Health
Was football player Terrance Howard really dead? His parents didn’t think so.

From LifeSiteNews
The Uniform Determination of Death Act (UDDA) states that there must be an irreversible cessation of all functions of the entire brain for a declaration of brain death. The way doctors currently diagnose brain death does not comply with the law under the UDDA.
North Carolina Central University football player Terrance Howard died recently after a car accident reportedly left him “brain dead.” But his family disputed this diagnosis and requested that their son be transferred to another facility for treatment of his brain injury, leading to conflict with Terrance’s doctors and hospital. According to News One, his parents claimed that Atrium Health Carolinas Medical Center wanted to kill their son for his organs, and accused doctors of snickering and laughing while refusing to help him. His father, Anthony Allen, told News One that the hospital removed Terrance from life support against his family’s wishes and forcibly ejected his family from his room. The family posted videos on social media of apparent police officers entering Terrance’s hospital room, and said that the hospital threatened them with criminal action for trespassing.
If these allegations are true, the Howard family has every right to be outraged at the disrespectful treatment they received at Atrium Health. Especially now, as the legitimacy of brain death is coming under increasing scrutiny, it is outrageous that hospitals and doctors continue being so heavy-handed. The National Catholic Bioethics Center (NCBC), formerly a staunch supporter of “brain death,” released a statement in April 2024, saying:
Events in the last several months have revealed a decisive breakdown in a shared understanding of brain death (death by neurological criteria) which has been critical in shaping the ethical practice of organ transplantation. At stake now is whether clinicians, potential organ donors, and society can agree on what it means to be dead before vital organs are procured.
The NCBC statement was prompted by the newest brain death guideline which explicitly allows people with partial brain function to be declared brain dead. But the Uniform Determination of Death Act (UDDA) states that there must be an irreversible cessation of all functions of the entire brain for a declaration of brain death. The way doctors currently diagnose brain death does not comply with the law under the UDDA.
Terrance Howard’s story is reminiscent of the mistreatment of another Black teenager, Jahi McMath. In 2013, Jahi was a quiet, cautious teenager with sleep apnea who underwent a tonsillectomy and palate reconstruction to improve her airflow while sleeping. An hour after the surgery, she started spitting up blood. Her parents requested repeatedly to see a doctor without success. Her mother, Nailah Winkfield, said, “No one was listening to us, and I can’t prove it, but I really feel in my heart: if Jahi was a little white girl, I feel we would have gotten a little more help and attention.”
Jahi continued to bleed until she had a cardiac arrest just after midnight. She was pulseless for ten minutes during her “code blue” resuscitation. Two days later, her electroencephalogram (EEG) was flatline, and it was clear that Jahi had suffered a severe brain injury which was worsening. But rather than treating these findings aggressively, her doctors proceeded toward a diagnosis of brain death. Three days after her surgery, her parents were informed that their daughter was “dead” and that Jahi could now become an organ donor. The family was stunned. How could Jahi be dead? She was warm, she was moving occasionally, and her heart was still beating. As a Christian, Nailah believed her daughter’s spirit remained in her body as long as her heart continued to beat. While the family sought medical and legal assistance, Children’s Hospital Oakland doubled down, refusing to feed Jahi for three weeks. The hospital finally agreed to release Jahi to the county coroner for a death certificate, following which her family would be responsible for her.
On January 3, 2014, Jahi received a death certificate from California, listing her cause of death as “Pending Investigation.” Why was the hospital so adamant about insisting Jahi was dead, even to the point of issuing a death certificate? Possibly because California’s Medical Injury Compensation Reform Act limits noneconomic damages to $250,000. If Jahi was “dead,” the hospital and its malpractice insurer would only be liable for $250,000. But if Jahi was alive, there would be no limit to the amount her family could claim for her ongoing care.
After Jahi was transferred to New Jersey, the only US state with a religious exemption to a diagnosis of brain death, she began to improve. After noticing that Jahi’s heart rate would decrease at the sound of her mother’s voice, the family began asking her to respond to commands, and videoed her correct responses. Jahi went through puberty and began to menstruate — something not seen in corpses! By August 2014 she was stable enough to move into her mother’s apartment for continuing care. Subsequently Jahi was examined by two neurologists (Dr. Calixto Machado and Dr. D. Alan Shewmon) who found that she had definitely improved: she no longer met the criteria for brain death and was in a minimally conscious state. Jahi continued responding to her family in a meaningful way until her death in June 2018 from complications of liver failure.
How could Jahi McMath, who was declared brain dead by three doctors, who failed three apnea tests, and who had four flatline EEGs and a radioisotope scan showing no intracranial blood flow, go on to recover neurologic function? Very likely, due to a condition called Global Ischemic Penumbra, or GIP. Like every other organ, the brain shuts down its function when its blood flow is reduced in order to conserve energy. At 70 percent of normal blood flow, the brain’s neurological functioning is reduced, and at a 50 percent reduction the EEG becomes flatline. But tissue damage doesn’t begin until blood flow to the brain drops below 20 percent of normal for several hours. GIP is a term doctors use to refer to that interval when the brain’s blood flow is between 20 and 50 percent of normal. During GIP the brain will not respond to neurological testing and has no electrical activity on EEG, but still has enough blood flow to maintain tissue viability — meaning that recovery is still possible. During GIP, a person will appear “brain dead” using the current medical guidelines and testing, but with continuing care they could potentially improve.
Dr. D. Alan Shewmon, one of the world’s leading authorities on brain death, describes GIP this way:
This [GIP] is not a hypothesis but a mathematical necessity. The clinically relevant question is therefore not whether GIP occurs but how long it might last. If, in some patients, it could last more than a few hours, then it would be a supreme mimicker of brain death by bedside clinical examination, yet the non-function (or at least some of it) would be in principle reversible.
Dr. Cicero Coimbra first described GIP in 1999, but in the never-ending quest for transplantable organs, his work has been largely ignored. There is absolutely no medical or moral certainty in a brain death diagnosis, and people need to be made aware of this. “Brain dead” people are very ill, and their prognosis may be death, but they deserve to be treated aggressively until they either recover or succumb to natural death. Unfortunately, as the family of Terrance Howard seems to have experienced, doctors are continuing to use a brain death guideline that ignores the reality of GIP and does not comply with brain death law under the UDDA.
Heidi Klessig MD is a retired anesthesiologist and pain management specialist who writes and speaks on the ethics of organ harvesting and transplantation. She is the author of “The Brain Death Fallacy” and her work may be found at respectforhumanlife.com.
Health
Last day and last chance to win this dream home! Support the 2025 Red Deer Hospital Lottery before midnight!

Deadline: June 16, 2025
Draw: June 26, 2025
|



|
|
The 2025 Red Deer Hospital Lottery Dream Home, designed by Sorento Custom Homes, continues Sorento’s tradition of award-winning designs. This gorgeous bungalow features 2,824 sq ft of developed living space and showcases a tall, vaulted ceiling.














Located at 128 Emmett Crescent in the neighbourhood of Evergreen, this outstanding home features a screened deck off the dining room, a large family room on the lower level, and of course, a beautiful primary suite. Sorento’s ensuites are always something to behold, and this one features a claw foot tub. There’s an office on the main level, two bedrooms below, and a large fitness room that includes a two-person infrared sauna. Enjoy the convenience of a walk-in pantry, main floor laundry, and chef quality appliances. The design of this unique home is complemented by gorgeous furnishings by Urban Barn.
Our Grand Prize Dream Home package is valued at $1,074,472! You won’t want to miss seeing this outstanding home or your chance to live in it.
50 FOR $75
Make a Difference

Aristotle Foundation
The Canadian Medical Association’s inexplicable stance on pediatric gender medicine

![]()
By Dr. J. Edward Les
The thalidomide saga is particularly instructive: Canada was the last developed country to pull thalidomide from its shelves — three months during which babies continued to be born in this country with absent or deformed limbs
Physicians have a duty to put forward the best possible evidence, not ideology, based treatments
Late last month, the Canadian Medical Association (CMA) announced that it, along with three Alberta doctors, had filed a constitutional challenge to Alberta’s Bill 26 “to protect the relationship between patients, their families and doctors when it comes to making treatment decisions.”
Bill 26, which became law last December, prohibits doctors in the province from prescribing puberty blockers and hormone therapies for those under 16; it also bans doctors from performing gender-reassignment surgeries on minors (those under 18).
The unprecedented CMA action follows its strongly worded response in February 2024 to Alberta’s (at the time) proposed legislation:
“The CMA is deeply concerned about any government proposal that restricts access to evidence-based medical care, including the Alberta government’s proposed restrictions on gender-affirming treatments for pediatric transgender patients.”
But here’s the problem with that statement, and with the CMA’s position: the evidence supporting the “gender affirmation” model of care — which propels minors onto puberty blockers, cross-gender hormones, and in some cases, surgery — is essentially non-existent. That’s why the United Kingdom’s Conservative government, in the aftermath of the exhaustive four-year-long Cass Review, which laid bare the lack of evidence for that model, and which shone a light on the deeply troubling potential for the model’s irreversible harm to youth, initiated a temporary ban on puberty blockers — a ban made permanent last December by the subsequent Labour government. And that’s why other European jurisdictions like Finland and Sweden, after reviews of gender affirming care practices in their countries, have similarly slammed the brakes on the administration of puberty blockers and cross-gender hormones to minors.
It’s not only the Europeans who have raised concerns. The alarm bells are ringing loudly within our own borders: earlier this year, a group at McMaster University, headed by none other than Dr. Gordon Guyatt, one of the founding gurus of the “evidence-based care” construct that rightfully underpins modern medical practice, issued a pair of exhaustive systematic reviews and meta analyses that cast grave doubts on the wisdom of prescribing these drugs to youth.
And yet, the CMA purports to be “deeply concerned about any government proposal that restricts access to evidence-based medical care,” which begs the obvious question: Where, exactly, is the evidence for the benefits of the “gender affirming” model of care? The answer is that it’s scant at best. Worse, the evidence that does exist, points, on balance, to infliction of harm, rather than provision of benefit.
CMA President Joss Reimer, in the group’s announcement of the organization’s legal action, said:
“Medicine is a calling. Doctors pursue it because they are compelled to care for and promote the well-being of patients. When a government bans specific treatments, it interferes with a doctor’s ability to empower patients to choose the best care possible.”
Indeed, we physicians have a sacred duty to pursue the well-being of our patients. But that means that we should be putting forward the best possible treatments based on actual evidence.
When Dr. Reimer states that a government that bans specific treatments is interfering with medical care, she displays a woeful ignorance of medical history. Because doctors don’t always get things right: look to the sad narratives of frontal lobotomies, the oxycontin crisis, thalidomide, to name a few.
The thalidomide saga is particularly instructive: it illustrates what happens when a government drags its heels on necessary action. Canada was the last developed country to pull thalidomide, given to pregnant women for morning sickness, from its shelves, three months after it had been banned everywhere else — three months during which babies continued to be born in this country with absent or deformed limbs, along with other severe anomalies. It’s a shameful chapter in our medical past, but it pales in comparison to the astonishing intransigence our medical leaders have displayed — and continue to display — on the youth gender care file.
A final note (prompted by thalidomide’s history), to speak to a significant quibble I have with Alberta’s Bill 26 legislation: as much as I admire Premier Danielle Smith’s courage in bringing it forward, the law contains a loophole allowing minors already on puberty blockers and cross-gender hormones to continue to take them. Imagine if, after it was removed from the shelves in 1962, government had allowed pregnant women already on the drug to continue to take thalidomide. Would that have made any sense? Of course not. And the same applies to puberty blockers and cross-gender hormones: they should be banned outright for all youth.
That argument is the kind our medical associations should be making — and would be making, if they weren’t so firmly in the grasp, seemingly, of ideologues who have abandoned evidence-based medical care for our youth.
J. Edward Les is a Calgary pediatrician, a senior fellow with the Aristotle Foundation for Public Policy, and co-author of “Teenagers, Children, and Gender Transition Policy: A Comparison of Transgender Medical Policy for Minors in Canada, the United States, and Europe.”

Iran nuclear talks were ‘coordinated deception’ between US and Israel: report

Carney promotes MP instrumental in freezing Freedom Convoy donors’ bank accounts
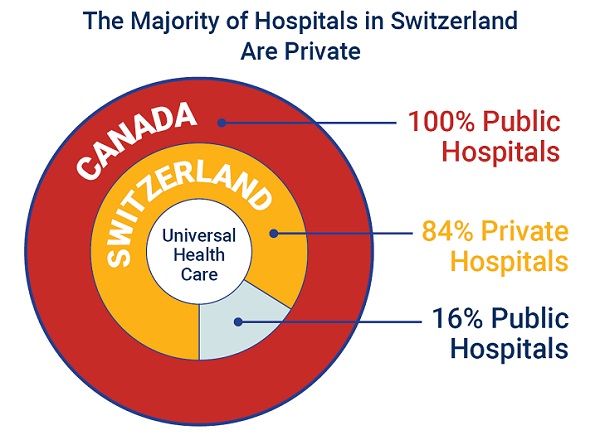
84% of Swiss hospitals and 60% of hospitalizations are in private facilities, and they face much lower wait times

The carbon tax’s last stand – and what comes after
-
 Alberta2 days ago
Alberta2 days agoAlberta’s grand bargain with Canada includes a new pipeline to Prince Rupert
-
 Bruce Dowbiggin23 hours ago
Bruce Dowbiggin23 hours agoWOKE NBA Stars Seems Natural For CDN Advertisers. Why Won’t They Bite?
-
 Business2 days ago
Business2 days agoCarney’s European pivot could quietly reshape Canada’s sovereignty
-
Health18 hours ago
Last day and last chance to win this dream home! Support the 2025 Red Deer Hospital Lottery before midnight!
-
 Crime8 hours ago
Crime8 hours agoUK finally admits clear evidence linking Pakistanis and child grooming gangs
-
 Business13 hours ago
Business13 hours agoCarney praises Trump’s world ‘leadership’ at G7 meeting in Canada
-
 Energy24 hours ago
Energy24 hours agoCould the G7 Summit in Alberta be a historic moment for Canadian energy?
-
 Crime23 hours ago
Crime23 hours agoMinnesota shooter arrested after 48-hour manhunt