National
Medical Assistance in Dying now accounts for over 4% of deaths in Canada
The following are interesting statistics pulled directly from the:
Fourth annual report on Medical Assistance in Dying in Canada 2022
Growth in the number of medically assisted deaths in Canada continues in 2022.
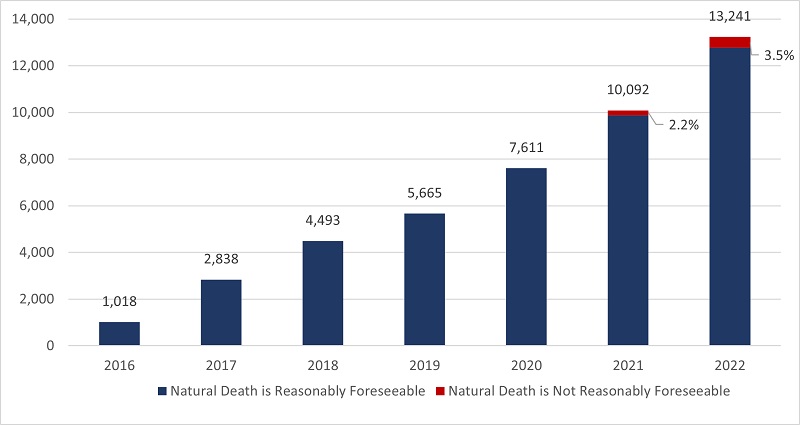
- In 2022, there were 13,241 MAID provisions reported in Canada, accounting for 4.1% of all deaths in Canada.
- The number of cases of MAID in 2022 represents a growth rate of 31.2% over 2021. All provinces except Manitoba and the Yukon continue to experience a steady year-over-year growth in 2022.
- When all data sources are considered, the total number of medically assisted deaths reported in Canada since the introduction of federal MAID legislation in 2016 is 44,958.
Profile of MAID recipients
- In 2022, a slightly larger proportion of males (51.4%) than females (48.6%) received MAID. This result is consistent with 2021 (52.3% males and 47.7% females), 2020 (51.9% males and 48.1% females) and 2019 (50.9% males and 49.1% females).
- The average age of individuals at the time MAID was provided in 2022 was 77.0 years. This average age is slightly higher than the averages of 2019 (75.2), 2020 (75.3) and 2021 (76.3). The average age of females during 2022 was 77.9, compared to males at 76.1.
- Cancer (63.0%) is the most cited underlying medical condition among MAID provisions in 2022, down from 65.6% in 2021 and from a high of 69.1% in 2020. This is followed by cardiovascular conditions (18.8%), other conditions (14.9%), respiratory conditions (13.2%) and neurological conditions (12.6%).
- In 2022, 3.5% of the total number of MAID provisions (463 individuals), were individuals whose natural deaths were not reasonably foreseeable. This is an increase from 2.2% in 2021 (223 individuals). The most cited underlying medical condition for this population was neurological (50.0%), followed by other conditions (37.1%), and multiple comorbidities (23.5%), which is similar to 2021 results. The average age of individuals receiving MAID whose natural death was not reasonably foreseeable was 73.1 years, slightly higher than 70.1 in 2021 but lower than the average age of 77.0 for all MAID recipients in 2022.
Nature of suffering among MAID recipients
- In 2022, the most commonly cited sources of suffering by individuals requesting MAID were the loss of ability to engage in meaningful activities (86.3%), followed by loss of ability to perform activities of daily living (81.9%) and inadequate control of pain, or concern about controlling pain (59.2%).
- These results continue to mirror very similar trends seen in the previous three years (2019 to 2021), indicating that the nature of suffering that leads a person to request MAID has remained consistent over the past four years.
Eligibility Criteria
- Request MAID voluntarily
- 18 years of age or older
- Capacity to make health care decisions
- Must provide informed consent
- Eligible for publicly funded health care services in Canada
- Diagnosed with a “grievous and irremediable medical condition,” where a person must meet all of the following criteria:
- serious and incurable illness, disease or disability
- advanced state of irreversible decline in capability,
- experiencing enduring physical or psychological suffering that is caused by their illness, disease or disability or by the advanced state of decline in capability, that is intolerable to them and that cannot be relieved under conditions that they consider acceptable
- Mental Illness as sole underlying medical condition is excluded until March 17, 2024
3.1 Number of Reported MAID Deaths in Canada (2016 to 2022)
2022 marks six and a half years of access to MAID in Canada. In 2022, there were 13,241 MAID provisions in Canada, bringing the total number of medically assisted deaths in Canada since 2016 to 44,958. In 2022, the total number of MAID provisions increased by 31.2% (2022 over 2021) compared to 32.6% (2021 over 2020). The annual growth rate in MAID provisions has been steady over the past six years, with an average growth rate of 31.1% from 2019 to 2022.

Access to MAID for individuals whose deaths were not reasonably foreseeable marked its second year of eligibility in 2022. In Canada, eligibility for individuals whose death is not reasonably foreseeable began on March 17, 2021, after the passage of the new legislation.Footnote8 There were 463 MAID provisions for persons whose natural death was not reasonably foreseeable, representing 3.5% of all MAID deaths in 2022. This is just over twice the total number of provisions for individuals where natural death was not reasonably foreseeable in 2021 (223 provisions representing 2.2% of all MAID provisions in 2021). Table 3.1 represents total MAID provisions in Canada from 2016 to 2022, including provisions for individuals where natural death was not reasonably foreseeable.
All jurisdictions, except Manitoba and Yukon, experienced growth in MAID provisions in 2022. The highest percentage year over year increases occurred in Québec (45.5%), Alberta (40.7%), Newfoundland and Labrador (38.5%), Ontario (26.8%) and British Columbia (23.9%). Nova Scotia (11.8%), Prince Edward Island (7.3%) and Saskatchewan (4.0%) had lower growth rates. The Yukon remained at the same level as 2021, while Manitoba was the only jurisdiction to experience a decline in MAID provisions for 2022 (-9.0%).
| MAID | NL | PE | NS | NB | QC | ON | MB | SK | AB | BC | YT | NT | NU | Canada |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2016 | – | – | 24 | 9 | 494 | 191 | 24 | 11 | 63 | 194 | – | – | – | 1,018 |
| 2017 | – | – | 62 | 49 | 853 | 839 | 63 | 57 | 205 | 677 | – | – | – | 2,838 |
| 2018 | 23 | 8 | 126 | 92 | 1,249 | 1,500 | 138 | 85 | 307 | 951 | 12 | – | – | 4,493 |
| 2019 | 20 | 20 | 147 | 141 | 1,604 | 1,788 | 177 | 97 | 377 | 1,280 | 13 | – | – | 5,665 |
| 2020 | 49 | 37 | 190 | 160 | 2,278 | 2,378 | 214 | 160 | 555 | 1,572 | 13 | – | – | 7,611 |
| 2021 | 65 | 41 | 245 | 205 | 3,299 | 3,102 | 245 | 247 | 594 | 2,030 | 16 | – | – | 10,092 |
| 2022 | 90 | 44 | 274 | 247 | 4,801 | 3,934 | 223 | 257 | 836 | 2,515 | 16 | – | – | 13,241 |
| TOTAL 2016-2022 |
267 | 156 | 1,068 | 903 | 14,578 | 13,732 | 1,084 | 914 | 2,937 | 9,219 | 84 | – | – | 44,958 |
3.2 MAID Deaths as a Proportion of Total Deaths in Canada
MAID deaths accounted for 4.1% of all deaths in Canada in 2022, an increase from 3.3% in 2021, 2.5% in 2020 and 2.0% in 2019. In 2022, six jurisdictions continue to experience increases in the number of MAID provisions as a percentage of total deaths, ranging from a low of 1.5% (Newfoundland & Labrador) to a high of 6.6% (Québec). MAID deaths as a percentage of total deaths remained at the same levels as 2021 for Prince Edward Island, Nova Scotia, and Saskatchewan, while Manitoba experienced a decline in MAID deaths as a percentage of all deaths (from 2.1% in 2021 to 1.8% in 2022). As with each of the three previous years (2019 to 2021), Québec and British Columbia experienced the highest percentage of MAID deaths as a proportion of all deaths within their jurisdiction in 2022 (6.6% and 5.5% respectively), continuing to reflect the socio-political dynamics of these two jurisdictions in the context of MAID.
4.5 Profile of Persons Receiving MAID Whose Natural Death is not Reasonably Foreseeable
2022 marks the second year that MAID for persons whose natural death is not reasonably foreseeable is permitted under the law if all other eligibility criteria are met (Table 1.1). New federal MAID legislation passed on March 17, 2021, created a two-track approach to procedural safeguards for MAID practitioners to follow, based on whether or not a person’s natural death is reasonably foreseeable. This approach to safeguards ensures that sufficient time and expertise are spent assessing MAID requests from persons whose natural death is not reasonably foreseeable. New and enhanced safeguards (Table 1.2), including a minimum 90-day assessment period, seek to address the diverse source of suffering and vulnerability that could potentially lead a person who is not nearing death to ask for MAID and to identify alternatives to MAID that could reduce suffering.
In 2022, 3.5% of MAID recipients (463 individuals) were assessed as not having a reasonably foreseeable natural death, up slightly from 2.2% (223 individuals) in 2021. As a percentage of all MAID deaths in Canada, MAID for individuals whose natural death is not reasonably foreseeable represents just 0.14% of all deaths in Canada in 2022 (compared to all MAID provisions, which represent 4.1% of all 2022 deaths in Canada). The proportion of MAID recipients whose natural death was not reasonably foreseeable continues to remain very small compared to the total number of MAID recipients.
This population of individuals whose natural death was not reasonably foreseeable have a different medical profile than individuals whose death was reasonably foreseeable. As shown in Chart 4.5A, the main underlying medical condition reported in the population whose natural death was not reasonably foreseeable was neurological (50.0%), followed by ‘other condition’ (37.1%), and multiple comorbidities (23.5%). This differs from the main condition (as reported in Chart 4.1A) for all MAID recipients in 2022, where the majority of persons receiving MAID had cancer as a main underlying medical condition (63.0%), followed by cardiovascular conditions (18.8%) and other conditions (14.9%) (such as chronic pain, osteoarthritis, frailty, fibromyalgia, autoimmune conditions). These results are similar to 2021.

Of the MAID provisions for individuals where death was reasonably foreseeable, the majority were individuals ages 71 and older (71.1%) while only 28.9% were between ages 18-70. A similar trend was observed for individuals where natural death was not reasonably foreseeable which also showed a greater percentage of individuals who received MAID being 71 and older (58.5%) and a lower number of MAID provisions for individuals between 18-70 years (41.5%). Overall, however, MAID provisions for individuals whose death is not reasonably foreseeable tended to be in the younger age categories than those where natural death is foreseeable.



[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research]
By Adam Zivo
A Canadian poll finds that racial minorities don’t believe drug enforcement is bigoted.
Is drug prohibition racist? Many left-wing institutions seem to think so. But their argument is historically illiterate—and it contradicts recent polling data, too, which show that minorities overwhelmingly reject that view.
Policies and laws are tools to establish order. Like any tool, they can be abused. The first drug laws in North America, dating back to the late nineteenth and early twentieth centuries, arguably fixated on opium as a legal pretext to harass Asian immigrants, for example. But no reasonable person would argue that laws against home invasion, murder, or theft are “racist” because they have been misapplied in past cases. Absent supporting evidence, leaping from “this tool is sometimes used in racist ways” to “this tool is essentially racist” is kindergarten-level reasoning.
Yet this is precisely what institutions and activist groups throughout the Western world have done. The Drug Policy Alliance, a U.S.-based organization, suggests that drug prohibition is rooted in “racism and fear.” Harm Reduction International, a British NGO, argues for legalization on the grounds that drug prohibition entrenches “racialized hierarchies, which were established under colonial control and continue to dominate today.” In Canada, where I live, the top public health official in British Columbia, our most drug-permissive province, released a pro-legalization report last summer claiming that prohibition is “based on a history of racism, white supremacy, paternalism, colonialism, classism and human rights violations.”
These claims ignore how drug prohibition has been and remains popular in many non-European societies. Sharia law has banned the use of mind-altering substances since the seventh century. When Indigenous leaders negotiated treaties with Canadian colonists in the late 1800s, they asked for “the exclusion of fire water (whiskey)” from their communities. That same century, China’s Qing Empire banned opium amid a national addiction crisis. “Opium is a poison, undermining our good customs and morality,” the Daoguang emperor wrote in an 1810 edict.
Today, Asian and Muslim jurisdictions impose much stiffer penalties on drug offenders than do Western nations. In countries like China, Saudi Arabia, Iran, Singapore, and Thailand, addicts and traffickers are given lengthy prison sentences or executed. Meantime, in Canada and the United States, de facto decriminalization has left urban cores littered with syringes and shrouded in clouds of meth.
The anti-drug backlash building in North America appears to be spearheaded by racial minorities. When Chesa Boudin, San Francisco’s former district attorney, was recalled in 2022, support for his ouster was highest among Asian voters. Last fall, 73 percent of Latinos backed California’s Proposition 36, which heightened penalties for drug crimes, while only 58 percent of white respondents did.
In Canada, the first signs of a parallel trend emerged during Vancouver’s 2022 municipal election, where an apparent surge in Chinese Canadian support helped install a slate of pro-police candidates. Then, in British Columbia’s provincial election last autumn, nonwhite voters strongly preferred the BC Conservatives, who campaigned on stricter drug laws. And in last month’s federal election, within both Vancouver and Toronto’s metropolitan areas, tough-on-crime conservatives received considerable support from South Asian communities.
These are all strong indicators that racial minorities do not, in fact, universally favor drug legalization. But their small population share means there is relatively little polling data to measure their preferences. Since only 7.6 percent of Americans are Asian, for example, a poll of 1,000 randomly selected people will yield an average of only 76 Asian respondents—too small a sample from which to draw meaningful conclusions. You can overcome this barrier by commissioning very large polls, but that’s expensive.
Nonetheless, last autumn, the Centre for Responsible Drug Policy (a nonprofit I founded and operate) did just that. In partnership with the Macdonald-Laurier Institute, we contracted Mainstreet Research to ask over 12,000 British Columbians: “Do you agree or disagree that criminalizing drugs is racist?”
The results undermine progressives’ assumptions. Only 26 percent of nonwhite respondents agreed (either strongly or weakly) that drug criminalization is racist, while over twice as many (56 percent) disagreed. The share of nonwhite respondents who strongly disagreed was three times larger than the share that strongly agreed (43.2 percent versus 14.3 percent). These results are fairly conclusive for this jurisdiction, given the poll’s sample size of 2,233 nonwhite respondents and a margin of error of 2 percent.
Notably, Indigenous respondents seemed to be the most anti-drug ethnic group: only 20 percent agreed (weakly or strongly) with the “criminalization is racist” narrative, while 61 percent disagreed. Once again, those who disagreed were much more vehement than those who agreed. With a sample size of 399 respondents, the margin of error here (5 percent) is too small to confound these dramatic results.
We saw similar outcomes for other minority groups, such as South Asians, Southeast Asians, Latinos, and blacks. While Middle Eastern respondents also seemed to follow this trend, the poll included too few of them to draw definitive conclusions. Only East Asians were divided on the issue, though a clear majority still disagreed that criminalization is racist.
As this poll was limited to British Columbian respondents, our findings cannot necessarily be assumed to hold throughout Canada and the United States. But since the province is arguably the most drug-permissive jurisdiction within the two countries, these results could represent the ceiling of pro-drug, anti-criminalization attitudes among minority communities.
Legalization proponents and their progressive allies take pride in being “anti-racist.” Our polling, however, suggests that they are not listening to the communities they profess to care about.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards

![]()
The 21 st century is going to be overshadowed by a crisis that human beings have never faced before. I don’t mean war, pestilence, famine or climate change. Those are perennial troubles. Yes, even climate change, despite the hype, is nothing new as anyone who’s heard of the Roman Warm Period, the Mediaeval Warm Period or the Little Ice Age will know. Climate change and the others are certainly problems, but they aren’t new.
But the crisis that’s coming is new.
The global decline in fertility rates has grown so severe that some demographers now talk about “peak humanity” – a looming maximum from which the world’s population will begin to rapidly decline. Though the doomsayers who preach the dangers of overpopulation may think that’s a good development, it is in fact a grave concern.
In the Canadian context, it is doubly worrisome. Our birth rates have been falling steadily since 1959. It was shortly after that in the 1960s when we began to build a massive welfare state, and we did so despite a shrinking domestically-born population and the prospect of an ever-smaller pool of taxable workers to pay for the expanding social programs.
Immigration came to the rescue, and we became adept at recruiting a surplus population of young, skilled, economically focused migrants seeking their fortune abroad. The many newcomers meant a growing population and with it a larger tax base.
But what would happen if Canada could no longer depend on a steady influx of newcomers? The short answer is that our population would shrink, and our welfare state would come under intolerable strain. The long answer is that Canadian businesses, which have become addicted to abundant, cheap foreign labour through the Temporary Foreign Worker Program, would be obliged to invest in hiring, training and retaining Canadian workers.
Provincial and federal governments would scramble to keep older Canadians in the workforce for longer. And governments would be torn between demands to cut the welfare state or privatize large parts of it while raising taxes to help pay for it.
No matter what, the status quo won’t continue. And – even though Canada is right now taking in record numbers of new immigrants and temporary workers – we are going to discover this soon. The main cause is the “peak humanity” that I mentioned before. Fertility rates are falling rapidly nearly everywhere. In the industrialized West, births have fallen further in some places than in others, but all countries are now below replacement levels
(except Israel, which was at 2.9 in 2020).
Deaths have long been outpacing births in China, Japan and some Western countries like Italy. A recent study in The Lancet expects that by 2100, 97 percent of countries will be shrinking. Only Western and Eastern sub-Saharan Africa will have birth rates above replacement levels, though births will be falling in those regions also.
In a world of sub-replacement fertility, there will still be well-educated, highly skilled people abroad. But there will not be a surplus of them. Some may still be ready and willing to put down roots in Canada, but the number will soon be both small and dwindling. And it seems likely that countries which have produced Canada’s immigrants in recent years will try hard to retain domestic talent as their own populations decline. In contrast, the population of sub-Saharan Africa will be growing for a little longer. But unless education and skills-training change drastically in that region, countries there will not produce the kind of skilled immigrants that Canada has come to rely on.
And so the moment is rapidly approaching when immigration will no longer be able to make up for falling Canadian fertility. Governments will have to confront the problem directly—not years or decades hence, but now.
While many will cite keeping the welfare state solvent as the driving force, in my view this is not the reason to do it. The reason to do it is that it is in Canada’s national interest to make it easier for families to have the number of children that they want. A 2023 study by the think-tank Cardus found that nearly half of Canadian women at the end of their reproductive years had fewer children than they had wanted. This amounted to an average
of 0.5 fewer children per woman – a shortfall that would lift Canada close to replacement level.
The United Nations Population Fund (UNPF) has noticed the same challenge on a global scale. Neither Cardus nor the UNPF prescribes any specific solutions, but their analysis points to the same thing: public policy should focus on identifying and removing barriers families face to having the number of children they want.
Every future government should be vigilant against impediments to family-formation and raising a desired number of children. Making housing more abundant and affordable would surely be a good beginning. Better planning must go into making livable communities (not merely atomized dwellings) with infrastructure favouring families and designed to ease commuting. But more fundamentally, policy-makers will need to ask and answer an uncomfortable question: why did we allow barriers to fertility to arise in the first place?
The original, full-length version of this article was recently published in C2C Journal.
Michael Bonner is a political consultant with Atlas Strategic Advisors, LLC, contributing editor to the Dorchester Review, and author of In Defense of Civilization: How Our Past Can Renew Our Present.

RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Blind to the Left: Canada’s Counter-Extremism Failure Leaves Neo-Marxist and Islamist Threats Unchecked

Why it’s time to repeal the oil tanker ban on B.C.’s north coast
Alberta Provincial Police – New chief of Independent Agency Police Service
-
 Agriculture2 days ago
Agriculture2 days agoCanada’s supply management system is failing consumers
-
 Alberta1 day ago
Alberta1 day agoAlberta uncorks new rules for liquor and cannabis
-
 Energy20 hours ago
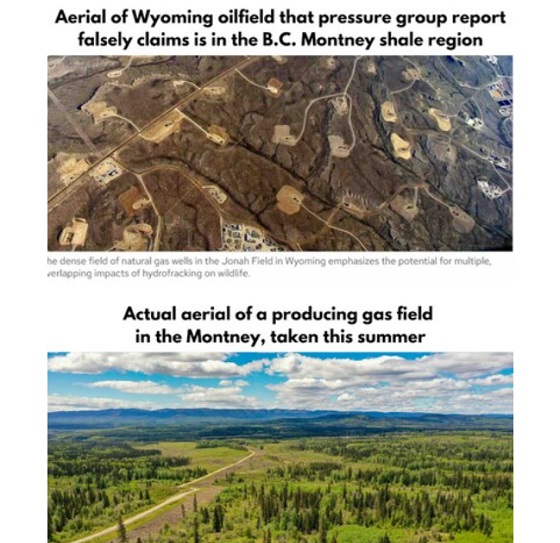
Energy20 hours agoB.C. Residents File Competition Bureau Complaint Against David Suzuki Foundation for Use of False Imagery in Anti-Energy Campaigns
-
 COVID-1920 hours ago
COVID-1920 hours agoCourt compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts
-
 Crime1 day ago
Crime1 day agoProject Sleeping Giant: Inside the Chinese Mercantile Machine Linking Beijing’s Underground Banks and the Sinaloa Cartel
-
 International1 day ago
International1 day agoTrump transportation secretary tells governors to remove ‘rainbow crosswalks’
-
 Alberta24 hours ago
Alberta24 hours agoAlberta Next: Alberta Pension Plan
-
C2C Journal17 hours ago
Canada Desperately Needs a Baby Bump