COVID-19
So. Who gets the ventilators?

This is posted with permission from the author, Neil MacDonald. It is originally posted at neilmacdonald.me
So. Who gets the ventilators?
I wish Sophie Gregoire Trudeau good health, and a complete recovery in her quarantine. The same for the lovely Margaret Trudeau, if she comes down with COVID-19. Both women were at the same speaking engagement in London; presumably, that is where Madame Gregoire Trudeau contracted the virus.
If, heaven forfend, either woman develops the sort of severe respiratory difficulties that have killed other COVID-19 patients, I hope they will both have access to peerless medical care, and a ventilator. Actually, I am certain they will.
One is the prime minister’s wife, the other his mother. Privilege has its privileges.
At the same time – and here comes the kicker – I am not at all certain that, if I or any of my aged relatives come down with the disease in the uncertain and increasingly terrifying weeks to come, there will be ventilators for us. And as one American epidemiologist put it recently, the alternative to ventilation for someone with extreme respiratory symptoms is death. As a despairing Italian physician put it on social media from the horrors of his triage centre in Bergamo: “Every ventilator becomes like gold.”
Here is the math: Health Minister Patty Hajdu says between 30 and 70 per cent of Canadians will likely be infected. The mortality rate of COVID-19 is between two and three per cent. Assuming the optimistic end of Hajdu’s estimate, and the optimistic end of the mortality rate, we are still talking about 225,000 people dying, and, as the despairing Italian physician says, the diagnosis is always the same: Bilateral interstitial pneumonia. Meaning those patients’ lungs are so badly compromised the only thing that has a chance of saving them is a ventilator, or mechanical breathing apparatus. It alone can infuse the lungs with enough oxygen to maintain life.
Now: We are told Canada has about 5,000 ventilators. That’s one ventilator for every 45 of those dying patients. Unless Canada somehow acquires a lot more of the machines, and the entire world is now chasing them, there will be rationing. That is what has been happening in Italy. Doctors there have been given the ghastly job of deciding who receives ventilation, and who is sent home to meet their fate.
Now, let’s add something else to the equation: In Canada, the law prevents citizens from paying for core medical care, which a ventilator surely is. In principle, ventilators will be rationed, well, rationally.
But that’s not how the system really works.
In Canada, influence and power get you to the front of the line. Does anyone really believe that cabinet ministers or premiers or captains of industry or very senior government officials sit in waiting rooms, or have a hard time finding a family doctor? Or that those of us with professional or family connections aren’t treated as privileged entities?
So the big question – the crucial, life-or-death question as this virus tears through the population – will very quickly be this: who gets the ventilators?
No doubt, an attempt will be made to lay down a set of objective criteria. They probably already exist. It makes sense to ventilate patients who stand the best chance of surviving. A physician friend in Italy unilaterally decided to send very old people home, along with anyone whose health was already severely compromised by previous morbidities.
But imagine the pressure on a Canadian doctor, or hospital dependent on government funding, when the aged relative of a very powerful politician needs ventilation. Or a very rich person who has donated generously to the hospital. Or the mother or father of a person whose role in the economy is considered so crucial that he or she must not be distracted by familial worries.
Jane Philpott, Justin Trudeau’s first health minister, once declared that not being able to buy your way to the front of the line is a “core Canadian value.” The remark was rather gormless, I thought at the time, given the reality of the system. Doctor friends of mine thought it was hysterical.
But the big test is coming. The public deserves to know precisely how lifesaving care will be allocated. The public has a right to transparent fairness.
My guess: fairness and objective allocation of resources will slam into the wall of privilege. We shall see. We shall also see how intrepid the media is on this subject. So far, it hasn’t been.
From neilmacdonald.me

Neil Macdonald spent 43 years reporting on politics, wars, elections, revolutions, booms, crashes, coups, and the struggles of ordinary human beings in the unforgiving, bewildering rush of history.
He worked as an editor and reporter in three newspapers before moving to CBC News, for which he covered Quebec before moving to Parliament Hill, then abroad as a foreign correspondent in the Middle East and Washington, DC., and finally as the CBC’s opinion columnist.
He has stood in Iraq watching missiles strike, in Bethlehem watching people welcome the new millennium, in Jerusalem watching an intifada erupt, and in Chicago watching Barack Obama accept the American presidency. He followed the Pope through the Holy Land, tracked down Hitler’s last general in Europe, covered the triumphant arrival and subsequent humiliation of Jean-Bertrand Aristide in Haiti, revealed the plotters who killed Rafiq Hariri in Beirut, and documented the financial horrors unleashed on America’s cities by Wall Street.
He speaks French, having grown up in Quebec, reasonably good English, and sufficient Arabic. He lives in Ottawa.
Learning at home? Here’s a list of links to take you on a “Virtual Field Trip”

From LifeSite News
The government said that it has decided to stop ‘waste’ by not making the shots free starting this fall.
Beginning this fall, COVID shots in the province will have to be pre-ordered at the full price, about $110, to receive them. (This will roll out in four ‘phases’. In the first phases COVID shots will still be free for those with pre-existing medical conditions, people on social programs, and seniors.)
The UCP government in a press release late last week noted due to new “federal COVID-19 vaccine procurement” rules, which place provinces and territories as being responsible for purchasing the jabs for residents, it has decided to stop “waste” by not making the jab free anymore.
“Now that Alberta’s government is responsible for procuring vaccines, it’s important to better determine how many vaccines are needed to support efforts to minimize waste and control costs,” the government stated.
“This new approach will ensure Alberta’s government is able to better determine its overall COVID-19 vaccine needs in the coming years, preventing significant waste.”
The New Democratic Party (NDP) took issue with the move to stop giving out the COVID shots for free, claiming it was “cruel” and would place a “financial burden” on people wanting the shots.
NDP health critic Sarah Hoffman claimed the move by the UCP is health “privatization” and the government should promote the abortion-tainted shots instead.
The UCP said that in 2023-2024, about 54 percent of the COVID shots were wasted, with Health Minister Adriana LaGrange saying, “In previous years, we’ve seen significant vaccine wastage.”
“By shifting to a targeted approach and introducing pre-ordering, we aim to better align supply with demand – ensuring we remain fiscally responsible while continuing to protect those at highest risk,” she said.
The UCP government said that the COVID shots for the fall will be rolled out in four phases, with those deemed “high risk” getting it for free until then. However, residents who want the shots this fall “will be required to pay the full cost of the vaccine, the government says.”
The jabs will only be available through public health clinics, with pharmacies no longer giving them out.
The UCP also noted that is change in policy comes as a result of the Federal Drug Administration in the United States recommending the jabs be stopped for young children and pregnant women.
The opposite happened in Canada, with the nation’s National Advisory Committee on Immunization (NACI) continuing to say that pregnant women should still regularly get COVID shots as part of their regular vaccine schedule.
The change in COVID jab policy is no surprise given Smith’s opposition to mandatory shots.
As reported by LifeSiteNews, early this year, Smith’s UCP government said it would consider halting COVID vaccines for healthy children.
Smith’s reasoning was in response to the Alberta COVID-19 Pandemic Data Review Task Force’s “COVID Pandemic Response” 269-page final report. The report was commissioned by Smith last year, giving the task force a sweeping mandate to investigate her predecessor’s COVID-era mandates and policies.
The task force’s final report recommended halting “the use of COVID-19 vaccines without full disclosure of their potential risks” as well as outright ending their use “for healthy children and teenagers as other jurisdictions have done,” mentioning countries like “Denmark, Sweden, Norway, Finland, and the U.K.”
The mRNA shots have also been linked to a multitude of negative and often severe side effects in children and all have connections to cell lines derived from aborted babies.
Many Canadian doctors who spoke out against COVID mandates and the experimental mRNA injections were censured by their medical boards.
LifeSiteNews has published an extensive amount of research on the dangers of the experimental COVID mRNA jabs that include heart damage and blood clots.

From LifeSiteNews
With lockdowns, mass vaccination campaigns, and social distancing still on the table from the last around, it appears that AI and Machine Learning will play a much bigger role in the next.
DARPA is getting into the business of simulating disease outbreaks, including modeling interventions such as mass vaccination campaigns, lockdowns, and communication strategies.
At the end of May, the U.S. Defense Advanced Research Projects Agency (DARPA) put out a Request for Information (RFI) seeking information regarding “state-of-the-art capabilities in the simulation of disease outbreaks.”
The Pentagon’s research and development funding arm wants to hear from academic, industry, commercial, and startup communities on how to develop “advanced capabilities that drive technical innovation and identify critical gaps in bio-surveillance, diagnostics, and medical countermeasures” in order to “improve preparedness for future public health emergencies.”
Dr. @P_McCulloughMD: "This Is a Military Operation"
"The military said in 2012, 'We will end pandemics in 60 days using messenger RNA.' That's long before Moderna and Pfizer were even in the game. … They are profiting from this, but they didn't drive it." pic.twitter.com/71jAV5wfG0
— The Vigilant Fox 🦊 (@VigilantFox) March 12, 2023
As if masks, social distancing, lockdowns, and vaccination mandates under the unscientific guise of slowing the spread and preventing the transmission of COVID weren’t harmful enough, the U.S. military wants to model the effects of these exact same countermeasures for future outbreaks.
The RFI also asks participants “Fatality Rate & Immune Status: How are fatality rates and varying levels of population immunity (natural or vaccine-induced) incorporated into your simulations?“
Does “natural or vaccine-induced” relate to “population immunity” or “fatality rates” or both?
Moving on, the RFI gets into modeling lockdowns, social distancing, and mass vaccination campaigns, along with communication strategies:
Intervention Strategies: Detail the range of intervention strategies that can be modeled, including (but not limited to) vaccination campaigns, social distancing measures, quarantine protocols, treatments, and public health communication strategies. Specifically, describe the ability to model early intervention and its impact on outbreak trajectory.
The fact that DARPA wants to model these so-called intervention strategies just after the entire world experienced them suggests that these exact same measures will most likely be used again in the future:
“We are committed to developing advanced modeling capabilities to optimize response strategies and inform the next generation of (bio)technology innovations to protect the population from biological threats. We are particularly focused on understanding the complex interplay of factors that drive outbreak spread and evaluating the effectiveness of potential interventions.” — DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025.
“Identification of optimal timelines and capabilities to detect, identify, attribute, and respond to disease outbreaks, including but not limited to biosensor density deployment achieving optimal detection timelines, are of interest.” — DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025.
With lockdowns, mass vaccination campaigns, and social distancing still on the table from the last around, it appears that AI and Machine Learning will play a much bigger role in the next.
For future innovation, the DARPA RFI asks applicants to: “Please describe any novel technical approaches – or applications of diverse technical fields (e.g., machine learning, artificial intelligence, complex systems theory, behavioral science) – that you believe would significantly enhance the state-of-the-art capabilities in this field or simulation of biological systems wholistically.”
Instead of putting a Dr. Fauci, a Dr. Birx, a replaceable CDC director, a TV doctor, a big pharma CEO, or a Cuomo brother out there to lie to your face about how they were all just following The ScienceTM, why not use AI and ML and combine them with behavioral sciences in order to concoct your “public health communications strategies?”
When you look at recently announced DARPA programs like Kallisti and MAGICS, which are aimed at creating an algorithmic Theory of Mind to model, predict, and influence collective human behavior, you start to get a sense of how all these programs can interweave:
“The MAGICS ARC calls for paradigm-shifting approaches for modeling complex, dynamic systems for predicting collective human behaviour.” — DARPA, MAGICS ARC, April 2025
On April 8, DARPA issued an Advanced Research Concepts (ARC) opportunity for a new program called “Methodological Advancements for Generalizable Insights into Complex Systems (MAGICS)” that seeks “new methods and paradigms for modeling collective human behavior.”
Nowhere in the MAGICS description does it mention modeling or predicting the behavior of “adversaries,” as is DARPA’s custom.
Instead, it talks at length about “modeling human systems,” along with anticipating, predicting, understanding, and forecasting “collective human behavior” and “complex social phenomena” derived from “sociotechnical data sets.”
Could DARPA’s MAGICS program be applied to simulating collective human behavior when it comes to the next public health emergency, be it real or perceived?
“The goal of an upcoming program will be to develop an algorithmic theory of mind to model adversaries’ situational awareness and predict future behaviour.” — DARPA, Theory of Mind Special Notice, December 2024.
In December 2024, DARPA launched a similar program called Theory of Mind, which was renamed Kallisti a month later.
The goal of Theory of Mind is to develop “new capabilities to enable national security decisionmakers to optimize strategies for deterring or incentivizing actions by adversaries,” according to a very brief special announcement.
DARPA never mentions who those “adversaries” are. In the case of a public health emergency, an adversary could be anyone who questions authoritative messaging.
The Theory of Mind program will also:
… seek to combine algorithms with human expertise to explore, in a modeling and simulation environment, potential courses of action in national security scenarios with far greater breadth and efficiency than is currently possible.
This would provide decisionmakers with more options for incentive frameworks while preventing unwanted escalation.
We are interested in a comprehensive overview of current and emerging technologies for disease outbreak simulation, how simulation approaches could be extended beyond standard modeling methods, and to understand how diseases spread within and between individuals including population level dynamics.
They say that all the modeling and simulating across programs is for “national security,” but that is a very broad term.
DARPA is in the business of research and development for national security purposes, so why is the Pentagon modeling disease outbreaks and intervention strategies while simultaneously looking to predict and manipulate collective human behavior?
If and when the next outbreak occurs, the same draconian and Orwellian measures that governments and corporations deployed in the name of combating COVID are still on the table.
And AI, Machine Learning, and the military will play an even bigger role than the last time around.
From analyzing wastewater to learning about disease spread; from developing pharmaceuticals to measuring the effects of lockdowns and vaccine passports, from modeling and predicting human behavior to coming up with messaging strategies to keep everyone in compliance – “improving preparedness for future public health emergencies” is becoming more militaristically algorithmic by the day.
“We are exploring innovative solutions to enhance our understanding of outbreak dynamics and to improve preparedness for future public health emergencies.” — DARPA, Advanced Disease Outbreak Simulation Capabilities RFI, May 2025.
Kennedy on Covid Jabs as a Military Operation:
"Turns out that the vaccines were developed not by Moderna and Pfizer. They were developed by NIH.”
“They're owned. The patents are owned 50% by NIH.
They were manufactured by military contractors.”
pic.twitter.com/R6y8i8tAsD— Jonny Paradise 🌱 (@plantparadise7) April 15, 2025
Reprinted with permission from The Sociable.

Audit report reveals Canada’s controversial COVID travel app violated multiple rules

Iran nuclear talks were ‘coordinated deception’ between US and Israel: report

Carney promotes MP instrumental in freezing Freedom Convoy donors’ bank accounts
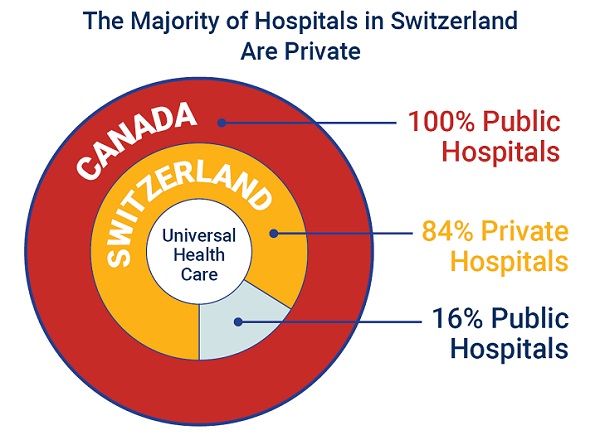
84% of Swiss hospitals and 60% of hospitalizations are in private facilities, and they face much lower wait times
-
 Business1 day ago
Business1 day agoCarney’s European pivot could quietly reshape Canada’s sovereignty
-
 Alberta24 hours ago
Alberta24 hours agoAlberta’s grand bargain with Canada includes a new pipeline to Prince Rupert
-
 Crime1 day ago
Crime1 day agoManhunt on for suspect in shooting deaths of Minnesota House speaker, husband
-
 Bruce Dowbiggin8 hours ago
Bruce Dowbiggin8 hours agoWOKE NBA Stars Seems Natural For CDN Advertisers. Why Won’t They Bite?
-
 Crime9 hours ago
Crime9 hours agoMinnesota shooter arrested after 48-hour manhunt
-
 Energy9 hours ago
Energy9 hours agoCould the G7 Summit in Alberta be a historic moment for Canadian energy?
-
 conflict2 hours ago
conflict2 hours agoIsrael bombs Iranian state TV while live on air
-
 Aristotle Foundation6 hours ago
Aristotle Foundation6 hours agoThe Canadian Medical Association’s inexplicable stance on pediatric gender medicine