and roles of parents or even a minimum age for safer supply clients.
Of deep concern is also the BC government’s approach of continually increasing access to “safe” opioids despite openly admitting that there is no evidence of proven benefits or safety. The protocols also require that clients be told that their access to free fentanyl and sufentanil will almost certainly be cut off if they are hospitalized, or if they attend withdrawal management or substance use treatment facilities.
Zivo explains: “The prospect of free fentanyl and sufentanil creates powerful incentives to sign away one’s rights to evidence based treatment, so the province is essentially exploiting clients’ addictions so that it can experiment on them without taking legal responsibility for potential harms.”
Zivo adds that “one can reasonably expect that a significant portion of the fentanyl tablets being distributed by the BC government will end up being traded or resold on the black market,” explaining how mass diversion is already a major issue for weaker “safer supply” opioids like hydromorphone.
While addiction experts have been overwhelmingly critical of unsupervised safer supply, Zivo notes that many believe that the solution is not to abolish but to reform the program so that drugs can be provided more responsibly. By receiving safer supply as a temporary intervention, addicted users can transition to recovery-oriented treatments such as opioid agonist therapy (OAT.)
“It would not take much to reshape BC’s safer supply fentanyl and sufentanil programs into something more responsible and genuinely safe,” concludes Zivo. “There is nothing preventing the province from redesigning safer supply as a recovery-oriented intervention.”
To learn more, read the full paper here:

Executive Summary
This past August, British Columbia’s government quietly launched new protocols that allow doctors to prescribe “safer supply” fentanyl tablets and liquid sufentanil. Fentanyl is at least 10 times stronger than hydromorphone and sufentanil, which is derived from fentanyl, is a further 5 to 10 times more potent than its parent drug. While in theory these drugs could save lives if provisioned cautiously, the way the province has chosen to distribute these dangerous opioids is nothing short of reckless.
There is evidence to support the use of opioid agonist therapy (“OAT”) medications, such as methadone, buprenorphine, and slow release oral morphine in addiction treatment, but the government’s new protocols extrapolate OAT-related evidence to support “safer supply” fentanyl even though the two therapies have little in common. In fact, the government’s protocols stress that providing safer supply fentanyl or sufentanil is “not a treatment for opioid use disorder” and that “there is no evidence available supporting this intervention, safety data, or established best practices for when and how to provide it.” It is deeply concerning that the BC government has, over the past several years, significantly increased access to “safe” fentanyl and sufentanil despite openly admitting that there is no evidence showing that these interventions provide any benefits and can be implemented safely.
“Safer supply” programs claim to reduce overdoses and deaths by providing free pharmaceutical-grade drugs as alternatives to potentially tainted illicit substances. While safer supply sounds nice in theory, addiction experts have found that drug users are reselling (“diverting”) a significant portion of their free hydromorphone on the black market to purchase harder substances. This has fuelled new addictions while generating handsome profits for organized crime. Some patients have even been coerced into securing safer supply they didn’t need. Pimps and abusive partners pressure vulnerable women into securing as much hydromorphone as possible for black market resale. Other vulnerable patients, such as the geriatric and disabled, have been robbed of their safer supply outside of pharmacies.
There are other issues with the protocols, too. They require that clients be told that their access to free fentanyl and sufentanil will almost certainly be cut off if they are hospitalized, or if they attend withdrawal management or substance use treatment facilities. This creates powerful disincentives for drug users to seek life-saving health care. Further, none of the safer supply protocols by the British Columbia Centre on Substance Use (BCCSU) discuss the rights and roles of the parents of minors struggling with addiction. It appears that health care providers can give fentanyl and sufentanil to minors regardless of whether parents are aware of, or consent to, this intervention. The protocols do not specify a minimum age for safer supply clients.
It would not take much to reshape BC’s safer supply fentanyl and sufentanil programs into something more responsible and genuinely safe. There is nothing preventing the province from redesigning safer supply as a recovery-oriented intervention. Experts argue that safer supply could be helpful if used as a temporary intervention that helps severely-addicted users make the transition to recovery-oriented treatments, such as OAT.
There is also nothing stopping the province from fixing many of the issues with the safer supply program – including lax safeguards for youth. Any safer supply model must require supervised consumption. It is the absence of this supervision that has enabled the mass diversion of safer supply drugs onto the black market.
Governments have a duty to provide evidence-based treatment to vulnerable citizens and consider collateral harms to others. Rather than fulfil this duty, the BC government is committing to risky and highly experimental interventions that lack an appropriate evidence base.
Adam Zivo is a freelance writer and political analyst best known for his weekly columns in the National Post. He holds a Master of Public Policy from the Munk School of Global Affairs and Public Policy and recently founded the Centre for Responsible Drug Policy, a nonprofit advocacy organization.
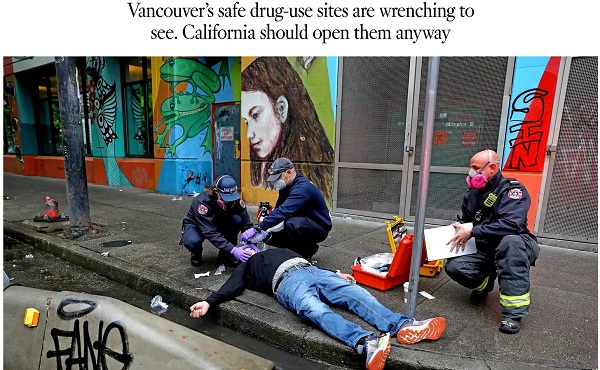
A 2022 Los Angeles Times piece advocates following Vancouver’s model of drug liberalization and treatment. Adam Zivo argues British Columbia’s model has been proven a failure.

By Adam Zivo
Oregon and British Columbia neglected to coerce addicts into treatment.
Ever since Portugal enacted drug decriminalization in 2001, reformers have argued that North America should follow suit. The Portuguese saw precipitous declines in overdoses and blood-borne infections, they argued, so why not adopt their approach?
But when Oregon and British Columbia decriminalized drugs in the early 2020s, the results were so catastrophic that both jurisdictions quickly reversed course. Why? The reason is simple: American and Canadian policymakers failed to grasp what led to the Portuguese model’s initial success.
Contrary to popular belief, Portugal does not allow consequence-free drug use. While the country treats the possession of illicit drugs for personal use as an administrative offense, it nonetheless summons apprehended drug users to “dissuasion” commissions composed of doctors, social workers, and lawyers. These commissions assess a drug user’s health, consumption habits, and socioeconomic circumstances before using arbitrator-like powers to impose appropriate sanctions.
These sanctions depend on the nature of the offense. In less severe cases, users receive warnings, small fines, or compulsory drug education. Severe or repeat offenders, however, can be banned from visiting certain places or people, or even have their property confiscated. Offenders who fail to comply are subject to wage garnishment.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Throughout the process, users are strongly encouraged to seek voluntary drug treatment, with most penalties waived if they accept. In the first few years after decriminalization, Portugal made significant investments into its national addiction and mental-health infrastructure (e.g., methadone clinics) to ensure that it had sufficient capacity to absorb these patients.
This form of decriminalization is far less radical than its North American proponents assume. In effect, Portugal created an alternative justice system that coercively diverts addicts into rehab instead of jail. That users are not criminally charged does not mean they are not held accountable. Further, the country still criminalizes the public consumption and trafficking of illicit drugs.
At first, Portugal’s decriminalization experiment was a clear success. During the 2000s, drug-related HIV infections halved, non-criminal drug seizures surged 500 percent, and the number of addicts in treatment rose by two-thirds. While the data are conflicting on whether overall drug use increased or decreased, it is widely accepted that decriminalization did not, at first, lead to a tidal wave of new addiction cases.
Then things changed. The 2008 global financial crisis destabilized the Portuguese economy and prompted austerity measures that slashed public drug-treatment capacity. Wait times for state-funded rehab ballooned, sometimes reaching a year. Police stopped citing addicts for possession, or even public consumption, believing that the country’s dissuasion commissions had grown dysfunctional. Worse, to cut costs, the government outsourced many of its addiction services to ideological nonprofits that prioritized “harm reduction” services (e.g., distributing clean crack pipes, operating “safe consumption” sites) over nudging users into rehab. These factors gradually transformed the Portuguese system from one focused on recovery to one that enables and normalizes addiction.
This shift accelerated after the Covid-19 pandemic. As crime and public disorder rose, more discarded drug paraphernalia littered the streets. The national overdose rate reached a 12-year high in 2023, and that year, the police chief of the country’s second-largest city told the Washington Post that, anecdotally, the drug problem seemed comparable to what it was before decriminalization. Amid the chaos, some community leaders demanded reform, sparking a debate that continues today.
In North America, however, progressive policymakers seem entirely unaware of these developments and the role that treatment and coercion played in Portugal’s initial success.
In late 2020, Oregon embarked on its own drug decriminalization experiment, known as Measure 110. Though proponents cited Portugal’s success, unlike the European nation, Oregon failed to establish any substantive coercive mechanisms to divert addicts into treatment. The state merely gave drug users a choice between paying a $100 ticket or calling a health hotline. Because the state imposed no penalty for failing to follow through with either option, drug possession effectively became a consequence-free behavior. Police data from 2022, for example, found that 81 percent of ticketed individuals simply ignored their fines.
Additionally, the state failed to invest in treatment capacity and actually defunded existing drug-use-prevention programs to finance Measure 110’s unused support systems, such as the health hotline.
The results were disastrous. Overdose deaths spiked almost 50 percent between 2021 and 2023. Crime and public drug use became so rampant in Portland that state leaders declared a 90-day fentanyl emergency in early 2024. Facing withering public backlash, Oregon ended its decriminalization experiment in the spring of 2024 after almost four years of failure.
The same story played out in British Columbia, which launched a three-year decriminalization pilot project in January 2023. British Columbia, like Oregon, declined to establish dissuasion commissions. Instead, because Canadian policymakers assumed that “destigmatizing” treatment would lead more addicts to pursue it, their new system employed no coercive tools. Drug users caught with fewer than 2.5 grams of illicit substances were simply given a card with local health and social service contacts.
This approach, too, proved calamitous. Open drug use and public disorder exploded throughout the province. Parents complained about the proliferation of discarded syringes on their children’s playgrounds. The public was further scandalized by the discovery that addicts were permitted to smoke fentanyl and meth openly in hospitals, including in shared patient rooms. A 2025 study published in JAMA Health Forum, which compared British Columbia with several other Canadian provinces, found that the decriminalization pilot was associated with a spike in opioid hospitalizations.
The province’s progressive government mostly recriminalized drugs in early 2024, cutting the pilot short by two years. Their motivations were seemingly political, with polling data showing burgeoning support for their conservative rivals.
The lessons here are straightforward. Portugal’s decriminalization worked initially because it did not remove consequences for drug users. It imposed a robust system of non-criminal sanctions to control addicts’ behavior and coerce them into well-funded, highly accessible treatment facilities.
Done right, decriminalization should result in the normalization of rehabilitation—not of drug use. Portugal discovered this 20 years ago and then slowly lost the plot. North American policymakers, on the other hand, never understood the story to begin with.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards


By Alexandra Keeler
Experts say physicians have lost their ‘zeal’ for prescribing safer supply amid growing concerns about diversion and effectiveness
Participation in B.C.’s safer supply program — which offers prescription opioids to people who use drugs — has dropped by nearly 25 per cent over the past two years, according to recent government data.
The B.C. Ministry of Health says updated prescribing guidelines and tighter program oversight are behind the decline.
But addiction experts say the story is more complicated.
“Many of my addiction medicine colleagues have stopped prescribing ‘safe supply’ hydromorphone to their patients because of the high rates of diversion … and lack of efficacy in stabilizing the substance use disorder (sometimes worsening it),” said Dr. Launette Rieb, a clinical associate professor at the University of British Columbia and addiction medicine specialist.
“Many doctors who initially supported ‘safe supply’ no longer provide it but do not wish to talk about it publicly for fear of reprisals,” she said in her email.
Missing data
B.C. has had safer supply programs in place province-wide since 2021.
Participation in its program peaked at nearly 5,200 individuals in March 2023, and then declined to fewer than 3,900 individuals by December 2024. This is the most recent data publicly available, according to B.C.’s health ministry.
In an emailed statement, the ministry attributed the decline to updated clinical guidance and more restrictive prescribing practices “aimed at strengthening the integrity and safety of the program.”
In February, the province updated its safer supply prescribing guidelines to require most patients of the program to consume prescription opioids under the supervision of health-care professionals — a practice known as “witnessed dosing.”
The B.C. government has not released any data on how many patients have been transitioned to witnessed dosing.
The ministry did not address Canadian Affairs’ questions about whether patients are being cut off involuntarily from the program, whether fewer physicians are prescribing or whether barriers to accessing safer supply have increased.
‘Dependence, tolerance, addiction’
Some experts say the decline in safer supply participation is due to physicians being influenced by their peers and public controversy over the program.
Dr. Karen Urbanoski, an associate professor in the Public Health and Social Policy department at the University of Victoria, says peer influence plays a significant role in prescribing practices.
A 2024 study found the uptake of prescribed safer supply in B.C. was closely tied to prescribers’ professional networks.
“These peer influences are apparent for both the uptake of [safer supply] prescribing and its discontinuation — they are likely playing a role here,” Urbanoski said in an email to Canadian Affairs.
Urbanoski also points to the broader environment — including negative media coverage and uncertainty about program funding — as factors behind the decline.
“Media discourse and general politicization of [safer supply] has likely had a ‘cooling effect’ on prescribing,” she said.
Dr. Leonara Regenstreif, a primary care physician and founding member of Addiction Medicine Canada, says many physicians embraced safer supply without fully grasping its clinical risks. Addiction Medicine Canada is an advocacy group representing 23 addiction specialists across Canada.
Regenstreif says physicians too young to have practiced during the peak of OxyContin prescribing were often enthusiastic prescribers of safer supply in the program’s early days. OxyContin is a prescription opioid that helped spark North America’s addiction crisis.
“In my experience, the MD colleagues who have embraced [safer supply] prescribing most zealously … never experienced the trap of writing scripts without knowing what was ahead — dependence, tolerance, addiction, consequences,” her emailed statement says.
Now, many of these physicians are looking for an “exit ramp,” Regenstreif says, as concerns over safer supply diversion and its treatment benefits grow.
Reib, of the UBC, says some of her colleagues in addictions medicine fear speaking out about their concerns with the program.
“Some of my colleagues have had their lives threatened by their patients who have become financially dependent on selling their [hydromorphone],” said Rieb.
The College of Physicians and Surgeons of B.C., which represents physicians in the province, referred Canadian Affairs’ questions about declining program participation to the health ministry and the BC Centre on Substance Use. The centre was unable to provide comment by press time.
Public backlash
The decline in B.C.’s safer supply participation unfolds amid mounting scrutiny of the program and its effectiveness.
Rieb says that the program’s framing — as free, safe and widely available — may run counter to longstanding public health strategies aimed at reducing drug use through pricing and harm awareness.
“Drivers of public use of substances are availability, cost, and perception of harm,” she said. “[Safe supply] is being promoted as safe, free and available for the asking.”
There have been reports of youth gaining access to diverted safer supply opioids and developing addictions to fentanyl as a result. Last September, B.C. father Gregory Sword testified before the House of Commons that his teenage daughter died after accessing diverted safer supply opioids.
B.C.’s recent decision to overhaul its prescribing guidelines followed revelations of a widespread scam by dozens of B.C. pharmacists to exploit the safer supply program to maximize profits.
Experts also note that Canada still lacks the evidence needed to assess the long-term health outcomes of people in safer supply programs. There is currently no research in Canada tracking these long-term health outcomes.
“There is a lack of research to date on retention on [safer supply],” said Urbanoksi.
Rieb agrees. “There are many methodological problems with the recent studies that conclude [the] benefit of pharmaceutical alternatives (‘safe supply’),” she said.
“We need long term studies that look at risks/harms as well as potential benefits.”
Regenstreif says the recent drop in participation may have an unintended upside — encouraging more people with substance use disorders to try what she sees as a more effective treatment: opioid agonist therapy, or OAT. This therapy uses medications like methadone or buprenorphine to reduce withdrawal symptoms and cravings.
“If fewer people are accessing [safer supply] tablets … more people with [opioid use disorder] might accept proper OAT treatment,” she said.
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.

Bystanders Tried To Help Charlotte Stabbing Victim In Her Dying Moments

Charlotte train killer hit with federal murder charge, faces max penalty

French government collapses after budget vote, Le Pen demands elections

Charlie Kirk ASSASSINATED
Mark Carney’s Climate Competitiveness Pitch Falls Flat

Poilievre: “Carney More Irresponsible Than Trudeau” as Housing, Jobs, and Energy Failures Mount

Conservative speaker and celebrity Charlie Kirk shot during Q & A event at Utah Valley University
-
 Crime2 days ago
Crime2 days agoDown the Charlie Kirk Murder Rabbit Hole
-
 Business1 day ago
Business1 day agoIt’s time to finally free the beer
-
 Daily Caller1 day ago
Daily Caller1 day agoTrump Admin To Push UN Overhaul Of ‘Haphazard And Chaotic’ Refugee Policy
-
 Business1 day ago
Business1 day agoCarney Admits Deficit Will Top $61.9 Billion, Unveils New Housing Bureaucracy
-
 Business17 hours ago
Business17 hours agoCarney’s Ethics Test: Opposition MP’s To Challenge Prime Minister’s Financial Ties to China
-
 Artificial Intelligence1 day ago
Artificial Intelligence1 day agoWhat are data centers and why do they matter?
-
 Business14 hours ago
Business14 hours agoAttrition doesn’t go far enough, taxpayers need real cuts
-
 Business13 hours ago
Business13 hours agoCarney government’s housing GST rebate doesn’t go far enough