Addictions
BC NDP, Conservatives’ drug policies converge in close election

From Break The Needle

By Alexandra Keeler
The BC NDP and Conservatives have both pledged to introduce involuntary care for addicts as they contend for voter support on unpopular issue
Gregory Sword has been advocating for British Columbia to permit involuntary care of individuals struggling with addiction ever since losing his 14-year-old daughter to an overdose two years ago.
Now, he looks likely to get his wish — regardless of which party wins the provincial election on Oct. 19.
On Sept. 15, NDP Premier David Eby announced plans to expand involuntary care for “people with addiction challenges, brain injuries, and mental-health issues.” The announcement follows a similar pledge by BC Conservative Leader John Rustad, who on Sept. 11 promised to introduce involuntary care for adults and minors.
The move suggests the BC NDP may be recalibrating its drug policies in response to polling data and competitive pressure from the BC Conservative Party, which has seen its electoral prospects bolstered by the collapse of the centre-right BC United Party.
The BC Conservatives and BC NDP are tied in the polls, at 44 and 43 per cent respectively, according to an Aug. 30 Angus Reid survey. More than two-thirds of respondents said they thought the province was on the “wrong track” in dealing with the opioid crisis. A Sept. 5 Angus Reid poll had similar findings, with 74 per cent of respondents rating the NDP’s handling of the drug crisis as “poor” or “very poor.”
‘A new phase’
B.C. saw a six per cent drop in opioid-related deaths in early 2024 compared to 2023. But the province continues to account for 32 per cent of all drug-related deaths in Canada, despite having just 13 per cent of its population.
In Sunday’s announcement, Eby referred to the introduction of involuntary care as “the beginning of a new phase of our response to the addiction crisis … We are taking action to get them the care they need to keep them safe, and in doing so, keep our communities safe, too.”
Rustad criticized the announcement, citing policy inconsistency. “For years, the NDP ignored the calls for involuntary care, leaving families helpless and those suffering on the streets,” he said in a media release.
“Now, after our party clearly outlined a plan to bring compassion and accountability to addiction treatment, Eby is suddenly pretending to be on board.”
However, Eby first proposed introducing involuntary care in August 2022 during his leadership race. The NDP’s move also partially follows a recommendation of Dr. Daniel Vigo, B.C.’s first chief scientific adviser for psychiatry, who was appointed to that role in June 2024.
Sword, who tried to get his daughter help, believes B.C.’s youth treatment framework — which currently requires minors to consent to addictions treatment — ultimately contributed to his daughter’s death.
“This is how screwed up B.C. is: If I harm my child, beat my child, get my child drugs — she can be taken away from me and get the help that she needs,” he told Canadian Affairs in August. “But if she’s doing it to herself, it’s okay.”
Bold harm-reduction measures
The “new phase” in the NDP’s response to the drug crisis reflects a shift from a prior focus on bold harm-reduction measures — some of which have been followed by reversals.
Since taking office in 2017, the NDP has doubled the number of supervised consumption sites in B.C., from three to six (five are currently operational). And it has expanded the number of overdose prevention sites — which generally offer fewer services than supervised consumption sites — from 20 to 44.
In 2020, the NDP government introduced prescribed alternative supply programs — previously known as “safer supply” — which enable users to receive prescribed opioids as an alternative to illicit street drugs.
In January 2023, the province began a three-year, trial decriminalization project that permitted British Columbians to possess small amounts of otherwise illicit drugs such as heroin, fentanyl, and methamphetamine. B.C. was the first — and so far only — province to decriminalize hard drugs.
But in April, the province partially reversed course, obtaining Ottawa’s approval to recriminalize the use of hard drugs in public spaces.
In October 2023, Provincial Health Officer Dr. Bonnie Henry ordered that vending machines be installed outside hospital emergency departments on Vancouver Island to dispense free drug consumption supplies. On Sept. 12, Eby ordered a review of this initiative, leading to a suspension of the machines until the review is complete.
The BC NDP party did not respond to multiple requests for comment for this story by press time.
Subscribe for free to get BTN’s latest news and analysis, or donate to our journalism fund.
Conservative alternatives
The BC Conservatives have positioned themselves as champions of “common sense” solutions to the drug crisis. In response to requests for comment for this story, the BC Conservatives referred Canadian Affairs to its Sept. 15 media release.
Rustad has said that safe supply programs and decriminalization have been policy failures. The party’s platform pledges to “end heroin hand-outs” and to “reverse decriminalization of hard drugs.” Rustad has also criticized harm-reduction vending machines, accusing Eby of “encouraging the proliferation of hard drug use across the province.”
“I know that they [BC Conservatives] are very much on board for more recovery models versus drug decriminalization,” said William Yoachim, a Nanaimo city council member and member of the Snuneymuxw First Nation. Yoachim says he is cautiously optimistic there could be a significant policy change under a new government.
“My only concern with what a Conservative government’s approach would be is their leader. I’m not sure how committed he would be towards the Indigenous recovery.”
The BC Conservatives have said they would develop a new public health strategy focused on addressing “the root causes of drug addiction that prioritizes treatment and not free drugs.”
They have also proposed stricter penalties for drug smuggling and enhanced border security.
Before suspending its electoral campaign, the BC United Party had pledged to introduce free, accessible mental health and addiction services and longer treatment stays. It had also advocated for people with lived experience of addiction, homelessness and mental illness to be involved in designing recovery-oriented housing.
It remains unclear whether the BC Conservatives — which now includes some former BC United candidates — will adopt any of these policies.
Sarah Blyth, a frontline harm-reduction worker with the Vancouver Overdose Prevention Society, says she is frustrated by how polarizing the issue of drug policy has become.
“People are becoming really dogmatic on either side of it,” she said. “We should be looking at each other to see what unique, creative approaches we’re taking … and figure out what’s working where, and do our best.”
Blyth says she plans to keep her head down through this election. “Let them fight it out.”
“Let this be over, and then let’s get back to work.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle. Our content is always free – but if you want to help us commission more high-quality journalism, consider getting a voluntary paid subscription.
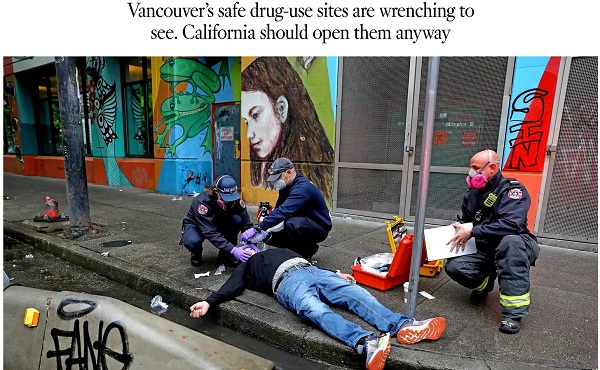
A 2022 Los Angeles Times piece advocates following Vancouver’s model of drug liberalization and treatment. Adam Zivo argues British Columbia’s model has been proven a failure.

By Adam Zivo
Oregon and British Columbia neglected to coerce addicts into treatment.
Ever since Portugal enacted drug decriminalization in 2001, reformers have argued that North America should follow suit. The Portuguese saw precipitous declines in overdoses and blood-borne infections, they argued, so why not adopt their approach?
But when Oregon and British Columbia decriminalized drugs in the early 2020s, the results were so catastrophic that both jurisdictions quickly reversed course. Why? The reason is simple: American and Canadian policymakers failed to grasp what led to the Portuguese model’s initial success.
Contrary to popular belief, Portugal does not allow consequence-free drug use. While the country treats the possession of illicit drugs for personal use as an administrative offense, it nonetheless summons apprehended drug users to “dissuasion” commissions composed of doctors, social workers, and lawyers. These commissions assess a drug user’s health, consumption habits, and socioeconomic circumstances before using arbitrator-like powers to impose appropriate sanctions.
These sanctions depend on the nature of the offense. In less severe cases, users receive warnings, small fines, or compulsory drug education. Severe or repeat offenders, however, can be banned from visiting certain places or people, or even have their property confiscated. Offenders who fail to comply are subject to wage garnishment.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Throughout the process, users are strongly encouraged to seek voluntary drug treatment, with most penalties waived if they accept. In the first few years after decriminalization, Portugal made significant investments into its national addiction and mental-health infrastructure (e.g., methadone clinics) to ensure that it had sufficient capacity to absorb these patients.
This form of decriminalization is far less radical than its North American proponents assume. In effect, Portugal created an alternative justice system that coercively diverts addicts into rehab instead of jail. That users are not criminally charged does not mean they are not held accountable. Further, the country still criminalizes the public consumption and trafficking of illicit drugs.
At first, Portugal’s decriminalization experiment was a clear success. During the 2000s, drug-related HIV infections halved, non-criminal drug seizures surged 500 percent, and the number of addicts in treatment rose by two-thirds. While the data are conflicting on whether overall drug use increased or decreased, it is widely accepted that decriminalization did not, at first, lead to a tidal wave of new addiction cases.
Then things changed. The 2008 global financial crisis destabilized the Portuguese economy and prompted austerity measures that slashed public drug-treatment capacity. Wait times for state-funded rehab ballooned, sometimes reaching a year. Police stopped citing addicts for possession, or even public consumption, believing that the country’s dissuasion commissions had grown dysfunctional. Worse, to cut costs, the government outsourced many of its addiction services to ideological nonprofits that prioritized “harm reduction” services (e.g., distributing clean crack pipes, operating “safe consumption” sites) over nudging users into rehab. These factors gradually transformed the Portuguese system from one focused on recovery to one that enables and normalizes addiction.
This shift accelerated after the Covid-19 pandemic. As crime and public disorder rose, more discarded drug paraphernalia littered the streets. The national overdose rate reached a 12-year high in 2023, and that year, the police chief of the country’s second-largest city told the Washington Post that, anecdotally, the drug problem seemed comparable to what it was before decriminalization. Amid the chaos, some community leaders demanded reform, sparking a debate that continues today.
In North America, however, progressive policymakers seem entirely unaware of these developments and the role that treatment and coercion played in Portugal’s initial success.
In late 2020, Oregon embarked on its own drug decriminalization experiment, known as Measure 110. Though proponents cited Portugal’s success, unlike the European nation, Oregon failed to establish any substantive coercive mechanisms to divert addicts into treatment. The state merely gave drug users a choice between paying a $100 ticket or calling a health hotline. Because the state imposed no penalty for failing to follow through with either option, drug possession effectively became a consequence-free behavior. Police data from 2022, for example, found that 81 percent of ticketed individuals simply ignored their fines.
Additionally, the state failed to invest in treatment capacity and actually defunded existing drug-use-prevention programs to finance Measure 110’s unused support systems, such as the health hotline.
The results were disastrous. Overdose deaths spiked almost 50 percent between 2021 and 2023. Crime and public drug use became so rampant in Portland that state leaders declared a 90-day fentanyl emergency in early 2024. Facing withering public backlash, Oregon ended its decriminalization experiment in the spring of 2024 after almost four years of failure.
The same story played out in British Columbia, which launched a three-year decriminalization pilot project in January 2023. British Columbia, like Oregon, declined to establish dissuasion commissions. Instead, because Canadian policymakers assumed that “destigmatizing” treatment would lead more addicts to pursue it, their new system employed no coercive tools. Drug users caught with fewer than 2.5 grams of illicit substances were simply given a card with local health and social service contacts.
This approach, too, proved calamitous. Open drug use and public disorder exploded throughout the province. Parents complained about the proliferation of discarded syringes on their children’s playgrounds. The public was further scandalized by the discovery that addicts were permitted to smoke fentanyl and meth openly in hospitals, including in shared patient rooms. A 2025 study published in JAMA Health Forum, which compared British Columbia with several other Canadian provinces, found that the decriminalization pilot was associated with a spike in opioid hospitalizations.
The province’s progressive government mostly recriminalized drugs in early 2024, cutting the pilot short by two years. Their motivations were seemingly political, with polling data showing burgeoning support for their conservative rivals.
The lessons here are straightforward. Portugal’s decriminalization worked initially because it did not remove consequences for drug users. It imposed a robust system of non-criminal sanctions to control addicts’ behavior and coerce them into well-funded, highly accessible treatment facilities.
Done right, decriminalization should result in the normalization of rehabilitation—not of drug use. Portugal discovered this 20 years ago and then slowly lost the plot. North American policymakers, on the other hand, never understood the story to begin with.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards


By Alexandra Keeler
Experts say physicians have lost their ‘zeal’ for prescribing safer supply amid growing concerns about diversion and effectiveness
Participation in B.C.’s safer supply program — which offers prescription opioids to people who use drugs — has dropped by nearly 25 per cent over the past two years, according to recent government data.
The B.C. Ministry of Health says updated prescribing guidelines and tighter program oversight are behind the decline.
But addiction experts say the story is more complicated.
“Many of my addiction medicine colleagues have stopped prescribing ‘safe supply’ hydromorphone to their patients because of the high rates of diversion … and lack of efficacy in stabilizing the substance use disorder (sometimes worsening it),” said Dr. Launette Rieb, a clinical associate professor at the University of British Columbia and addiction medicine specialist.
“Many doctors who initially supported ‘safe supply’ no longer provide it but do not wish to talk about it publicly for fear of reprisals,” she said in her email.
Missing data
B.C. has had safer supply programs in place province-wide since 2021.
Participation in its program peaked at nearly 5,200 individuals in March 2023, and then declined to fewer than 3,900 individuals by December 2024. This is the most recent data publicly available, according to B.C.’s health ministry.
In an emailed statement, the ministry attributed the decline to updated clinical guidance and more restrictive prescribing practices “aimed at strengthening the integrity and safety of the program.”
In February, the province updated its safer supply prescribing guidelines to require most patients of the program to consume prescription opioids under the supervision of health-care professionals — a practice known as “witnessed dosing.”
The B.C. government has not released any data on how many patients have been transitioned to witnessed dosing.
The ministry did not address Canadian Affairs’ questions about whether patients are being cut off involuntarily from the program, whether fewer physicians are prescribing or whether barriers to accessing safer supply have increased.
‘Dependence, tolerance, addiction’
Some experts say the decline in safer supply participation is due to physicians being influenced by their peers and public controversy over the program.
Dr. Karen Urbanoski, an associate professor in the Public Health and Social Policy department at the University of Victoria, says peer influence plays a significant role in prescribing practices.
A 2024 study found the uptake of prescribed safer supply in B.C. was closely tied to prescribers’ professional networks.
“These peer influences are apparent for both the uptake of [safer supply] prescribing and its discontinuation — they are likely playing a role here,” Urbanoski said in an email to Canadian Affairs.
Urbanoski also points to the broader environment — including negative media coverage and uncertainty about program funding — as factors behind the decline.
“Media discourse and general politicization of [safer supply] has likely had a ‘cooling effect’ on prescribing,” she said.
Dr. Leonara Regenstreif, a primary care physician and founding member of Addiction Medicine Canada, says many physicians embraced safer supply without fully grasping its clinical risks. Addiction Medicine Canada is an advocacy group representing 23 addiction specialists across Canada.
Regenstreif says physicians too young to have practiced during the peak of OxyContin prescribing were often enthusiastic prescribers of safer supply in the program’s early days. OxyContin is a prescription opioid that helped spark North America’s addiction crisis.
“In my experience, the MD colleagues who have embraced [safer supply] prescribing most zealously … never experienced the trap of writing scripts without knowing what was ahead — dependence, tolerance, addiction, consequences,” her emailed statement says.
Now, many of these physicians are looking for an “exit ramp,” Regenstreif says, as concerns over safer supply diversion and its treatment benefits grow.
Reib, of the UBC, says some of her colleagues in addictions medicine fear speaking out about their concerns with the program.
“Some of my colleagues have had their lives threatened by their patients who have become financially dependent on selling their [hydromorphone],” said Rieb.
The College of Physicians and Surgeons of B.C., which represents physicians in the province, referred Canadian Affairs’ questions about declining program participation to the health ministry and the BC Centre on Substance Use. The centre was unable to provide comment by press time.
Public backlash
The decline in B.C.’s safer supply participation unfolds amid mounting scrutiny of the program and its effectiveness.
Rieb says that the program’s framing — as free, safe and widely available — may run counter to longstanding public health strategies aimed at reducing drug use through pricing and harm awareness.
“Drivers of public use of substances are availability, cost, and perception of harm,” she said. “[Safe supply] is being promoted as safe, free and available for the asking.”
There have been reports of youth gaining access to diverted safer supply opioids and developing addictions to fentanyl as a result. Last September, B.C. father Gregory Sword testified before the House of Commons that his teenage daughter died after accessing diverted safer supply opioids.
B.C.’s recent decision to overhaul its prescribing guidelines followed revelations of a widespread scam by dozens of B.C. pharmacists to exploit the safer supply program to maximize profits.
Experts also note that Canada still lacks the evidence needed to assess the long-term health outcomes of people in safer supply programs. There is currently no research in Canada tracking these long-term health outcomes.
“There is a lack of research to date on retention on [safer supply],” said Urbanoksi.
Rieb agrees. “There are many methodological problems with the recent studies that conclude [the] benefit of pharmaceutical alternatives (‘safe supply’),” she said.
“We need long term studies that look at risks/harms as well as potential benefits.”
Regenstreif says the recent drop in participation may have an unintended upside — encouraging more people with substance use disorders to try what she sees as a more effective treatment: opioid agonist therapy, or OAT. This therapy uses medications like methadone or buprenorphine to reduce withdrawal symptoms and cravings.
“If fewer people are accessing [safer supply] tablets … more people with [opioid use disorder] might accept proper OAT treatment,” she said.
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.

Charlotte train killer hit with federal murder charge, faces max penalty

Trump confronts mainstream media with Chicago’s bloody receipts

Bystanders Tried To Help Charlotte Stabbing Victim In Her Dying Moments

French government collapses after budget vote, Le Pen demands elections

Carney engaging in Orwellian doublethink with federal budget rhetoric

Charlie Kirk ASSASSINATED

Ken Dryden: Hockey’s Diogenes. He Called Them As He Saw Them
-
 Crime2 days ago
Crime2 days ago“Hey fascist! Catch!”: Authorities confirm writing on alleged Kirk killer’s bullet casings
-
 espionage20 hours ago
espionage20 hours agoInside Xi’s Fifth Column: How Beijing Uses Gangsters to Wage Political Warfare in Taiwan — and the West
-
 J.D. Tuccille2 days ago
J.D. Tuccille2 days agoAfter Charlie Kirk’s Murder, Politicians Can Back Away From the Brink, or Make Matters Worse
-
 International2 days ago
International2 days agoCharlie Kirk Shooting Suspect Revealed: Here’s What His Ammunition Said
-
 Daily Caller1 day ago
Daily Caller1 day ago‘You Have No Idea What You Have Unleashed’: Erika Kirk Addresses Supporters For First Time Since Kirk’s Assassination
-
 Health2 days ago
Health2 days agoCanadians left with no choice but euthanasia when care is denied
-
 Censorship Industrial Complex19 hours ago
Censorship Industrial Complex19 hours agoDecision expected soon in case that challenges Alberta’s “safe spaces” law
-
 COVID-1912 hours ago
COVID-1912 hours agoWhy FDA Was Right To Say No To COVID-19 Vaccines For Healthy Kids