COVID-19
WHO member states agree to develop legally-binding pandemic treaty

Article submitted by The Counter Signal
The World Health Organization (WHO) announced that member states inched closer to developing a legally binding global pandemic treaty.
“I welcome the agreement by @WHO Member States to develop a zero draft of a legally binding #PandemicAccord designed to protect the world from future pandemics and to continue discussions on the draft in February 2023,” said WHO CEO Dr. Tedros Adhanom Ghebreyesus.
The development follows a third meeting from WHO member states to develop a global pandemic treaty. The first meeting was in December 2021, and the second was in March 2022.
It’s unclear how the WHO’s pandemic treaty will affect its 194 member states, including Canada.
The WHO states the global pandemic treaty will determine future pandemic requirements for individual countries, such as lockdowns, and that these requirements will be “legally binding.”
The WHO says the treaty will be a “legal instrument, rooted in the WHO Constitution, designed to protect the world from future pandemics.”
Article 21 of the WHO’s constitution states the WHO has “authority to adopt regulations concerning (a) sanitary and quarantine requirements and other procedures designed to prevent the international spread of disease.”
“Other procedures” presumably include global vaccine passports, which member states have already supported.
However, the WHO also claims the pandemic treaty will “respect sovereignty.”
The draft that resulted from this third meeting includes a provision that reads:
“States have, in accordance with the Charter of the United Nations and the principles of international law, the sovereign right to determine and manage their approach to public health, notably pandemic prevention, preparedness, response and recovery of health systems pursuant to their own policies and legislation provided that activities within their jurisdiction or control do not cause damage to other States and their peoples.”
Conservative MP Leslyn Lewis has been outspoken regarding the potential impact a global pandemic treaty could have on Canadians.
In April, she said the treaty would allow the WHO to determine what a pandemic is and when one is occurring — even over something non-viral like an obesity crisis.
Earlier this year, the WHO and the German health minister said that countries disobeying regulations dictated by the WHO through their pandemic treaty might need to be sanctioned.
The Counter Signal contacted the WHO for comment but did not receive a response by publication.

From the Brownstone Institute
Instead of admitting policy error that the Covid vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates.
In so many words—and data—CDC has quietly admitted that all of the indignities of the Covid-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, and especially the vaccines; all of it failed to control the pandemic.
It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period, in 2006. The spread of a new virus with replication factor R0 of about 3, with more than one million cases across the country by April 2020, with no potentially virus-sterilizing vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
Covid-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully 2-3 weeks later. Thus, management of the Covid-19 pandemic should not have relied upon counts of cases or infections, but on numbers of deaths, numbers of people hospitalized or with serious long-term outcomes of the infection, and of serious health, economic, and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities.
Even though numbers of Covid cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because Covid-19 infection mortality is estimated to range below 0.1% in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious “long-Covid” on first infection.
Nevertheless, once the Covid-19 vaccines were rolled out, with a new large wave of the Delta strain spreading across the US in July-August 2021 even after eight months of the vaccines taken by half of Americans, instead of admitting policy error that the Covid vaccines do not much control virus spread, our public health administration doubled down, attempting then to compel vaccination on as many more people as could be threatened by mandates. That didn’t work out too well as seen when the large Omicron wave hit the country during December 2021-January 2022 in spite of some 10% more of the population getting vaccinated from September through December of 2021.
A typical mandate example: in September 2021, Washington Governor Jay Inslee issued Emergency Proclamation 21-14.2, requiring Covid-19 vaccination for various groups of state workers. In the proclamation, the stated goal was, “WHEREAS, COVID-19 vaccines are effective in reducing infection and serious disease, and widespread vaccination is the primary means we have as a state to protect everyone…from COVID-19 infections.” That is, the stated goal was to reduce the number of infections.
What the CDC recently reported (see chart below), however, is that by the end of 2023, cumulatively, at least 87% of Americans had anti-nucleocapsid antibodies to and thus had been infected with SARS-CoV-2, this in spite of the mammoth, protracted and booster-repeated vaccination campaign that led to about 90% of Americans taking the shots. My argument is that by making policies based on number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce spread failed in that 87% of Americans eventually became infected anyway.

In reality, neither vaccine immunity nor post-infection immunity were ever able fully to control the spread of the infection. On August 11, 2022, the CDC stated, “Receipt of a primary series alone, in the absence of being up to date with vaccination* through receipt of all recommended booster doses, provides minimal protection against infection and transmission (3,6). Being up to date with vaccination provides a transient period of increased protection against infection and transmission after the most recent dose, although protection can wane over time.” Public health pandemic measures that “wane over time” are very unlikely to be useful for control of infection spread, at least without very frequent and impractical revaccinations every few months.
Nevertheless, infection spread per se is not of consequence, because count of infections is not and should not have been the main priority of public health pandemic management. Rather, the consequences of the spread and the negative consequences of the policies invoked should have been the priorities. Our public health agencies chose to prioritize a failed policy of reducing the spread rather than reducing the mortality or the lockdown and school and business closure harms, which led to unnecessary and avoidable damage to millions of lives. We deserved better from our public health institutions.
Republished from the author’s Substack
Author

COVID-19
Japanese study shows disturbing increase in cancer related deaths during the Covid pandemic
From Cureus.com
The study is called:
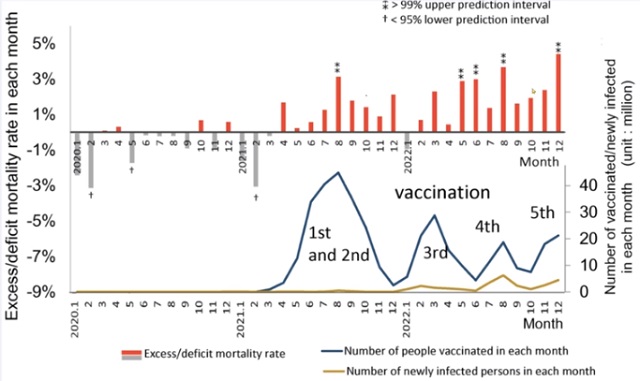
Increased Age-Adjusted Cancer Mortality After the Third mRNA-Lipid Nanoparticle Vaccine Dose During the COVID-19 Pandemic in Japan
During the COVID-19 pandemic, excess deaths including cancer have become a concern in Japan, which has a rapidly aging population. Thus, this study aimed to evaluate how age-adjusted mortality rates (AMRs) for different types of cancer in Japan changed during the COVID-19 pandemic (2020-2022).
Introduction
The COVID-19 pandemic began in December 2019 in Wuhan, China, and was first detected in Japan in January 2020. In response, a range of healthcare and socio-economic restrictions were implemented to curb the spread of the disease. Since February 2021, the mRNA-lipid nanoparticle (mRNA-LNP) vaccine has been available for emergency use and is recommended for all individuals aged six months and older, especially those at high risk.
As of March 2023, 80% of the Japanese population had received their first and second doses, 68% had received their third dose, and 45% had received their fourth dose [1]. Despite these national measures, 33.8 million people had been infected, and 74,500 deaths had been attributed to COVID-19 in Japan by the end of April 2023.
Additionally, excess deaths from causes other than COVID-19 have been reported in various countries [2-6], including deaths from cancer [7-10], and Japan is no exception [11,12]. Cancer is the leading cause of death in Japan, accounting for one-fourth of all deaths. Therefore, it is essential to understand the effects of the pandemic on mortality rates of cancer from 2020 to 2022. Age adjustment is necessary for accurate evaluation, especially in diseases such as cancer that tend to occur in elderly adults.
Japan has several characteristics that make it ideal for analyzing the impact of the pandemic on cancer mortality rates, including its large population of 123 million, availability of official statistics, and the high 80% accuracy rate of death certificates according to autopsy studies [13].
Conclusions
Statistically significant increases in age-adjusted mortality rates of all cancer and some specific types of cancer, namely, ovarian cancer, leukemia, prostate, lip/oral/pharyngeal, pancreatic, and breast cancers, were observed in 2022 after two-thirds of the Japanese population had received the third or later dose of SARS-CoV-2 mRNA-LNP vaccine. These particularly marked increases in mortality rates of these ERα-sensitive cancers may be attributable to several mechanisms of the mRNA-LNP vaccination rather than COVID-19 infection itself or reduced cancer care due to the lockdown. The significance of this possibility warrants further studies.
From the YouTube channel of Dr John Campbell
CDC Quietly Admits to Covid Policy Failures
Deborah Birx Gets Her Close-Up
Trudeau gov’t still receiving COVID shots while throwing away $1.5 billion worth of expired jabs

Conservative MP testifies that foreign agents could effectively elect Canada’s prime minister, premiers
-
COVID-194 hours ago
CDC Quietly Admits to Covid Policy Failures
-
COVID-197 hours ago
Japanese study shows disturbing increase in cancer related deaths during the Covid pandemic
-
 Great Reset2 hours ago
Great Reset2 hours agoClimate expert warns against extreme ‘weather porn’ from alarmists pushing ‘draconian’ policies
-
 Alberta2 days ago
Alberta2 days agoDanielle Smith warns arsonists who start wildfires in Alberta that they will be held accountable
-
 Bruce Dowbiggin1 day ago
Bruce Dowbiggin1 day agoWhy Are Canadian Mayors So Far Left And Out Of Touch?
-
 National2 days ago
National2 days agoCanada’s Governor General slammed for hosting partisan event promoting Trudeau’s ‘hate speech’ bill
-
 Economy1 day ago
Economy1 day agoExtreme Weather and Climate Change
-
 International1 day ago
International1 day agoTelegram founder tells Tucker Carlson that US intel agents tried to spy on user messages