Business
Nestlé boycott begins as activists target DEI rollbacks


 MxM News
MxM News
Quick Hit:

The latest corporate boycott targeting companies rolling back their diversity, equity, and inclusion (DEI) initiatives is set to begin this week, with Nestlé in the crosshairs. Unlike previous boycotts of Amazon and Target, which focused on avoiding specific retailers, this campaign urges consumers to boycott hundreds of household products from March 21 to March 28. Other major companies, including Walmart, McDonald’s, and General Mills, are also slated for boycotts in the coming months.
Key Details:
-
The Nestlé boycott runs from March 21 to March 28 and encourages avoiding products like Cheerios, KitKat, Purina pet food, and DiGiorno frozen pizza.
-
The movement follows the rollback of DEI policies by several major corporations after President Donald Trump’s call to eliminate DEI at the federal level.
-
Additional boycotts are planned for Walmart, McDonald’s, and Amazon, with an “economic blackout” scheduled for April 18.
Diving Deeper:
The push for boycotts against Nestlé and other corporations stems from a broader activist response to changes in corporate policies following President Donald Trump’s directive to rescind DEI initiatives at the federal level. Many companies, including Amazon, Target, and Walmart, have scaled back or eliminated their DEI programs, prompting backlash from activist groups.
While past boycotts targeted specific retailers—such as avoiding Amazon purchases or skipping Target shopping trips—the Nestlé boycott is structured differently. Consumers are being asked to avoid a wide range of products, from Coffee-Mate creamers to Stouffer’s frozen meals and Perrier sparkling water. This more expansive approach seeks to impact Nestlé’s bottom line across multiple product categories, rather than just limiting consumer spending at a particular store.
This campaign is part of a broader wave of organized economic boycotts. A 40-day boycott of Target was launched last week, intentionally aligning with Lent, a religious period of fasting leading up to Easter. Additionally, Amazon is facing another boycott in May following one that concluded recently.
Nestlé is far from the last target. Activists have mapped out additional boycotts for General Mills (April 21-28), McDonald’s (June 24-30), and an Independence Day boycott on July 4. These efforts appear to be designed for maximum financial pressure, with coordinated economic “blackouts” meant to disrupt revenue streams at key moments throughout the year.
As these corporate boycotts continue, companies may be forced to decide between maintaining DEI initiatives to appease activists or rolling them back to avoid alienating a different segment of their customer base. With President Trump advocating against DEI policies, businesses that comply with his agenda may find themselves the target of an increasingly organized opposition.
Business
Federal funds FROZEN after massive fraud uncovered: Trump cuts off Minnesota child care money

The Trump administration has cut off all federal child care payments to Minnesota, ordering a sweeping audit of the state’s day care system as investigators dig into what officials describe as one of the largest fraud schemes ever tied to social service programs.
“We have frozen all child care payments to the state of Minnesota,” Deputy Health and Human Services Secretary Jim O’Neill wrote Tuesday afternoon, saying the move comes after mounting evidence that taxpayer dollars were being siphoned to sham or non-operational day care centers. The freeze follows a viral investigative video that put a national spotlight on facilities across Minneapolis that were receiving large sums of public money despite appearing closed or barely functioning.
According to Alex Adams, assistant secretary at HHS’s Administration for Children and Families, Minnesota has already received roughly $185 million in federal child care funding this year alone. Those funds, the administration says, will remain locked down until the state can demonstrate that payments are being used lawfully. “Funds will be released only when states prove they are being spent legitimately,” Adams said.
We have frozen all child care payments to the state of Minnesota.
You have probably read the serious allegations that the state of Minnesota has funneled millions of taxpayer dollars to fraudulent daycares across Minnesota over the past decade.
Today we have taken three actions… pic.twitter.com/VYbyf3WGop
— Deputy Secretary Jim O'Neill (@HHS_Jim) December 30, 2025
O’Neill accused Minnesota officials of allowing abuse to fester for years, alleging the state has “funneled millions of taxpayer dollars to fraudulent daycares across Minnesota over the past decade.” To halt further losses, HHS outlined a series of immediate enforcement steps. Going forward, states seeking reimbursement through the Administration for Children and Families will be required to provide receipts or photographic proof documenting how funds are spent.
The department has also formally demanded that Gov. Tim Walz order a “comprehensive audit” of the day care centers flagged by investigators. O’Neill said the review must include attendance records, licensing documents, complaints, investigative files, and inspection reports. He pointed directly to a video published Friday by YouTuber Nick Shirley, who visited multiple Minneapolis-area centers listed as receiving millions in public funds but found locations that appeared closed or inactive.
In addition, HHS has launched a dedicated fraud hotline and email address at childcare.gov to encourage tips from parents, providers, and the public. “We have turned off the money spigot and we are finding the fraud,” O’Neill said, urging anyone with information to come forward.
Federal prosecutors say the scope of the alleged abuse is staggering. Authorities have already confirmed at least $1 billion in fraud tied to Minnesota child care programs, with 92 people charged so far. The U.S. Attorney’s Office has warned the total could ultimately reach as high as $9 billion as investigators continue combing through records.
The funding freeze marks one of the most aggressive crackdowns yet by the Trump administration on state-run social programs accused of lax oversight, sending a clear message that federal dollars will not flow until Minnesota can account for where the money went — and who was cashing in.

From the Frontier Centre for Public Policy
By Conrad Eder
Conrad Eder supports universal health care, but not Canada’s broken version. Despite massive spending, Canadians face brutal wait times. He argues it’s time to allow private options, as other countries do, without abandoning universality.
It’s not about money. It’s about the rules shaping how Canada’s health care system works
Canada’s health care system isn’t failing because it lacks funding or public support. It’s failing because governments have tied it to restrictive rules that block private medical options used in other developed countries to deliver timely care.
Canada spends close to $400 billion a year on health care, placing it among the highest-spending countries in the Organization for Economic Co-operation and Development (OECD). Yet the system continues to struggle with some of the longest waits for care, the fewest doctors per capita and among the lowest numbers of hospital beds in the OECD. This is despite decades of spending increases, including growth of 4.5 per cent in 2023 and 5.7 per cent in 2024, according to estimates from the Canadian Institute for Health Information.
Canadians are losing confidence that government spending is the solution. In fact, many don’t even think it’s making a difference.
And who could blame them? Median health care wait times reached 30 weeks in 2024, up from 27.7 weeks in 2023, which was up from 27.4 weeks in 2022, according to annual surveys by the Fraser Institute.
Nevertheless, politicians continue to tout our universal health care system as a source of national pride and, according to national surveys, 74 per cent of Canadians agree. Yet only 56 per cent are satisfied with it. This gap reveals that while Canadians value universal health care in principle, they are frustrated with it in practice.
But it isn’t universal health care that’s the problem; it’s Canada’s uniquely restrictive version of it. In most provinces, laws restrict physicians from working simultaneously in public and private systems and prohibit private insurance for medically necessary services covered by medicare, constraints that do not exist in most other universal health care systems.
The United Kingdom, France, Germany and the Netherlands all maintain universal health care systems. Like Canada, they guarantee comprehensive insurance coverage for essential health care services. Yet they achieve better access to care than Canada, with patients seeing doctors sooner and benefiting from shorter surgical wait times.
In Germany, there are both public and private hospitals. In France, universal insurance covers procedures whether patients receive them in public hospitals or private clinics. In the Netherlands, all health insurance is private, with companies competing for customers while coverage remains guaranteed. In the United Kingdom, doctors working in public hospitals are allowed to maintain private practices.
All of these countries preserved their commitment to universal health care while allowing private alternatives to expand choice, absorb demand and deliver better access to care for everyone.
Only 26 per cent of Canadians can get same-day or next-day appointments with their family doctor, compared to 54 per cent of Dutch and 47 per cent of English patients. When specialist care is needed, 61 per cent of Canadians wait more than a month, compared to 25 per cent of Germans. For elective surgery, 90 per cent of French patients undergo procedures within four months, compared to 62 per cent of Canadians.
If other nations can deliver timely access to care while preserving universal coverage, so can Canada. Two changes, inspired by our peers, would preserve universal coverage and improve access for all.
First, allow physicians to provide services to patients in both public and private settings. This flexibility incentivizes doctors to maximize the time they spend providing patient care, expanding service capacity and reducing wait times for all patients. Those in the public system benefit from increased physician availability, as private options absorb demand that would otherwise strain public resources.
Second, permit private insurance for medically necessary services. This would allow Canadians to obtain coverage for private medical services, giving patients an affordable way to access health care options that best suit their needs. Private insurance would enable Canadians to customize their health coverage, empowering patients and supporting a more responsive health care system.
These proposals may seem radical to Canadians. They are not. They are standard practice everywhere else. And across the OECD, they coexist with universal health care. They can do the same in Canada.
Alberta has taken an important first step by allowing some physicians to work simultaneously in public and private settings through its new dual-practice model. More Canadian provinces should follow Alberta’s lead and go one step further by removing legislative barriers that prohibit private health insurance for medically necessary services. Private insurance is the natural complement to dual practice, transforming private health care from an exclusive luxury into a viable option for Canadian families.
Canadians take pride in their health care system. That pride should inspire reform, not prevent it. Canada’s health care crisis is real. It’s a crisis of self-imposed constraints preventing our universal system from functioning at the level Canadians deserve.
Policymakers can, and should, preserve universal health care in this country. But maintaining it will require a willingness to learn from those who have built systems that deliver universality and timely access to care, something Canada’s current system does not.
Conrad Eder is a policy analyst at the Frontier Centre for Public Policy.


Remembering Afghanistan and the sacrifices of our military families

How to talk about housing at the holiday dinner table

Largest fraud in US history? Independent Journalist visits numerous daycare centres with no children, revealing massive scam

US Under Secretary of State Slams UK and EU Over Online Speech Regulation, Announces Release of Files on Past Censorship Efforts

Sweden Fixed What Canada Won’t Even Name
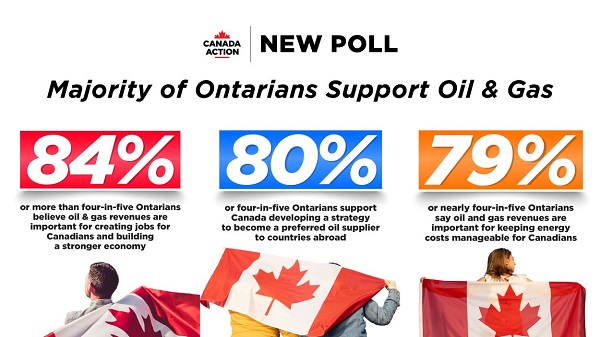
New Poll Shows Ontarians See Oil & Gas as Key to Jobs, Economy, and Trade

Alberta Next Panel calls for less Ottawa—and it could pay off
-
 Alberta2 days ago
Alberta2 days agoThe Canadian Energy Centre’s biggest stories of 2025
-
Business19 hours ago
The Real Reason Canada’s Health Care System Is Failing
-
 Business2 days ago
Business2 days agoOttawa Is Still Dodging The China Interference Threat
-
 Business2 days ago
Business2 days agoResurfaced Video Shows How Somali Scammers Used Day Care Centers To Scam State
-
 Business19 hours ago
Business19 hours agoDark clouds loom over Canada’s economy in 2026
-
 Addictions16 hours ago
Addictions16 hours agoCoffee, Nicotine, and the Politics of Acceptable Addiction
-
Business2 days ago
Minneapolis day care filmed empty suddenly fills with kids
-
 Business2 days ago
Business2 days agoDisclosures reveal Minnesota politician’s husband’s companies surged thousands-fold amid Somali fraud crisis