Health
Leaked footage shows Trump questioning childhood vaccines in phone call with RFK Jr.
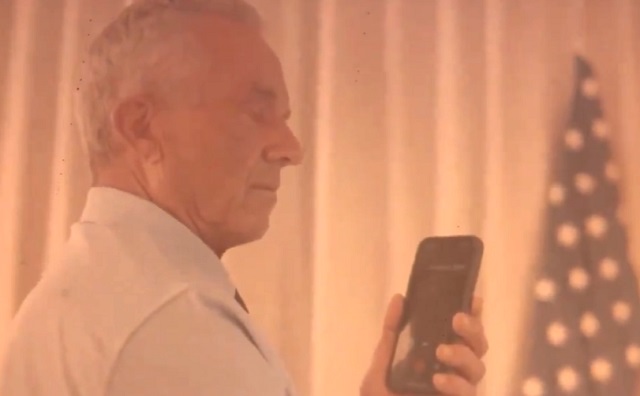

Robert F. Kennedy Jr. speaks with Donald Trump.
From LifeSiteNews

The former president appears to admit that childhood vaccination can lead to injuries during a Sunday phone call with Robert Kennedy Jr., the footage of which was originally leaked by Kennedy’s son.
The son of independent presidential candidate Robert F. Kennedy Jr. recently leaked footage online of his father’s phone call with Donald Trump during which the former president questioned childhood vaccines.
Holy cow. Leaked RFK Jr. call with Trump, talking about vaccines. I hope Trump puts him in charge of shutting down the CDC, FDA corruption.
— Liz Wheeler (@Liz_Wheeler) July 16, 2024
At the beginning of the video clip, Trump can be heard saying, “I agree with you, man. Something’s wrong with that whole system, and it’s the doctors you find. Remember I said, ‘I want to do small doses.’”
“When you feed a baby, Bobby, a vaccination that is like 38 different vaccines, and it looks like it’s meant for a horse, not a, you know, 10-pound or 20-pound baby … and then you see the baby all of a sudden starting to change radically. I’ve seen it so many times,” Trump continued.
“And then you hear that it doesn’t have an impact, right? But you and I talked about that a long time ago,” the former president added.
The leaked footage shows that Trump holds to a stance of skepticism about childhood vaccination that he was publicly known for before the COVID shot rollout under his administration’s Operation Warp Speed. For example, in 2017, Trump was criticized for a statement he made in 2015 linking vaccines to autism: “People that work for me, just the other day, two years old, beautiful child went to have the vaccine and came back and a week later, got a tremendous fever, got very, very sick, now is autistic,” Trump said at the time.
In 2014, Trump tweeted, “Healthy young child goes to doctor, gets pumped with massive shot of many vaccines, doesn’t feel good and changes – AUTISM. Many such cases!”
Kennedy’s son, Robert F. Kennedy III, who posted the footage online early on Tuesday, reportedly said in his X post that he wanted to show Trump’s “real opinion” on vaccination, but has since deleted the clip, according to the BBC.
It is noteworthy that while Trump admits that at least certain doses and kinds of childhood vaccines lead to autism and potentially other health problems, he has consistently defended Operation Warp Speed’s rollout of novel “vaccine” technology in the face of grievances that it has caused many deaths and serious health issues. Since leaving office, he repeatedly promoted the jab as “one of the greatest achievements of mankind.” In January 2023, he dismissed potential safety issues by suggesting that “problems” were in “relatively small numbers.”
It is little discussed, however, that while Operation Warp Speed was technically an initiative of the Trump administration, a significant number of the players involved clashed with the White House, as Politico has revealed. In fact, White House Coronavirus Task Force members were reported to have been excluded from early Warp Speed discussions.
A former White House official involved in the task force says they were “blindsided” by this exclusion, according to Politico. “They wouldn’t brief the task force on it … (just) a private briefing,” the official said at the time.
Politico further revealed that Operation Warp Speed was the brainchild of Health and Human Services Secretary Alex Azar, “who was often at odds with the White House.” His advisory board included NIH director Francis Collins and NIAID director Anthony Fauci, and his plan won the support of White House senior adviser Jared Kushner as well as White House Chief of Staff Mark Meadows.
Kennedy is known for vehemently opposing vaccines, a stance he adopted after the mothers of vaccine-injured children implored him to look into the research linking thimerosal to neurological injuries, including autism. He went on to found Children’s Health Defense, an organization with the stated mission of “ending childhood health epidemics by eliminating toxic exposure,” largely through vaccines.
Trump appears to invite Kennedy to support his presidential campaign during their phone call on Sunday.
“I would love you to do something,” Trump can be heard saying in the video footage. “And I think it’ll be so good for you and so big for you. And we’re going to win.”
Trump also brought up Saturday’s assassination attempt, telling Kennedy that the bullet that pierced his ear “felt like a giant – like the world’s largest mosquito.”
After the video clip of their conversation made the rounds online, Kennedy apologized on Tuesday for its public posting, writing on X, “When President Trump called me, I was taping with an in-house videographer,” he wrote. “I should have ordered the videographer to stop recording immediately. I am mortified that this was posted.”
When President Trump called me I was taping with an in-house videographer. I should have ordered the videographer to stop recording immediately. I am mortified that this was posted. I apologize to the president.
— Robert F. Kennedy Jr (@RobertKennedyJr) July 16, 2024

From LifeSiteNews
Playing fast and loose with the definitions of death for the sake of organ donation must stop.
Another congressional committee is investigating more whistleblowers’ complaints regarding the organ transplantation industry. United States House Ways and Means Committee Chairman Jason Smith and Oversight Subcommittee Chairman David Schweikert are seeking answers from Carolyn Welsh, president and CEO of the New Jersey Organ and Tissue Sharing Network (NJTO), regarding multiple allegations of legal and ethical violations on her watch.
The complaints include the horrific case of a “circulatory death” organ donor who reanimated prior to organ retrieval. Despite the fact that the patient had regained signs of life, NJTO executives actually directed frontline staff to continue the organ recovery process. (Thankfully, hospital personnel at Virtua Our Lady of Lourdes Hospital in Camden, New Jersey, refused this request.) NJTO is also accused of pressuring the families of potential donors by falsely implying the New Jersey Department of Motor Vehicles had registered a consent to donate when that was not known to be the case. NJTO apparently also continued to insist that people were registered donors even after they had removed their consent to donate from their driver’s licenses. The official complaint further states that NJTO allegedly tried to delete evidence pertaining to the committee’s investigation.
Since 1968, when 13 men at Harvard Medical School redefined “desperately injured” people as being dead enough to become organ donors, organ procurement has continued to push the boundaries of life and death in a never-ending quest for more organs. When the first and only multicenter prospective study of brain death discovered in 1972 that a brain death diagnosis did not invariably correlate with a diffusely destroyed brain, principal investigator Dr. Gaetano Molinari pointed out that “brain death” was a prognosis of death, and not death itself. Dr. Molinari wrote:
[D]oes a fatal prognosis permit the physician to pronounce death? It is highly doubtful whether such glib euphemisms as ‘he’s practically dead,’… ‘he can’t survive,’ … ‘he has no chance of recovery anyway,’ will ever be acceptable legally or morally as a pronouncement that death has occurred.
But despite Dr. Molinari’s doubts, history shows this is exactly what has been accepted, and the rising numbers of people who have been taken for organ harvesting while still alive bears this out. Even though “brain dead” TJ Hoover III was still looking around and visibly crying such that two doctors refused to remove his organs, Kentucky Organ Donor Affiliates ordered their staff to find another doctor to perform the procedure. “Circulatory death” donor Misty Hawkins was found to have a beating heart when her breastbone was sawed open for organ procurement. And Larry Black Jr. was rescued from the operating room table just minutes before having his organs removed, and went on to make a full recovery.
Given that we have been stretching the definitions of death for nearly 60 years, is it any wonder that organ procurement personnel appear to be thinking “he’s practically dead,” “he can’t survive,” “he has no chance of recovery anyway” as they push still-living people towards the operating room?
But it’s not just organ procurement teams that are pushing these new definitions of death. Just three weeks after failing in their attempts to broaden the legal definitions of death by revising the Uniform Determination of Death Act (UDDA), the American Academy of Neurology (AAN) published a new brain death guideline that explicitly allows brain death to be declared in the presence of ongoing brain function. Since this obviously does not comply with the UDDA, which requires “the irreversible cessation of all functions of the entire brain including the brain stem,” the AAN has been trying to get around the law by contacting state health departments, medical boards, medical societies, and hospital associations requesting that they acknowledge the AAN’s brain death guideline as the “accepted medical standards” for declaring neurological death.
The AAN has also just published a position statement of additional guidance on brain death discussing how to handle objections to the brain death diagnosis. Even though the AAN’s brain death guideline does not comply with U.S. law and has been proven to be unable to predict whether or not a brain injury is irreversible, the AAN still wants to make the use of their guideline mandatory. If a family’s objection to a brain death diagnosis cannot be overcome, the AAN says that life support may be unilaterally withdrawn – over the family’s objections. The AAN also says that clinicians are professionally obligated to make a brain death determination, and that they should be credentialed to do so according to the standards of the AAN guideline. Laughably, the AAN recommends the Neurocritical Care Society’s brain death determination course, which consists of a one-hour video, followed by unlimited attempts to correctly answer 25 questions, following which a certificate of completion can be had for as little as six dollars.
The Dead Donor Rule is an ethical maxim stating that people must neither be alive when organs are removed nor killed by the process of organ removal. Redefining neurologically injured people as being “brain dead” and redefining people who could still be resuscitated as being dead according to “circulatory death” standards have for too long allowed organ procurement teams to meet the letter of the Dead Donor Rule through sleight of hand. Playing fast and loose with the definitions of death for the sake of organ donation must stop. Patients with a poor prognosis must not be considered “dead enough” to become organ donors. People registering as organ donors must be given fully informed consent as to the risks involved.
Even utilitarian philosopher Dr. Peter Singer has called brain death an ethical choice masquerading as a medical fact. Imposing mandates that force patients and doctors to accept these questionable ethical choices is NOT the best way to establish trust.
Heidi Klessig MD is a retired anesthesiologist and pain management specialist who writes and speaks on the ethics of organ donation and transplantation. She is the author of “The Brain Death Fallacy” and her work may be found at respectforhumanlife.com.
Alberta
Alberta introducing dual practice health care model to increase options and shorten wait times while promising protection for publicly funded services
Enhancing access through dual practice
If passed, Bill 11, the Health Statutes Amendment Act, 2025 (No. 2), would modernize physician participation rules to give doctors flexibility to work in both the public system and private settings. Dual practice would allow physicians to continue providing insured services through the provincial health insurance plan while also delivering private services.
Alberta’s government has looked to proven models in other jurisdictions to guide the development of a model that strengthens access while safeguarding the public system. Dual practice exists in New Brunswick and Quebec and is widely used in countries with top-performing health systems, including Denmark, the Netherlands, United Kingdom, France, Germany, Spain and Australia.
“For years, governments across Canada have tried to fix long wait times by spending more money, yet the problem keeps getting worse. Alberta will not accept the status quo. Dual practice gives us a practical, proven tool that lets surgeons do more without asking taxpayers to pay more. It means shorter waits, better outcomes and a stronger health system for everyone.”
If passed, this dual practice model would be closely monitored to protect Alberta’s public health care system. The government, for example, would ensure that dual practice physicians maintain separate records for the services they provide, so no public funding subsidizes private services.
Bill 11 would include provisions to restrict participation, which could include:
- Mandating that surgeons in dual practice must perform a dedicated number or ratio of surgeries in the public system to be eligible to perform surgeries privately.
- Restricting specialties to public practice if shortages would compromise public care.
- Potentially restricting private practice to evenings, weekends or to underutilized rural sites, as required.
Alberta’s government remains committed to its public health guarantee: No Albertan will ever have to pay out of pocket to see their family doctor or to get the medical treatment they need. These proposed changes comply with the Canada Health Act.
Alberta’s government is also committed to getting Alberta’s dual practice model right and to taking a thoughtful approach to ensure the best path forward. At this time, family medicine providers will not be eligible to be flexible participants within this new model. The priority is to focus on making sure all Albertans have access to a primary care provider. Additionally, surgeries for life-threatening conditions such as cancer and emergency procedures will remain entirely publicly funded with no private option available.
“Albertans are waiting too long for the health care they need, so we are taking bold and decisive action to shorten wait times, increase access and give Albertans more choices over their own health care. At the same time, we will continue building a strong public health system where no one is denied access to the services they need because of an inability to pay.”
If passed, Bill 11 would create new options for doctors and patients. It would expand Alberta’s health system to provide more care by allowing doctors to treat more patients. Each time a patient chooses to pay for care in a private clinic or a clinic operating on evenings and weekends, for example, resources would be freed up so another patient could receive publicly funded care. This proposed new model would also support physician attraction and retention.
“As dual practice enhances flexibility for Albertans, physicians and medical professionals, safeguards will be established and utilized to protect and grow hospital and public health system capacity.”
“Albertans deserve choice and timely access to safe care, whether in a private or public setting. With the creation of the dual practice model, we can extend treatment options to patients while helping hospitals focus their resources on the highest-acuity patients.”
“I believe all options to improve access to health care for Albertans should be on the table. Therefore, the government’s dual practice legislation is a welcome option. Appropriate guardrails must be in place to ensure the spirit of the Canada Health Act is maintained.”
Quick facts
- Physicians would continue to bill the provincial plan for public services and may offer private services separately.
- Physicians may still choose to work entirely in public or entirely in private settings.
Proposed legislation would modernize physician rules, drug coverage, food safety and health cards while improving oversight and administration in Alberta’s health system.
If passed, Bill 11, the Health Statutes Amendment Act, 2025 (No. 2), would amend several pieces of legislation to reflect Alberta’s evolving health needs, strengthen the ability of health care professionals to deliver care and improve accountability and efficiency across the system.
“This legislation represents a new era for health care in Alberta. By putting patients first and supporting providers, we are improving transparency, flexibility and access. With modernized physician rules, stronger drug coverage, enhanced food safety and better health information sharing, Albertans will have world-class care.”
Protecting drug coverage for Albertans
If passed, amendments would improve coordination between public and private drug plans, ensuring taxpayer-funded programs are used efficiently and remain available for those who need them most.
Private plans would become the first payer for individuals who have them, with public programs acting as a safety net. The legislation would also protect older Albertans by ensuring employers cannot reduce or terminate health benefits for employees aged 65 and older who remain actively employed.
“People shouldn’t be punished for getting older – it’s that straightforward. With this legislation, we’re protecting Albertans by ensuring employers can no longer kick folks off their health benefits when they need them most.”
Ensuring consistent billing and remuneration practices
Alberta’s government is also proposing amendments to the Alberta Health Care Insurance Act to ensure health care providers and clinics are not engaging in improper billing practices and making inappropriate claims. The proposed amendments would strengthen accountability and transparency while generating cost savings by introducing penalties for systemic non-compliance.
Strengthening food safety in Alberta
If passed, amendments to the Public Health Act and related regulations would strengthen food safety across all establishments by improving training for staff, increasing transparency of inspection results and giving inspectors new tools for oversight and investigation.
The changes would also update the Food Regulation, Food Retail and Food Services Code, Institutions Regulation and create a new Public Health Investigator Regulation, ensuring consistent standards, better reporting and increased public confidence in Alberta’s food safety system.
“Enhancing food safety in Alberta is an important step to making sure Albertans have the safeguards and protections in place to keep them healthy and well. If passed, these amendments to the Public Health Act will ensure food establishments are following best practices and that enforcement measures are in place to support proper food safety.”
Improving health cards and information sharing
If passed, the legislation would create a new process for health card renewal, prevent card misuse and allow cards to be seized or suspended if tampered with. The changes would also permit information sharing with the ministries of Technology and Innovation and Service Alberta and Red Tape Reduction to support continued efforts to modernize health cards.
Amendments to the Health Information Act would support a more integrated health care system and seamless patient experience to help improve care for Albertans who are accessing the system.
It would also add new authority to enable health foundations to better connect with patients to support innovation and advancement of care in their community in an appropriate manner, in accordance with the requirements set out in regulations.
“Albertans generously support enhancements to health care delivery, innovation and research in their communities each year. We look forward to working with our health partners across the continuum to better communicate with grateful patients. With these changes, we will join other Canadian jurisdictions in connecting patients with health foundations in their community while ensuring the strongest protection of Albertans’ private health data.”
Advancing a new era of health care
If passed, proposed amendments to the Alberta Health Care Insurance Act and the Provincial Health Agencies Act would support operational changes to implement previously announced objectives like transitioning Alberta Health Services to a hospital-based acute care service provider.
The proposed amendments would also result in the repealing of the Hospitals Act, as all hospital governance and operational provisions would be moved into the Provincial Health Agencies Act.
New dual practice model to increase access and choice
The Health Statutes Amendment Act, 2025 (No. 2) includes proposed amendments to the Alberta Health Care Insurance Act that would modernize how physicians participate in Alberta’s publicly funded health insurance plan. The changes would introduce a new dual practice model, giving physicians greater flexibility to provide care in both public and private settings while maintaining safeguards to ensure Albertans continue to have access to publicly funded health services.


Carney fails to undo Trudeau’s devastating energy policies

New airline compensation rules could threaten regional travel and push up ticket prices

EXCLUSIVE: The Nova Scotia RCMP Veterans’ Association IS TARGETING VETERANS with Euthanasia

How Global Organized Crime Took Root In Canada

Roblox to Mandate Facial and ID Verification

Landmark 2025 Study Says Near-Death Experiences Can’t Be Explained Away

I Was Hired To Root Out Bias At NIH. The Nation’s Health Research Agency Is Still Sick
-
 Business1 day ago
Business1 day agoFederal major projects list raises questions
-
 International1 day ago
International1 day agoAmerica first at the national parks: Trump hits Canadians and other foreign visitors with $100 fee
-
Health2 days ago
Organ donation industry’s redefinitions of death threaten living people
-
 Artificial Intelligence2 days ago
Artificial Intelligence2 days agoGoogle denies scanning users’ email and attachments with its AI software
-
 Artificial Intelligence16 hours ago
Artificial Intelligence16 hours agoTrump’s New AI Focused ‘Manhattan Project’ Adds Pressure To Grid
-
 International7 hours ago
International7 hours agoAfghan Ex–CIA Partner Accused in D.C. National Guard Ambush
-
 Alberta5 hours ago
Alberta5 hours agoAlberta and Ottawa ink landmark energy agreement
-
 Indigenous2 days ago
Indigenous2 days agoCanadian mayor promises to ‘vigorously defend’ property owners against aboriginal land grab