Alberta
Masks to be mandatory in Alberta schools – Update on back to school plan

From the Province of Alberta
School health measures now include mandatory masks
As part of a number of new school safety measures to combat COVID-19, mask use for Grade 4 to 12 students, and all school staff, will be mandatory when school returns for the 2020-21 year.
While mandatory mask use is for students in Grades 4 to 12 and all staff, all students and staff in public, separate, Francophone, charter and independent schools will receive two reusable masks from Alberta’s government. More than 1.6 million masks will be distributed to 740,000 students and 90,000 staff. Additional single-use masks will be available at schools, if required.
Mask use will be mandatory for staff and teachers in all settings where physical distancing cannot be maintained. Students will be required to wear them in all shared and common areas such as hallways and on buses. Exemptions will be made for students and staff who are unable to wear a mask due to medical or other needs.
Mask use for kindergarten to Grade 3 students will continue to be optional. Mask use for younger children is a challenge due to difficulties with proper fit and compliance. In addition, evidence shows that children under 10 may be less likely than older children or adults to transmit COVID-19.
“The safety of our staff and students continues to be my number 1 priority. Since cancelling in-person classes in March and developing our school re-entry plan, we have been clear that we would continue to adapt our guidelines as necessary based on current medical advice. These new safety measures will help prevent the spread of COVID-19 in our schools, and we will continue to work with our school authorities to ensure they are equipped for a successful start to the school year.”
“After reviewing the emerging evidence, it is clear that masks can play an important role in limiting the spread of COVID-19. I am not making this updated recommendation lightly, but acting on the best current evidence available. While masks are important, I want to stress that they are only one of the many public health measures in place to limit the spread of COVID-19 and protect the health of students, staff and families.”
“CASS’ board of directors appreciates the government’s commitment to adapting Alberta’s health guidelines as new medical information becomes available and for ensuring school divisions are receiving the protective equipment they need for a successful transition back to school. This announcement clearly demonstrates Alberta Education’s willingness to take the necessary steps to support the safety of staff and students. We appreciate their continued collaboration and support as we approach the beginning of a new school year.”
Alberta’s government remains committed to adjusting the school re-entry guidelines based on current medical advice. The chief medical officer of health has been studying the evidence around masking in schools, and this decision is a direct result of evolving medical advice.
Face shields
School staff will receive one reusable face shield for their use in the schools. Shield use is at the discretion of the individual staff member. Plastic face shields can help reduce exposure but are not equivalent to masks. A mask must still be worn while wearing a face shield.
Hand sanitizer
About 466,000 litres of hand sanitizer will be distributed between all school authorities. The specific volume provided to an individual school authority will be based on student population.
Thermometers
Each school will receive two contactless thermometers to assist with managing student and staff health. Thermometer use will be at the discretion of the school authority.
Staff testing
Alberta Health and Alberta Health Services are working hard to expand testing capacity and reduce turnaround times for testing, including in-school staff, teachers and students, so that anyone with symptoms or close contacts of cases can be rapidly tested and receive test results promptly.
All supplies will be distributed to school authorities by the beginning of the 2020-21 school year. Authorities will then distribute to individual schools, staff and/or students based on the needs of their own communities.
Provincial health guidance for a safe return to school will continue to evolve as necessary to reflect the latest evidence on the nature of the COVID-19 pandemic.
Individual school authorities are developing return-to-school plans that meet the needs of their own communities. These plans are based on direction provided under the provincial school re-entry plan, and supporting health guidance documents.
Alberta’s Recovery Plan is a bold, ambitious long-term strategy to build, diversify, and create tens of thousands of jobs now. By building schools, roads and other core infrastructure we are benefiting our communities. By diversifying our economy and attracting investment with Canada’s most competitive tax environment, we are putting Alberta on a path for a generation of growth. Alberta came together to save lives by flattening the curve and now we must do the same to save livelihoods, grow and thrive.
Quick facts
- Alberta’s government announced students and staff would return to school under scenario 1 – near-normal daily operations with health measures – on July 21.
- School authorities are required to be prepared to move between the three scenarios outlined in the provincial school re-entry plan. Changes to scenarios will be determined by Alberta Education.

From the Montreal Economic Institute
Quebec has experienced increased productivity and efficiency, as well as reduced costs, in those sectors to which ABF has been applied
Alberta’s healthcare system costs more than those of many of its peers across Canada and internationally, yet underperforms by many metrics—wait times perhaps being the most visible.(1) For instance, while Alberta consistently spends a fair deal more per capita on health care than Canada’s other large provinces do, the median wait time from referral by a GP to treatment by a specialist was 33.3 weeks in 2022, versus 29.4 weeks in Quebec, 25.8 weeks in British Columbia, and 20.3 weeks in Ontario. Albertans waited a median 232 days for a hip replacement that year, longer than those in Quebec, British Columbia, and Ontario.(2) In Australia, meanwhile, the median wait time for a total hip replacement in 2022 was 175 days in public hospitals.(3)
One of the things keeping Alberta’s healthcare system from better performance is that it relies on global budgets for its hospital financing. Such a system allocates a pre-set amount of funding to pay for an expected number of services, based largely on historical volume. The problem with global budgets is that they disregard the actual costs incurred to deliver care, while undermining incentives to improve outcomes. This ultimately leads to rationing of care, with patients viewed as a cost that must be managed.
Activity-based funding systems are associated with reduced hospital costs, increased efficiency, and shorter wait times, among other things.
An alternative is activity-based funding (ABF), which has largely replaced global budgeting in many OECD countries, and is starting to do so in some Canadian provinces.(4) With ABF, hospitals receive a fixed payment for each specific service delivered, adjusted for certain parameters.(5) If a hospital treats more patients and delivers more services, it receives more funding; if it does less, it receives less. In essence, the money follows the patient, which has a dramatic effect: patients are now viewed as a source of revenue, not merely as a cost. Studies have shown that ABF systems that include appropriate safeguards for quality and waste are associated with reduced hospital costs, increased efficiency, and shorter wait times, among other things.(6)
To increase its capacity and performance, Alberta should consider moving to such a system for hospital financing. As over 25% of total health spending in the province goes to hospitals,(7) driving down costs and finding efficiencies is of paramount importance.
ABF models vary by jurisdiction and context to account for distinct situations and the particular policy objectives being pursued.(8) Two jurisdictions provide interesting insights: Quebec, with ABF hospital funding being gradually implemented in recent years, and Australia, where after more than three decades, ABF is the rule, global budgets the exception.
ABF in Quebec: Increased Performance and Decreased Costs
Quebec’s hospital payment reforms over the past two decades have been aimed at better linking funding with health care delivery to improve care quality and access.(9) These patient-based funding reforms (a type of ABF) have resulted in increased volumes and efficiency, and reduced costs and wait times for a number of surgical and other procedures in Quebec.(10)
These reforms started in 2004, when Quebec applied ABF in the context of additional funding to select surgeries in order to reduce wait times through the Access to Surgery Program.(11) The surgeries initially targeted were hip replacement, knee replacement, and cataract surgeries, but other procedures were eventually integrated into the program as well. Its funding covered the volume of surgeries that exceeded those performed in 2002-2003, and it used the average cost for each specific surgery. Procedures were classified by cost category, which also took into account the intensity of resource use and unit cost based on direct and indirect costs.
The expansion of ABF in Quebec aims to relieve hospital congestion by driving down wait times and shrinking wait lists.
By 2012-2013, this targeted program had helped to significantly increase the volume of surgeries performed, as well as decrease wait times and length of stay.(12) However, as ABF was applied only to surplus volumes of additional surgeries, efficiency gains were limited. For this reason, among others, the Expert Panel for Patient-Based Funding recommended expanding the program,(13) and in 2012, the Government of Quebec began considering further pilot projects for gradual ABF implementation.(14)
- In 2015, ABF was implemented in the radiation oncology sector, which resulted in better access to services at a lower cost, with productivity having increased more than 26% by 2023-2024, and average procedure costs having fallen 7%.(15)
- In 2017-2018, ABF was implemented in imaging, which resulted in the number of magnetic resonance imaging tests increasing more than 22% while driving the unit cost of procedures down 4%.(16)
- Following the above successes, in 2018-2019, the colonoscopy and digestive endoscopy sector also moved to ABF, which led to a productivity increase of 14% and a 31% decrease in the case backlog.(17)
Overall, then, Quebec has experienced increased productivity and efficiency, as well as reduced costs, in those sectors to which ABF has been applied (see Figure 1).

The Department of Health and Social Services continued to expand ABF to more surgeries in 2023, following which it was expected that about 25% of the care and services offered in physical health in Quebec hospitals would be funded in this manner, with the goal of reaching 100% by 2027-2028.(18) Further, the 2024-2025 budget expanded ABF again to include the medicine, emergency, neonatal, and dialysis sectors.
This expansion of ABF aims to relieve hospital congestion by driving down wait times and shrinking wait lists.(19) It will also align Quebec’s health care funding with what has become standard in most OECD countries. In Australia, for instance, ABF is the rule, not the exception, covering a large proportion of hospital services.
Australia’s Extensive Use of ABF
Australia also implemented ABF in stages, as Quebec is now doing. It was first introduced in the 1990s in one state and adopted nationally in 2012 for all admitted programs to increase efficiency, while also integrating quality and safety considerations.(20) These considerations act as safeguards to ensure efficiency incentives don’t negatively impact services. For instance, there are adjustments to the ABF payment framework in the presence of hospital acquired complications and avoidable hospital readmissions, two measures of hospital safety and service quality.(21) If service quality were to decrease, funding would be adjusted, and payments would be withheld. Not only has ABF been successful in increasing hospital efficiency in Australia, but it has also enabled proactive service improvement, which has in turn had a positive impact on safety and quality.(22)
ABF now makes up 87.0% of total hospital spending in Australia, ranging from 83.6% in Tasmania to 93.0% in the Australian Capital Territory.
Currently, ER services, acute services, admitted mental health services, sub-acute and non-acute services, and non-admitted services are funded with ABF in Australia. This includes rehabilitation, palliative, geriatric and/or maintenance care.(23) Global budgets are still used for some block funding, but this is the exception, restricted to certain hospitals, programs, or specific episodes of care.(24) Small rural hospitals, non-admitted mental health programs, and a few other highly specialized therapies or clinics or some community health services tend to be block funded due to higher than average costs stemming from a lack of economies of scale and inadequate volumes, among other things.
When first introduced, ABF made up about 25% of hospital revenue (approximately where Quebec currently stands).(25) ABF now makes up 87.0% of total hospital spending in Australia, ranging from 83.6% in Tasmania to 93.0% in the Australian Capital Territory (see Figure 2).

There is more variability, however, at the local hospital network level within territories or states. For instance, between 2019 and 2024, an average of 92.3% of total funding for the hospitals in the South Eastern Sydney Local Health District was ABF, and just 7.7% was block funding.(26) For the hospitals in the Far West Local Health District, in comparison, ABF represented an average of 72.0% of total funding, and block payments 28.0%, over the same period.(27)
The proportion of ABF funding per hospital is dictated, for the most part, by the types and volumes of patient services provided, but also by hospital characteristics and regional patient demographics.(28) For example, there could be a need to compensate for differences in hospital size and location, or to reimburse for some alternative element of the fixed cost of providing services. In the Far West Local Health District, on average 65.1% of block funding between 2019-2020 and 2023-2024 was provided for small rural hospitals, while only 1.4% of the block funding in the South Eastern Sydney Local Health District was for these types of hospitals.(29) Ultimately, these two districts serve very different populations, with the Far West Local Health District being the most thinly populated district in Australia.(30)
Overall, ABF implementation in Australia has significantly improved hospital performance. Early after ABF implementation, the volume of care in Australia increased, and waiting lists decreased by 16% in the first year.(31) Between 2005 and 2017 the hospitals that were funded by ABF in Queensland became more efficient than those receiving block funding.(32) In addition, ABF can contribute to reductions in extended lengths of stay and hospital readmission,(33) both of which are expensive propositions for health care systems and also tie up hospital beds and resources.
Conclusion
ABF has been associated with reduced hospital costs, increased efficiency, and shorter wait times, areas where Alberta is lacking and reform is needed. To increase its health system performance, Alberta should consider emulating Quebec and moving to an activity-based funding system. Indeed, based on the experience of countries like Australia, widespread application should be the goal, as it is in Quebec. Alberta patients have already waited far too long for timely access to the quality care they deserve. The time to act is now.
The MEI study is available here.
* * *
This Economic Note was prepared by Krystle Wittevrongel, Senior Policy Analyst and Alberta Project Lead at the MEI. The MEI’s Health Policy Series aims to examine the extent to which freedom of choice and entrepreneurship lead to improvements in the quality and efficiency of health care services for all patients.
The MEI is an independent public policy think tank with offices in Montreal and Calgary. Through its publications, media appearances, and advisory services to policy-makers, the MEI stimulates public policy debate and reforms based on sound economics and entrepreneurship.
Alberta
Red Deer Doctor critical of Alberta’s COVID response to submit report to Danielle Smith this May

From LifeSiteNews
Leading the task force is Dr. Gary Davidson, who was skeptical of mandates at the time.
Alberta Premier Danielle Smith will soon be receiving a little-known report she commissioned which tasked an Alberta doctor who was critical of the previous administration’s handling of COVID to look into how accurate the province’s COVID data collection was, as well as the previous administration’s decision-making process and effectiveness.
As noted in a recent Globe and Mail report, records it obtained show that just less than one month after becoming Premier of Alberta in November of 2022, Smith tasked then-health minister Jason Copping to create the COVID data task force.
Documents show that the Alberta government under Smith gave the new task force, led by Dr. Gary Davidson – who used to work as an emergency doctor in Red Deer, Alberta – a sweeping mandate to look at whether the “right data” was obtained during COVID as well as to assess the “integrity, validity, reliability and quality of the data/information used to inform pandemic decisions” by members of Alberta Health Services (AHS).
As reported by LifeSiteNews in 2021, Davidson said during the height of COVID that the hospital capacity crisis in his province was “created,” was not a new phenomenon, and had nothing to do with COVID.
“We have a crisis, and we have a crisis because we have no staff, because our staff quit, because they’re burned out, they’re not burnt out from COVID,” Davidson said at the time.
Davidson also claimed that the previous United Conservative Party government under former Premier Jason Kenney had been manipulating COVID statistics.
In comments sent to the media, Smith said that in her view it was a good idea to have a “contrarian perspective” with Davidson looking at “everything that happened with some fresh eyes.”
“I needed somebody who was going to look at everything that happened with some fresh eyes and maybe with a little bit of a contrarian perspective because we’ve only ever been given one perspective,” she told reporters Tuesday.
“I left it to [Davidson] to assemble the panel with the guidance that I would like to have a broad range of perspectives.”
Smith took over from Kenney as leader of the UCP on October 11, 2022, after winning the leadership of the party. The UCP then won a general election in May 2023. Kenney was ousted due to low approval ratings and for reneging on promises not to lock Alberta down during COVID.
After assuming her role as premier, Smith promptly fired the province’s top doctor, Deena Hinshaw, and the entire AHS board of directors, all of whom oversaw the implementation of COVID mandates.
Under Kenney, thousands of nurses, doctors, and other healthcare and government workers lost their jobs for choosing to not get the jabs, leading Smith to say – only minutes after being sworn in – that over the past year the “unvaccinated” were the “most discriminated against” group of people in her lifetime.
As for AHS, it still is promoting the COVID shots, for babies as young as six months old, as recently reported by LifeSiteNews.
Task force made up of doctors both for and against COVID mandates
In addition to COVID skeptic Dr. Gary Davidson, the rather secretive COVID task force includes other health professionals who were critical of COVID mandates and health restrictions, including vaccine mandates.
The task force was given about $2 million to conduct its review, according to The Globe and Mail, and is completely separate from another task force headed by former Canadian MP Preston Manning, who led the Reform Party for years before it merged with another party to form the modern-day Conservative Party of Canada.
Manning’s task force, known as the Public Health Emergencies Governance Review Panel (PHEGRP), released its findings last year. It recommend that many pro-freedom policies be implemented, such as strengthening personal medical freedoms via legislation so that one does not lose their job for refusing a vaccine, as well as concluding that Albertans’ rights were indeed infringed upon.
The Smith government task force is run through the Health Quality Council of Alberta (HQCA) which is a provincial agency involved in healthcare research.
Last March, Davidson was given a project description and terms of reference and was told to have a final report delivered to Alberta’s Health Minister by December of 2023.
As of now, the task force’s final report won’t be available until May, as per Andrea Smith, press secretary to Health Minister Adriana LaGrange, who noted that the goal of the task force is to look at Alberta’s COVID response compared to other provinces.
According to the Globe and Mail report, another person working on the task force is anesthetist Blaine Achen, who was part of a group of doctors that legally challenged AHS’s now-rescinded mandatory COVID jab policy for workers.
Some doctors on the task force, whom the Globe and Mail noted held “more conventional views regarding the pandemic,” left it only after a few meetings.
In a seeming attempt to prevent another draconian crackdown on civil liberties, the UCP government under Smith has already taken concrete action.
The Smith government late last year passed a new law, Bill 6, or the Public Health Amendment Act, that holds politicians accountable in times of a health crisis by putting sole decision-making on them for health matters instead of unelected medical officers.



Deborah Birx Gets Her Close-Up

Biden’s Kill Switch: The Growing Threat of Government Control of Your Car

US firms like BlackRock are dropping their climate obsession while Europe ramps theirs up
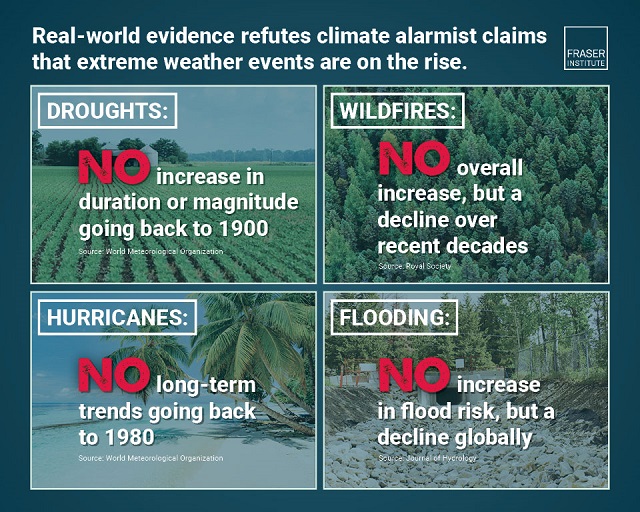
Extreme Weather and Climate Change
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoDesperate Liberals move to stop MPs from calling Trudeau ‘corrupt’
-
 Health1 day ago
Health1 day agoTransgender activists are threatening the author of scathing UK report on child ‘sex changes’
-
 conflict1 day ago
conflict1 day agoCol. Douglas Macgregor torches Trump over support for bill funding wars in Ukraine and Israel
-
 Frontier Centre for Public Policy1 day ago
Frontier Centre for Public Policy1 day agoThe end of Canada: The shift from democracy to totalitarian behavior in the ‘pandemic era’
-
 COVID-192 days ago
COVID-192 days agoInquiry shows Canadian gov’t agencies have spent $10 million on social media ads for COVID jabs
-
 International1 day ago
International1 day agoBiden admin expands Title IX to include ‘gender identity,’ sparking conservative backlash
-
 Alberta1 day ago
Alberta1 day agoAlberta’s baby name superstar steals the show again
-
 Business2 days ago
Business2 days agoFederal government’s ‘fudget budget’ relies on fanciful assumptions of productivity growth