Health
Canadian dentists desperate for details on federal dental care plan
News release from Canada’s Provincial and Territorial Dental Associations
Canadian dentists to MPs: We need answers about the Canadian Dental Care Plan
Lack of consultation with provincial and territorial dental associations is worrying
There are only two months left before the Canadian Dental Care Plan (CDCP) becomes available to many more Canadians. Yet more than 25,000 dentists nationwide are in the dark about how the Government of Canada will safeguard access to dental care.
In a letter sent to Members of Parliament (MPs) this week, the presidents of provincial and territorial dental associations across the country asked how the government will:
- Safeguard employer-provided dental plans that two-thirds of Canadians currently have access to?
- Ensure that a strong federal program can be coordinated with existing provincial programs?
- Protect patient choice and maintain the patient-provider relationship?
- Ensure minimal, efficient administration that promotes timely access to care?
- Respect the costs of delivering dental care to maximize provider participation?
- Increase the number of dental assistants and dental hygienists to meet the demands of the CDCP?
Dentists want to champion a CDCP that will respect patients, providers, and taxpayers. The provincial and territorial dental associations are concerned that the CDCP has been compromised by a lack of meaningful consultation with dentists – who will be expected to deliver on the government’s promises.
The CDCP is currently in final planning stages, with a potential rollout in 2024 that will attempt to increase access to uninsured Canadians under 18, people with disabilities, and seniors who have an annual family income of less than $90,000. Dentists believe all Canadians need access to dental care. If not done properly, two-thirds of Canadians who have great employer-provided dental plans could lose their coverage and be forced into a worse plan. Costs would then skyrocket, which means the $13 billion over five years the government set aside would not be enough to sustain the plan.
Let’s take the time to get it right. We can increase access to dental care right now through an expansion of the interim measure already in place – the Canada Dental Benefit. This establishes a fixed dollar amount that a patient can use to be reimbursed for dental-related expenses.
Facts:
- Canada’s provincial and territorial dental associations represent more than 25,000 licensed dentists working in more than 16,000 offices. They treat more than 30 million Canadians every year and employ at least 50,0001 oral health care workers.
- Over 60 per cent of Canadians have a dentist they visit on a regular basis.2
- A recent survey commissioned by Health Canada found that nearly nine out 10 Canadians are satisfied with the Canada Dental Benefit.3
Quotes:
“To succeed, this plan needs to work for both patients and providers, and to work in each province. What we are recommending is based on decades of experience and caring for the oral health needs of the more than 30 million people that come into our dental offices across the country every year.” — Dr. Bruce Yaholnitsky, President, Alberta Dental Association
“Poorly designed programs do not improve access to care, and they leave the most vulnerable people in society behind. This is an historic opportunity, but only if the government gets it right. Dentists have the expertise, experience, and skills to know what it takes to ensure good oral and overall health.” — Dr. Rob Wolanski, President, British Columbia Dental Association
“As dentists we are excited to be a part of this Canadian dental care program, but there are key critical issues that need to be included for this program to be successful.” — Dr. Scott Leckie, President, Manitoba Dental Association
“New Brunswick dentists are already extremely busy with the recent spike in population and the backlog in demand for services related to Covid-19. This program was intended to provide dental care to the 35 per cent of Canadians who are uninsured. It needs to be easy to understand and to administer, and to be fair to all parties, including patients, dental care providers and taxpayers. Canadians need to know what benefits are being provided and which are not, before they arrive at the dental clinic.” — Dr. Joanah Campbell, President, New Brunswick Dental Society
“The new program must be sustainable in terms of funding, and easy to understand and access. It has to be patient-centred and work for everyone.” — Dr. Shane Roberts, President, Newfoundland & Labrador Dental Association
“While the CDCP has the potential to improve the lives of many Canadians, this can only be achieved if it’s done right. To ensure the greatest possible outcome, we must consider all of the moving pieces and take a patient-centred approach.” — Dr. Juli Waterbury, President, Nova Scotia Dental Association
“The CDCP could be a game-changer for Canadians’ access to dental care. But we have one chance to get it right. Here in Ontario, we have seen that dental care programs developed without the input of dentists are doomed to fail. Just look at the Ontario Seniors Dental Care Program, where waiting lists are up to two years long in some areas, and some patients have to travel ridiculously long distances to receive treatment.” — Dr. Brock Nicolucci, President, Ontario Dental Association
“This new program has the potential to improve access to care for many Canadians. It must be sustainable, patient-centred, and easy to access for patients. A poorly designed program will not improve access to care which is something we would like to avoid. We want this to work for Canadians.” — Dr. Derek Thiessen, President, College of Dental Surgeons of Saskatchewan
Health
Last day and last chance to win this dream home! Support the 2025 Red Deer Hospital Lottery before midnight!

Deadline: June 16, 2025
Draw: June 26, 2025
|



|
|
The 2025 Red Deer Hospital Lottery Dream Home, designed by Sorento Custom Homes, continues Sorento’s tradition of award-winning designs. This gorgeous bungalow features 2,824 sq ft of developed living space and showcases a tall, vaulted ceiling.














Located at 128 Emmett Crescent in the neighbourhood of Evergreen, this outstanding home features a screened deck off the dining room, a large family room on the lower level, and of course, a beautiful primary suite. Sorento’s ensuites are always something to behold, and this one features a claw foot tub. There’s an office on the main level, two bedrooms below, and a large fitness room that includes a two-person infrared sauna. Enjoy the convenience of a walk-in pantry, main floor laundry, and chef quality appliances. The design of this unique home is complemented by gorgeous furnishings by Urban Barn.
Our Grand Prize Dream Home package is valued at $1,074,472! You won’t want to miss seeing this outstanding home or your chance to live in it.
50 FOR $75
Make a Difference

Aristotle Foundation
The Canadian Medical Association’s inexplicable stance on pediatric gender medicine

![]()
By Dr. J. Edward Les
The thalidomide saga is particularly instructive: Canada was the last developed country to pull thalidomide from its shelves — three months during which babies continued to be born in this country with absent or deformed limbs
Physicians have a duty to put forward the best possible evidence, not ideology, based treatments
Late last month, the Canadian Medical Association (CMA) announced that it, along with three Alberta doctors, had filed a constitutional challenge to Alberta’s Bill 26 “to protect the relationship between patients, their families and doctors when it comes to making treatment decisions.”
Bill 26, which became law last December, prohibits doctors in the province from prescribing puberty blockers and hormone therapies for those under 16; it also bans doctors from performing gender-reassignment surgeries on minors (those under 18).
The unprecedented CMA action follows its strongly worded response in February 2024 to Alberta’s (at the time) proposed legislation:
“The CMA is deeply concerned about any government proposal that restricts access to evidence-based medical care, including the Alberta government’s proposed restrictions on gender-affirming treatments for pediatric transgender patients.”
But here’s the problem with that statement, and with the CMA’s position: the evidence supporting the “gender affirmation” model of care — which propels minors onto puberty blockers, cross-gender hormones, and in some cases, surgery — is essentially non-existent. That’s why the United Kingdom’s Conservative government, in the aftermath of the exhaustive four-year-long Cass Review, which laid bare the lack of evidence for that model, and which shone a light on the deeply troubling potential for the model’s irreversible harm to youth, initiated a temporary ban on puberty blockers — a ban made permanent last December by the subsequent Labour government. And that’s why other European jurisdictions like Finland and Sweden, after reviews of gender affirming care practices in their countries, have similarly slammed the brakes on the administration of puberty blockers and cross-gender hormones to minors.
It’s not only the Europeans who have raised concerns. The alarm bells are ringing loudly within our own borders: earlier this year, a group at McMaster University, headed by none other than Dr. Gordon Guyatt, one of the founding gurus of the “evidence-based care” construct that rightfully underpins modern medical practice, issued a pair of exhaustive systematic reviews and meta analyses that cast grave doubts on the wisdom of prescribing these drugs to youth.
And yet, the CMA purports to be “deeply concerned about any government proposal that restricts access to evidence-based medical care,” which begs the obvious question: Where, exactly, is the evidence for the benefits of the “gender affirming” model of care? The answer is that it’s scant at best. Worse, the evidence that does exist, points, on balance, to infliction of harm, rather than provision of benefit.
CMA President Joss Reimer, in the group’s announcement of the organization’s legal action, said:
“Medicine is a calling. Doctors pursue it because they are compelled to care for and promote the well-being of patients. When a government bans specific treatments, it interferes with a doctor’s ability to empower patients to choose the best care possible.”
Indeed, we physicians have a sacred duty to pursue the well-being of our patients. But that means that we should be putting forward the best possible treatments based on actual evidence.
When Dr. Reimer states that a government that bans specific treatments is interfering with medical care, she displays a woeful ignorance of medical history. Because doctors don’t always get things right: look to the sad narratives of frontal lobotomies, the oxycontin crisis, thalidomide, to name a few.
The thalidomide saga is particularly instructive: it illustrates what happens when a government drags its heels on necessary action. Canada was the last developed country to pull thalidomide, given to pregnant women for morning sickness, from its shelves, three months after it had been banned everywhere else — three months during which babies continued to be born in this country with absent or deformed limbs, along with other severe anomalies. It’s a shameful chapter in our medical past, but it pales in comparison to the astonishing intransigence our medical leaders have displayed — and continue to display — on the youth gender care file.
A final note (prompted by thalidomide’s history), to speak to a significant quibble I have with Alberta’s Bill 26 legislation: as much as I admire Premier Danielle Smith’s courage in bringing it forward, the law contains a loophole allowing minors already on puberty blockers and cross-gender hormones to continue to take them. Imagine if, after it was removed from the shelves in 1962, government had allowed pregnant women already on the drug to continue to take thalidomide. Would that have made any sense? Of course not. And the same applies to puberty blockers and cross-gender hormones: they should be banned outright for all youth.
That argument is the kind our medical associations should be making — and would be making, if they weren’t so firmly in the grasp, seemingly, of ideologues who have abandoned evidence-based medical care for our youth.
J. Edward Les is a Calgary pediatrician, a senior fellow with the Aristotle Foundation for Public Policy, and co-author of “Teenagers, Children, and Gender Transition Policy: A Comparison of Transgender Medical Policy for Minors in Canada, the United States, and Europe.”

LA Mayor Karen Bass Makes New Demands Of Trump At Monday Night Press Conference
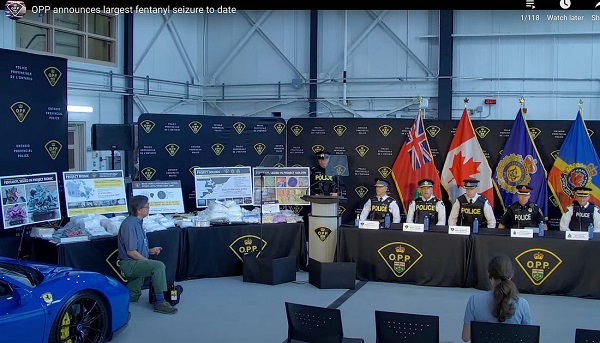
Ontario Police’s Record Fentanyl Bust Suggests Cartel–Iranian–PRC-Supplied Nexus from Ottawa to Hamilton Along Six Nations Corridor
Last day and last chance to win this dream home! Support the 2025 Red Deer Hospital Lottery before midnight!

Mass immigration can cause enormous shifts in local culture, national identity, and community cohesion

RFK Jr. purges CDC vaccine panel, citing decades of ‘skewed science’

Our addiction to dairy supply management is turning Canada into a trade pariah

Oil prices are headed for a hard fall
-
Health2 hours ago
Last day and last chance to win this dream home! Support the 2025 Red Deer Hospital Lottery before midnight!
-
 Business23 hours ago
Business23 hours agoCarney’s European pivot could quietly reshape Canada’s sovereignty
-
Aristotle Foundation6 hours ago
The Canadian Medical Association’s inexplicable stance on pediatric gender medicine
-
 Crime1 day ago
Crime1 day agoManhunt on for suspect in shooting deaths of Minnesota House speaker, husband
-
 Alberta23 hours ago
Alberta23 hours agoAlberta’s grand bargain with Canada includes a new pipeline to Prince Rupert
-
 Bruce Dowbiggin8 hours ago
Bruce Dowbiggin8 hours agoWOKE NBA Stars Seems Natural For CDN Advertisers. Why Won’t They Bite?
-
 conflict9 hours ago
conflict9 hours ago“Evacuate”: Netanyahu Warns Tehran as Israel Expands Strikes on Iran’s Military Command
-
 Energy8 hours ago
Energy8 hours agoCould the G7 Summit in Alberta be a historic moment for Canadian energy?