Addictions
So What ARE We Supposed To Do With the Homeless?



David Clinton
Involuntary confinement is currently enjoying serious reconsideration
Sometimes a quick look is all it takes to convince me that a particular government initiative has gone off the rails. The federal government’s recent decision to shut down their electric vehicle subsidy program does feel like a vindication of my previous claim that subsidies don’t actually increase EV sales.
But no matter how hard I look at some other programs – and no matter how awful I think they are – coming up with better alternatives of my own isn’t at all straightforward. A case in point is contemporary strategies for managing urban homeless shelters. The problem is obvious: people suffering from mental illnesses, addictions, and poverty desperately need assistance with shelter and immediate care.
The Audit is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Ideally, shelters should provide integration with local healthcare, social, and employment infrastructure to make it easier for clients to get back on their feet. But integration isn’t cost-free. Because many shelters serve people suffering from serious mental illnesses, neighbors have to worry about being subjected to dangerous and criminal behavior.
Apparently, City of Toronto policy now requires their staff to obscure from public view the purchase and preparation of new shelter locations. The obvious logic driving the policy is the desire to avoid push back from neighbors worried about the impact such a facility could have.
As much as we might regret the not-in-my-back-yard (NIMBY) attitude the city is trying to circumvent, the neighbors do have a point. Would I want to raise my children on a block littered with used syringes and regularly visited by high-as-a-kite – and often violent – substance abusers? Would I be excited about an overnight 25 percent drop in the value of my home? To be honest, I could easily see myself fighting fiercely to prevent such a facility opening anywhere near where I live.
On the other hand, we can’t very well abandon the homeless. They need a warm place to go along with access to resources necessary for moving ahead with their lives.
One alternative to dorm-like shelters where client concentration can amplify the negative impacts of disturbed behavior is “housing first” models. The goal is to provide clients with immediate and unconditional access to their own apartments regardless of health or behaviour warnings. The thinking is that other issues can only be properly addressed from the foundation of stable housing.
Such models have been tried in many places around the world over the years. Canada’s federal government, for example, ran their Housing First program between 2009 and 2013. That was replaced in 2014 with the Homelessness Partnering Strategy which, in 2019 was followed by Reaching Home.
There have been some successes, particularly in small communities. But one look at the disaster that is San Francisco will demonstrate that the model doesn’t scale well. The sad fact is that Canada’s emergency shelters are still as common as ever: serving as many as 11,000 people a night just in Toronto. Some individuals might have benefited from the Home First-type programs, but they haven’t had a measurable impact on the problem itself.
The Audit is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Where does the money to cover those programs come from? According to their 2023 Financial Report, the City of Toronto spent $1.1 billion on social housing, of which $504 million came in funding transfers from other levels of government. Now we probably have to be careful to distinguish between a range of programs that could be included in those “social housing” figures. But it’s probably safe to assume that they included an awful lot of funding directed at the homeless.
So money is available, but is there another way to spend it that doesn’t involve harming residential neighborhoods?
To ask the question is to answer it. Why not create homeless shelters in non-residential areas?
Right off the top I’ll acknowledge that there’s no guarantee these ideas would work and they’re certainly not perfect. But we already know that the current system isn’t ideal and there’s no indication that it’s bringing us any closer to solving the underlying problems. So why not take a step back and at least talk about alternatives?
Good government is about finding a smart balance between bad options.
Put bluntly, by “non-residential neighborhood shelters” I mean “client warehouses”. That is, constructing or converting facilities in commercial, industrial, or rural areas for dorm-like housing. Naturally, there would be medical, social, and guidance resources available on-site, and frequent shuttle services back and forth to urban hubs.
If some of this sounds suspiciously like the forced institutionalization of people suffering from dangerous mental health conditions that existing until the 1970s, that’s not an accident. The terrible abuses that existed in some of those institutions were replaced by different kinds of suffering, not to mention growing street crime. But shutting down the institutions themselves didn’t solve anything. Involuntary confinement is currently enjoying serious reconsideration.
Clients would face some isolation and inconvenience, and the risk of institutional abuses can’t be ignored. But those could be outweighed by the positives. For one thing, a larger client population makes it possible to properly separate families and healthy individuals facing short-term poverty from the mentally ill or abusive. It would also allow for more resource concentration than community-based models. That might mean dedicated law enforcement and medical staff rather than reliance on the 9-1-1 system.
It would also be possible to build positive pathways into the system, so making good progress in the rural facility could earn clients the right to move to in-town transition locations.
This won’t be the last word spoken on this topic. But we’re living with a system that’s clearly failing to properly serve both the homeless and people living around them. It would be hard to justify ignoring alternatives.
The Audit is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
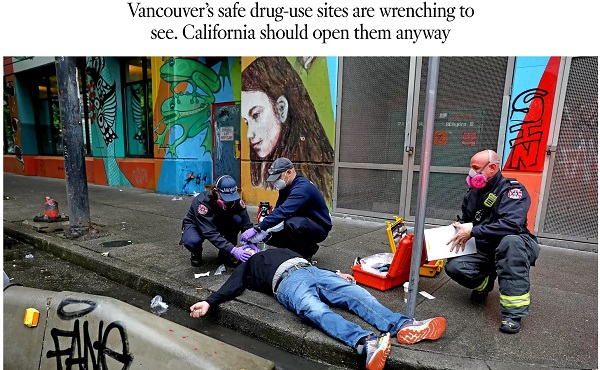
A 2022 Los Angeles Times piece advocates following Vancouver’s model of drug liberalization and treatment. Adam Zivo argues British Columbia’s model has been proven a failure.

By Adam Zivo
Oregon and British Columbia neglected to coerce addicts into treatment.
Ever since Portugal enacted drug decriminalization in 2001, reformers have argued that North America should follow suit. The Portuguese saw precipitous declines in overdoses and blood-borne infections, they argued, so why not adopt their approach?
But when Oregon and British Columbia decriminalized drugs in the early 2020s, the results were so catastrophic that both jurisdictions quickly reversed course. Why? The reason is simple: American and Canadian policymakers failed to grasp what led to the Portuguese model’s initial success.
Contrary to popular belief, Portugal does not allow consequence-free drug use. While the country treats the possession of illicit drugs for personal use as an administrative offense, it nonetheless summons apprehended drug users to “dissuasion” commissions composed of doctors, social workers, and lawyers. These commissions assess a drug user’s health, consumption habits, and socioeconomic circumstances before using arbitrator-like powers to impose appropriate sanctions.
These sanctions depend on the nature of the offense. In less severe cases, users receive warnings, small fines, or compulsory drug education. Severe or repeat offenders, however, can be banned from visiting certain places or people, or even have their property confiscated. Offenders who fail to comply are subject to wage garnishment.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Throughout the process, users are strongly encouraged to seek voluntary drug treatment, with most penalties waived if they accept. In the first few years after decriminalization, Portugal made significant investments into its national addiction and mental-health infrastructure (e.g., methadone clinics) to ensure that it had sufficient capacity to absorb these patients.
This form of decriminalization is far less radical than its North American proponents assume. In effect, Portugal created an alternative justice system that coercively diverts addicts into rehab instead of jail. That users are not criminally charged does not mean they are not held accountable. Further, the country still criminalizes the public consumption and trafficking of illicit drugs.
At first, Portugal’s decriminalization experiment was a clear success. During the 2000s, drug-related HIV infections halved, non-criminal drug seizures surged 500 percent, and the number of addicts in treatment rose by two-thirds. While the data are conflicting on whether overall drug use increased or decreased, it is widely accepted that decriminalization did not, at first, lead to a tidal wave of new addiction cases.
Then things changed. The 2008 global financial crisis destabilized the Portuguese economy and prompted austerity measures that slashed public drug-treatment capacity. Wait times for state-funded rehab ballooned, sometimes reaching a year. Police stopped citing addicts for possession, or even public consumption, believing that the country’s dissuasion commissions had grown dysfunctional. Worse, to cut costs, the government outsourced many of its addiction services to ideological nonprofits that prioritized “harm reduction” services (e.g., distributing clean crack pipes, operating “safe consumption” sites) over nudging users into rehab. These factors gradually transformed the Portuguese system from one focused on recovery to one that enables and normalizes addiction.
This shift accelerated after the Covid-19 pandemic. As crime and public disorder rose, more discarded drug paraphernalia littered the streets. The national overdose rate reached a 12-year high in 2023, and that year, the police chief of the country’s second-largest city told the Washington Post that, anecdotally, the drug problem seemed comparable to what it was before decriminalization. Amid the chaos, some community leaders demanded reform, sparking a debate that continues today.
In North America, however, progressive policymakers seem entirely unaware of these developments and the role that treatment and coercion played in Portugal’s initial success.
In late 2020, Oregon embarked on its own drug decriminalization experiment, known as Measure 110. Though proponents cited Portugal’s success, unlike the European nation, Oregon failed to establish any substantive coercive mechanisms to divert addicts into treatment. The state merely gave drug users a choice between paying a $100 ticket or calling a health hotline. Because the state imposed no penalty for failing to follow through with either option, drug possession effectively became a consequence-free behavior. Police data from 2022, for example, found that 81 percent of ticketed individuals simply ignored their fines.
Additionally, the state failed to invest in treatment capacity and actually defunded existing drug-use-prevention programs to finance Measure 110’s unused support systems, such as the health hotline.
The results were disastrous. Overdose deaths spiked almost 50 percent between 2021 and 2023. Crime and public drug use became so rampant in Portland that state leaders declared a 90-day fentanyl emergency in early 2024. Facing withering public backlash, Oregon ended its decriminalization experiment in the spring of 2024 after almost four years of failure.
The same story played out in British Columbia, which launched a three-year decriminalization pilot project in January 2023. British Columbia, like Oregon, declined to establish dissuasion commissions. Instead, because Canadian policymakers assumed that “destigmatizing” treatment would lead more addicts to pursue it, their new system employed no coercive tools. Drug users caught with fewer than 2.5 grams of illicit substances were simply given a card with local health and social service contacts.
This approach, too, proved calamitous. Open drug use and public disorder exploded throughout the province. Parents complained about the proliferation of discarded syringes on their children’s playgrounds. The public was further scandalized by the discovery that addicts were permitted to smoke fentanyl and meth openly in hospitals, including in shared patient rooms. A 2025 study published in JAMA Health Forum, which compared British Columbia with several other Canadian provinces, found that the decriminalization pilot was associated with a spike in opioid hospitalizations.
The province’s progressive government mostly recriminalized drugs in early 2024, cutting the pilot short by two years. Their motivations were seemingly political, with polling data showing burgeoning support for their conservative rivals.
The lessons here are straightforward. Portugal’s decriminalization worked initially because it did not remove consequences for drug users. It imposed a robust system of non-criminal sanctions to control addicts’ behavior and coerce them into well-funded, highly accessible treatment facilities.
Done right, decriminalization should result in the normalization of rehabilitation—not of drug use. Portugal discovered this 20 years ago and then slowly lost the plot. North American policymakers, on the other hand, never understood the story to begin with.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards


Experts warn surging THC levels are fuelling growing health risks — and say stronger regulation is urgently needed
More and more cannabis users are ending up in emergency rooms suffering from severe, repeated bouts of vomiting — a condition known as cannabis hyperemesis syndrome.
A new study found that emergency visits for cannabis hyperemesis syndrome increased 13-fold over eight years, accounting for more than 8,000 of the nearly 13,000 cannabis-related ER visits in that period.
Experts say the mounting health risks associated with cannabis use are due to rising THC levels in cannabis products. They urge stronger regulation, better labeling and more research — using Quebec’s approach as a potential model.
“I don’t think we have the perfect model in Quebec — there’s pros and cons,” said Dr. Didier Jutras-Aswad, a clinical scientist at the Centre hospitalier de l’Université de Montréal (CHUM) and a professor in the Department of Psychiatry and Addiction at Université de Montréal.
“But overall, the process of … progressively implementing changes, not wanting to be the first one in line to put all this new product on the market, I think is probably, in terms of public health, more prudent.”
THC levels
Tetrahydrocannabinol (THC) is the primary psychoactive compound in cannabis and what causes the “high.” It is one of more than 100 cannabinoids, or chemical compounds, naturally found in the cannabis plant.
Delta‑9‑THC is the most common and well-studied form, though other forms of THC exist and are less understood.
Federal drug laws place strict limits on delta-9-THC levels. They cap delta-9-THC at 10 milligrams per piece for edibles, and 1,000 milligrams per container for extracts and topicals. Dried cannabis flower and pre-rolled joints have no THC cap, but must disclose the THC level on their labels.
Other intoxicating cannabinoids — like delta-8-THC — are not regulated the same way. Some producers use these other cannabinoids to get around delta-9 limits to make their products more potent.
In 2023, Health Canada issued guidance warning against this practice, noting it could lead to inspections and regulatory action. Its guidance is not legally binding.
“Good weed”
Dr. Oyedeji Ayonrinde, a professor of psychiatry and psychology at Queen’s University, says “good weed” used to mean a product did not contain pesticides or contaminants. Now, it often means a product is high-THC — reinforcing the risky idea that stronger is better.
“We would say, Oh, man, that guy’s got good weed,’ because it’s 30 per cent [THC],” he said.
Today, THC levels average about 25 per cent — up from about four per cent in the 1960s. But some products go as high as 80 or 90 per cent THC.
“That’s ‘the good stuff,’” said Ayonrinde, referring to how consumers view products with these elevated levels of THC.
“One of the major [health] risk factors is the use of cannabis with higher than 10 per cent THC,” said Dr. Daniel Myran, a physician and Canada Research Chair at the University of Ottawa.
Myran led three Canadian studies this year linking heavy cannabis use to health risks such as schizophrenia, dementia and early death.
Chris Blair, a Canadian originally from Jamaica, says the cannabis he once smoked — natural, Jamaican, homegrown weed known as “sess” — was much milder than what is available through Ontario dispensaries today.
“We grew it, it was natural … the regular Mary Jane sess,” he said. “And then times changed … the sess was pushed to almost become the hydro[ponic] type of thing.”
Hydroponic growing methods produce more potent cannabis with higher THC levels. Blair says he could no longer go back to Jamaican sess, because he had built up a tolerance to it.
“Unfortunately, going back to sess was not the same, because it wasn’t the same high or same strength,” he said.
“Back when [I was] smoking [Jamaican sess] … I’d finished that spliff and we were ready to go hang out, we’re ready to party.
“Nowadays, after you smoke you’re mashed and you’re not doing anything.”
Greening out
Ayonrinde says higher THC levels can alter how the brain’s dopamine receptors work, which may induce paranoia.
“Being out of touch with reality, auditory hallucinogens, delusional thoughts, disorganized thinking — that’s part of the mechanism pathway for the development of a severe and enduring mental illness [like] schizophrenia,” he said.
High THC can also worsen anxiety, disrupt sleep, affect mood and trigger psychosis, he says. Other experts cited risks including cannabis use disorder, mental health issues, and dizziness or nausea — sometimes referred to as “greening out.”
Young people, whose brains are still developing until age 25, are most vulnerable to these harmful effects, Ayonrinde says.
During adolescence, the brain undergoes intense growth. “Think of the brain like a construction site,” he said. Frequent, high-dose THC use during this critical period can disrupt dopamine systems and increase the risk of building scaffolding for serious mental health conditions.
While some literature suggests that cannabidiol (CBD) — another major cannabinoid in most cannabis products — may act as a calming, non-psychoactive counterbalance to THC, Ayonrinde says this is only true at extremely high doses, around 6,000 mg.
Standard measurement
Experts say the diversity of cannabis products on the market is part of the challenge.
“When people say, ‘Weed helps me with my trauma,’ an example I often give is: cannabis is just like saying ‘dog’,” said Ayonrinde.
“What breed? Is it a chihuahua or a rottweiler or a great dane? Because without knowing exactly the THC, CBD … what are you talking about?
“There’s no single cannabis.”
Cannabis products lack clear dosage guidelines, and Ayonrinde says marketing messages push consumers to opt for high potency options.
Ruth Ross, a professor of pharmacology and toxicology at the University of Toronto, would like Canada to adopt a standard unit of measurement for THC levels, so consumers could easily understand what one unit means.
“Say a unit was one milligram; they could multiply that up — it’s easy math,” she said.
Myran agrees. “The way we sell alcohol in this country is not set up so that you pay the same amount for a litre of wine as you do for a litre of vodka,” said Myran.
“You have a minimum price per unit of ethanol … and there’s a really compelling reason to price cannabis according to its THC content … [to] financially discourage people from always moving to the highest potency THC products.”
Ross says there is also a need for more current cannabis research. Most cannabis research evaluates the effects of cannabis products with much lower THC levels than those seen on the market today. Long-term health effects can take decades to appear — similar to tobacco.
“Some of [the health harms] might emerge over many, many years, and we don’t know what those will be until data comes in,” she said.
Quebec’s approach
Ross points to Quebec as a unique model in cannabis regulation. It is the only province that caps THC potency and tightly controls how cannabis can be marketed. For example, edibles resembling candy or desserts are prohibited.
Jutras-Aswad, of the Université de Montréal, says overly strict rules can drive some consumers — especially those younger than the province’s legal age of 21 — to the black market.
Still, he says Quebec’s model offers benefits, including greater control over sales and a public health approach focused on harm reduction rather than profit.
Under Quebec’s Cannabis Regulation Act, the Société québécoise du cannabis (SQDC) is the only authorized cannabis retailer in the province.
SQDC employees are trained to offer science-based information, connect consumers with support services and promote safer use.
Researchers in Ontario are now studying how Quebec’s stricter THC limits may be affecting cannabis-related harms compared to other provinces.
“That’s going to be a really interesting within-Canada experiment,” said Ross.
Myran recommends adopting Quebec’s 30 per cent THC caps nationwide.
He also recommends better product labelling requirements and a pricing model that sets a minimum price per unit of THC — to discourage the purchase of high-potency products.
In a 2023 op-ed, Ross argued provinces should fund cannabis research to guide policy and public health.
In it, she notes that Quebec reinvested all $95 million of its 2022 revenue from cannabis sales into prevention and research. By contrast, Ontario set aside just 0.1% of its $170 million in cannabis revenue for a Social Impact Fund that has no clear public health focus.
“Canada can do so much better. We have world experts in cannabis research from coast-to-coast, and we are uniquely positioned to have high-quality, well-funded research on its medical use and potential harms,” she wrote.
“Five years from now, will we be dealing with major public health challenges that could have been avoided?”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards

Province urging post secondary students to apply for loans, grants, scholarships, bursaries and awards

Poilievre: “Carney More Irresponsible Than Trudeau” as Housing, Jobs, and Energy Failures Mount

Breaking: ‘Catch This Fascist’: Radicalized Utah Suspect Arrested in Charlie Kirk Assassination, Officials Say

Former NYPD Inspector Shares What Family Of Alleged Charlie Kirk Assassin Feared Before Turning Him In
-
 espionage2 days ago
espionage2 days agoInside Xi’s Fifth Column: How Beijing Uses Gangsters to Wage Political Warfare in Taiwan — and the West
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoDecision expected soon in case that challenges Alberta’s “safe spaces” law
-
 International2 days ago
International2 days agoBrazil sentences former President Bolsonaro to 27 years behind bars
-
 Energy1 day ago
Energy1 day agoThe IEA’s Peak Oil Fever Dream Looks To Be In Full Collapse
-
 Crime1 day ago
Crime1 day agoTransgender Roomate of Alleged Charlie Kirk Assassin Cooperating with Investigation
-
 COVID-191 day ago
COVID-191 day agoWhy FDA Was Right To Say No To COVID-19 Vaccines For Healthy Kids
-
 Crime19 hours ago
Crime19 hours agoDown the Charlie Kirk Murder Rabbit Hole
-
 Business16 hours ago
Business16 hours agoIt’s time to finally free the beer