Brownstone Institute
Bizarre Decisions about Nicotine Pouches Lead to the Wrong Products on Shelves

From the Brownstone Institute

A walk through a dozen convenience stores in Montgomery County, Pennsylvania, says a lot about how US nicotine policy actually works. Only about one in eight nicotine-pouch products for sale is legal. The rest are unauthorized—but they’re not all the same. Some are brightly branded, with uncertain ingredients, not approved by any Western regulator, and clearly aimed at impulse buyers. Others—like Sweden’s NOAT—are the opposite: muted, well-made, adult-oriented, and already approved for sale in Europe.
Yet in the United States, NOAT has been told to stop selling. In September 2025, the Food and Drug Administration (FDA) issued the company a warning letter for offering nicotine pouches without marketing authorization. That might make sense if the products were dangerous, but they appear to be among the safest on the market: mild flavors, low nicotine levels, and recyclable paper packaging. In Europe, regulators consider them acceptable. In America, they’re banned. The decision looks, at best, strange—and possibly arbitrary.
What the Market Shows
My October 2025 audit was straightforward. I visited twelve stores and recorded every distinct pouch product visible for sale at the counter. If the item matched one of the twenty ZYN products that the FDA authorized in January, it was counted as legal. Everything else was counted as illegal.
Two of the stores told me they had recently received FDA letters and had already removed most illegal stock. The other ten stores were still dominated by unauthorized products—more than 93 percent of what was on display. Across all twelve locations, about 12 percent of products were legal ZYN, and about 88 percent were not.
The illegal share wasn’t uniform. Many of the unauthorized products were clearly high-nicotine imports with flashy names like Loop, Velo, and Zimo. These products may be fine, but some are probably high in contaminants, and a few often with very high nicotine levels. Others were subdued, plainly meant for adult users. NOAT was a good example of that second group: simple packaging, oat-based filler, restrained flavoring, and branding that makes no effort to look “cool.” It’s the kind of product any regulator serious about harm reduction would welcome.
Enforcement Works
To the FDA’s credit, enforcement does make a difference. The two stores that received official letters quickly pulled their illegal stock. That mirrors the agency’s broader efforts this year: new import alerts to detain unauthorized tobacco products at the border (see also Import Alert 98-06), and hundreds of warning letters to retailers, importers, and distributors.
But effective enforcement can’t solve a supply problem. The list of legal nicotine-pouch products is still extremely short—only a narrow range of ZYN items. Adults who want more variety, or stores that want to meet that demand, inevitably turn to gray-market suppliers. The more limited the legal catalog, the more the illegal market thrives.
Why the NOAT Decision Appears Bizarre
The FDA’s own actions make the situation hard to explain. In January 2025, it authorized twenty ZYN products after finding that they contained far fewer harmful chemicals than cigarettes and could help adult smokers switch. That was progress. But nine months later, the FDA has approved nothing else—while sending a warning letter to NOAT, arguably the least youth-oriented pouch line in the world.
The outcome is bad for legal sellers and public health. ZYN is legal; a handful of clearly risky, high-nicotine imports continue to circulate; and a mild, adult-market brand that meets European safety and labeling rules is banned. Officially, NOAT’s problem is procedural—it lacks a marketing order. But in practical terms, the FDA is punishing the very design choices it claims to value: simplicity, low appeal to minors, and clean ingredients.
This approach also ignores the differences in actual risk. Studies consistently show that nicotine pouches have far fewer toxins than cigarettes and far less variability than many vapes. The biggest pouch concerns are uneven nicotine levels and occasional traces of tobacco-specific nitrosamines, depending on manufacturing quality. The serious contamination issues—heavy metals and inconsistent dosage—belong mostly to disposable vapes, particularly the flood of unregulated imports from China. Treating all “unauthorized” products as equally bad blurs those distinctions and undermines proportional enforcement.
A Better Balance: Enforce Upstream, Widen the Legal Path
My small Montgomery County survey suggests a simple formula for improvement.
First, keep enforcement targeted and focused on suppliers, not just clerks. Warning letters clearly change behavior at the store level, but the biggest impact will come from auditing distributors and importers, and stopping bad shipments before they reach retail shelves.
Second, make compliance easy. A single-page list of authorized nicotine-pouch products—currently the twenty approved ZYN items—should be posted in every store and attached to distributor invoices. Point-of-sale systems can block barcodes for anything not on the list, and retailers could affirm, once a year, that they stock only approved items.
Third, widen the legal lane. The FDA launched a pilot program in September 2025 to speed review of new pouch applications. That program should spell out exactly what evidence is needed—chemical data, toxicology, nicotine release rates, and behavioral studies—and make timely decisions. If products like NOAT meet those standards, they should be authorized quickly. Legal competition among adult-oriented brands will crowd out the sketchy imports far faster than enforcement alone.
The Bottom Line
Enforcement matters, and the data show it works—where it happens. But the legal market is too narrow to protect consumers or encourage innovation. The current regime leaves a few ZYN products as lonely legal islands in a sea of gray-market pouches that range from sensible to reckless.
The FDA’s treatment of NOAT stands out as a case study in inconsistency: a quiet, adult-focused brand approved in Europe yet effectively banned in the US, while flashier and riskier options continue to slip through. That’s not a public-health victory; it’s a missed opportunity.
If the goal is to help adult smokers move to lower-risk products while keeping youth use low, the path forward is clear: enforce smartly, make compliance easy, and give good products a fair shot. Right now, we’re doing the first part well—but failing at the second and third. It’s time to fix that.
Author


From the Brownstone Institute

Cigarettes kill nearly half a million Americans each year. Everyone knows it, including the Food and Drug Administration. Yet while the most lethal nicotine product remains on sale in every gas station, the FDA continues to block or delay far safer alternatives.
Nicotine pouches—small, smokeless packets tucked under the lip—deliver nicotine without burning tobacco. They eliminate the tar, carbon monoxide, and carcinogens that make cigarettes so deadly. The logic of harm reduction couldn’t be clearer: if smokers can get nicotine without smoke, millions of lives could be saved.
Sweden has already proven the point. Through widespread use of snus and nicotine pouches, the country has cut daily smoking to about 5 percent, the lowest rate in Europe. Lung-cancer deaths are less than half the continental average. This “Swedish Experience” shows that when adults are given safer options, they switch voluntarily—no prohibition required.
In the United States, however, the FDA’s tobacco division has turned this logic on its head. Since Congress gave it sweeping authority in 2009, the agency has demanded that every new product undergo a Premarket Tobacco Product Application, or PMTA, proving it is “appropriate for the protection of public health.” That sounds reasonable until you see how the process works.
Manufacturers must spend millions on speculative modeling about how their products might affect every segment of society—smokers, nonsmokers, youth, and future generations—before they can even reach the market. Unsurprisingly, almost all PMTAs have been denied or shelved. Reduced-risk products sit in limbo while Marlboros and Newports remain untouched.
Only this January did the agency relent slightly, authorizing 20 ZYN nicotine-pouch products made by Swedish Match, now owned by Philip Morris. The FDA admitted the obvious: “The data show that these specific products are appropriate for the protection of public health.” The toxic-chemical levels were far lower than in cigarettes, and adult smokers were more likely to switch than teens were to start.
The decision should have been a turning point. Instead, it exposed the double standard. Other pouch makers—especially smaller firms from Sweden and the US, such as NOAT—remain locked out of the legal market even when their products meet the same technical standards.
The FDA’s inaction has created a black market dominated by unregulated imports, many from China. According to my own research, roughly 85 percent of pouches now sold in convenience stores are technically illegal.
The agency claims that this heavy-handed approach protects kids. But youth pouch use in the US remains very low—about 1.5 percent of high-school students according to the latest National Youth Tobacco Survey—while nearly 30 million American adults still smoke. Denying safer products to millions of addicted adults because a tiny fraction of teens might experiment is the opposite of public-health logic.
There’s a better path. The FDA should base its decisions on science, not fear. If a product dramatically reduces exposure to harmful chemicals, meets strict packaging and marketing standards, and enforces Tobacco 21 age verification, it should be allowed on the market. Population-level effects can be monitored afterward through real-world data on switching and youth use. That’s how drug and vaccine regulation already works.
Sweden’s evidence shows the results of a pragmatic approach: a near-smoke-free society achieved through consumer choice, not coercion. The FDA’s own approval of ZYN proves that such products can meet its legal standard for protecting public health. The next step is consistency—apply the same rules to everyone.
Combustion, not nicotine, is the killer. Until the FDA acts on that simple truth, it will keep protecting the cigarette industry it was supposed to regulate.
Author


From the Brownstone Institute

Way back in the B.C. era (Before Covid), I taught Medical Humanities and Bioethics at an American medical school. One of my older colleagues – I’ll call him Dr. Quinlan – was a prominent member of the faculty and a nationally recognized proponent of physician-assisted suicide.
Dr. Quinlan was a very nice man. He was soft-spoken, friendly, and intelligent. He had originally become involved in the subject of physician-assisted suicide by accident, while trying to help a patient near the end of her life who was suffering terribly.
That particular clinical case, which Dr. Quinlan wrote up and published in a major medical journal, launched a second career of sorts for him, as he became a leading figure in the physician-assisted suicide movement. In fact, he was lead plaintiff in a challenge of New York’s then-prohibition against physician-assisted suicide.
The case eventually went all the way to the US Supreme Court, which added to his fame. As it happened, SCOTUS ruled 9-0 against him, definitively establishing that there is no “right to die” enshrined in the Constitution, and affirming that the state has a compelling interest to protect the vulnerable.
SCOTUS’s unanimous decision against Dr. Quinlan meant that his side had somehow pulled off the impressive feat of uniting Antonin Scalia, Ruth Bader Ginsberg, and all points in between against their cause. (I never quite saw how that added to his luster, but such is the Academy.)
At any rate, I once had a conversation with Dr. Quinlan about physician-assisted suicide. I told him that I opposed it ever becoming legal. I recall he calmly, pleasantly asked me why I felt that way.
First, I acknowledged that his formative case must have been very tough, and allowed that maybe, just maybe, he had done right in that exceptionally difficult situation. But as the legal saying goes, hard cases make bad law.
Second, as a clinical physician, I felt strongly that no patient should ever see their doctor and have to wonder if he was coming to help keep them alive or to kill them.
Finally, perhaps most importantly, there’s this thing called the slippery slope.
As I recall, he replied that he couldn’t imagine the slippery slope becoming a problem in a matter so profound as causing a patient’s death.
Well, maybe not with you personally, Dr. Quinlan, I thought. I said no more.
But having done my residency at a major liver transplant center in Boston, I had had more than enough experience with the rather slapdash ethics of the organ transplantation world. The opaque shuffling of patients up and down the transplant list, the endless and rather macabre scrounging for donors, and the nebulous, vaguely sinister concept of brain death had all unsettled me.
Prior to residency, I had attended medical school in Canada. In those days, the McGill University Faculty of Medicine was still almost Victorian in its ways: an old-school, stiff-upper-lip, Workaholics-Anonymous-chapter-house sort of place. The ethic was hard work, personal accountability for mistakes, and above all primum non nocere – first, do no harm.
Fast forward to today’s soft-core totalitarian state of Canada, the land of debanking and convicting peaceful protesters, persecuting honest physicians for speaking obvious truth, fining people $25,000 for hiking on their own property, and spitefully seeking to slaughter harmless animals precisely because they may hold unique medical and scientific value.
To all those offenses against liberty, morality, and basic decency, we must add Canada’s aggressive policy of legalizing, and, in fact, encouraging industrial-scale physician-assisted suicide. Under Canada’s Medical Assistance In Dying (MAiD) program, which has been in place only since 2016, physician-assisted suicide now accounts for a terrifying 4.7 percent of all deaths in Canada.
MAiD will be permitted for patients suffering from mental illness in Canada in 2027, putting it on par with the Netherlands, Belgium, and Switzerland.
To its credit, and unlike the Netherlands and Belgium, Canada does not allow minors to access MAiD. Not yet.
However, patients scheduled to be terminated via MAiD in Canada are actively recruited to have their organs harvested. In fact, MAiD accounts for 6 percent of all deceased organ donors in Canada.
In summary, in Canada, in less than 10 years, physician-assisted suicide has gone from illegal to both an epidemic cause of death and a highly successful organ-harvesting source for the organ transplantation industry.
Physician-assisted suicide has not slid down the slippery slope in Canada. It has thrown itself off the face of El Capitan.
And now, at long last, physician-assisted suicide may be coming to New York. It has passed the House and Senate, and just awaits the Governor’s signature. It seems that the 9-0 Supreme Court shellacking back in the day was just a bump in the road. The long march through the institutions, indeed.
For a brief period in Western history, roughly from the introduction of antibiotics until Covid, hospitals ceased to be a place one entered fully expecting to die. It appears that era is coming to an end.
Covid demonstrated that Western allopathic medicine has a dark, sadistic, anti-human side – fueled by 20th-century scientism and 21st-century technocratic globalism – to which it is increasingly turning. Physician-assisted suicide is a growing part of this death cult transformation. It should be fought at every step.
I have not seen Dr. Quinlan in years. I do not know how he might feel about my slippery slope argument today.
I still believe I was correct.


Bank of Canada governor warns citizens to anticipate lower standard of living

Canada Seizes 4,300 Litres of Chinese Drug Precursors Amid Trump’s Tariff Pressure Over Fentanyl Flows
The era of Climate Change Alarmism is over

B.C. government laid groundwork for turning private property into Aboriginal land
-
Environment2 days ago
The era of Climate Change Alarmism is over
-
Aristotle Foundation1 day ago
B.C. government laid groundwork for turning private property into Aboriginal land
-
 Business2 days ago
Business2 days agoYou Won’t Believe What Canada’s Embassy in Brazil Has Been Up To
-
 Crime1 day ago
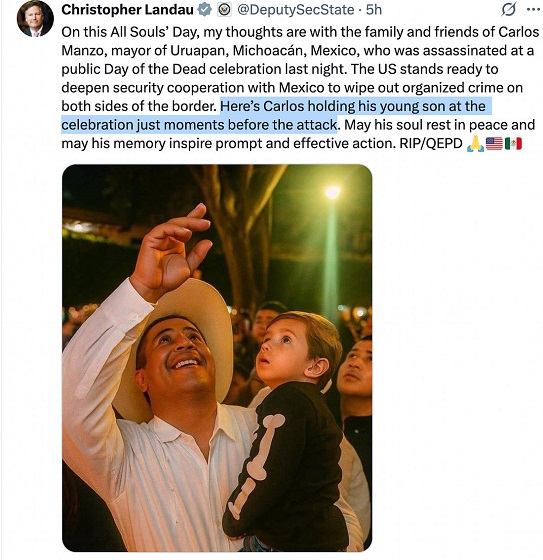
Crime1 day agoPublic Execution of Anti-Cartel Mayor in Michoacán Prompts U.S. Offer to Intervene Against Cartels
-
 Bruce Dowbiggin17 hours ago
Bruce Dowbiggin17 hours agoA Story So Good Not Even The Elbows Up Crew Could Ruin It
-
 Alberta17 hours ago
Alberta17 hours agoCanada’s heavy oil finds new fans as global demand rises
-
 Automotive2 days ago
Automotive2 days agoCarney’s Budget Risks Another Costly EV Bet
-
Addictions16 hours ago
The War on Commonsense Nicotine Regulation