Alberta
Big news for Alberta’s students in pandemic update from Minister LaGrange

Helping students catch up after pandemic disruption
As part of Alberta’s Recovery Plan, up to $45 million will support younger students who have fallen behind during the pandemic and more flexibility will be provided for students writing diploma exams.
Supporting reading, writing and numeracy skills for early learners
In May 2021, Alberta’s government announced $45 million would be available for school authorities to offer targeted programming to enhance literacy and numeracy skills.
School authorities have completed learning assessments to identify students who could benefit from targeted programming and now funds will be distributed at a per-student rate of $490.
School authorities have the flexibility to use this funding to design programming to best meet the needs of their students. Programming will be above and beyond classroom learning. The initial focus will be on students in grades 2 and 3, with targeted support for students in Grade 1 starting in February 2022.
“Many Alberta students had their education disrupted during the pandemic, which resulted in lost classroom and instruction time. We are committed to addressing this learning loss, and this funding will support students who need extra help to improve their reading, writing and numeracy skills. This grant gives school authorities the funds and flexibility they need to ensure each student is successful.”
“This $45 million for student learning is welcome news as school boards continue to face a variety of unique challenges due to the pandemic. This will help boards support recovery from long-term effects of learning loss, based on local needs.”
“AISCA is thankful that the Government of Alberta is recognizing and addressing learning disruptions caused by the COVID-19 pandemic. Our association appreciates that the government has taken a proactive approach to remediate and target learning challenges in the early years of a student’s development.”
Diploma exams
In response to feedback from students, parents and education partners about stress and anxiety around academic achievement exams, Alberta Education will temporarily change the weighting of diploma exams to 10 per cent from 30 per cent for the 2021-22 school year.
The ministers of Advanced Education and Education have sent an open letter to Alberta’s post-secondary institutions to advise them of this change and encourage them to further consider the impact the pandemic has had on students who are applying to their post-secondary institutions.
“Alberta’s students continue to face challenges due to the pandemic and I have heard concerns for our graduating class of 2022. I’ve heard feedback from students on my Minister’s Youth Council as well as from education partners that changing the weight of diploma exams will reduce the burden on students while still giving them valuable exam writing experience. We’re making this temporary change in recognition of these circumstances, which we hope will place less of a burden on these students.”
“The College of Alberta School Superintendents is pleased with the Alberta government’s commitment to provide additional funding to support school divisions with addressing Grade 1 to 3 student learning challenges stemming from the pandemic. We’re also grateful for the Minister’s decision to reduce the weighting of diploma exams as it will support Grade 12 students whose learning has also been adversely impacted.”
“As a member of the Minister’s Youth Council, it pleases me to see the Minister taking our feedback and concerns into consideration. As a Grade 12 student, the experience of writing diplomas is essential to prepare us for success as we consider post-secondary. Reducing the weighting of the exams will lessen the impact on mental health in youth while still ensuring that students are motivated to learn and understand the critical value of our education despite the effects of the pandemic.”
At-home rapid tests
Alberta’s government is continuing to use all available tools to stop the spread of COVID-19. Beginning Oct. 27, at-home rapid test kits will be provided to schools with kindergarten to Grade 6 students across the province that are on outbreak status. The program is optional, free, and starts immediately.
Schools will provide the students and staff who wish to participate with 10 tests to take home, and they will be required to test twice weekly for five weeks. Testing regularly ensures testing is most effective. A how-to video for parents and a fact sheet translated into multiple languages offer tips on how to use the kits.
Quick facts
Programming support:
- Of the up to $45 million in learning loss supports, approximately $30 million will be invested now to benefit students in grades 2 and 3. In response to feedback received from school authorities, up to $15 million will be allocated to students in Grade 1 in February 2022.
- With this funding, in grades 2 and 3, approximately 38,000 students will receiving literacy programing and approximately 25,000 will receive numeracy programming, recognizing that some students would qualify for both supports. The number of Grade 1 program opportunities will be available after assessments in the new year.
- Focused programming sessions are intended to be provided for up to 16 weeks. School authorities have the flexibility to design the length and frequency of the programming sessions.
- Funds will be distributed on a per-student basis with a minimum funding amount based on the number of eligible students per school.
At-home rapid tests:
- If a student or staff member has symptoms of COVID-19, they should not use a rapid test. They should stay home and book a test online with the Alberta Health Services (AHS) assessment tool or by calling 811.
- Schools on outbreak must submit a request to Alberta Health to receive tests for this program.
- If a student or staff member has a positive rapid test result, they must isolate for 10 days or until they have a negative test through AHS.
Agriculture
Lacombe meat processor scores $1.2 million dollar provincial tax credit to help expansion

Alberta’s government continues to attract investment and grow the provincial economy.
The province’s inviting and tax-friendly business environment, and abundant agricultural resources, make it one of North America’s best places to do business. In addition, the Agri-Processing Investment Tax Credit helps attract investment that will further diversify Alberta’s agriculture industry.
Beretta Farms is the most recent company to qualify for the tax credit by expanding its existing facility with the potential to significantly increase production capacity. It invested more than $10.9 million in the project that is expected to increase the plant’s processing capacity from 29,583 to 44,688 head of cattle per year. Eleven new employees were hired after the expansion and the company plans to hire ten more. Through the Agri-Processing Investment Tax Credit, Alberta’s government has issued Beretta Farms a tax credit of $1,228,735.
“The Agri-Processing Investment Tax Credit is building on Alberta’s existing competitive advantages for agri-food companies and the primary producers that supply them. This facility expansion will allow Beretta Farms to increase production capacity, which means more Alberta beef across the country, and around the world.”
“This expansion by Beretta Farms is great news for Lacombe and central Alberta. It not only supports local job creation and economic growth but also strengthens Alberta’s global reputation for producing high-quality meat products. I’m proud to see our government supporting agricultural innovation and investment right here in our community.”
The tax credit provides a 12 per cent non-refundable, non-transferable tax credit when businesses invest $10 million or more in a project to build or expand a value-added agri-processing facility in Alberta. The program is open to any food manufacturers and bio processors that add value to commodities like grains or meat or turn agricultural byproducts into new consumer or industrial goods.
Beretta Farms’ facility in Lacombe is a federally registered, European Union-approved harvesting and meat processing facility specializing in the slaughter, processing, packaging and distribution of Canadian and United States cattle and bison meat products to 87 countries worldwide.
“Our recent plant expansion project at our facility in Lacombe has allowed us to increase our processing capacities and add more job opportunities in the central Alberta area. With the support and recognition from the Government of Alberta’s tax credit program, we feel we are in a better position to continue our success and have the confidence to grow our meat brands into the future.”
Alberta’s agri-processing sector is the second-largest manufacturing industry in the province and meat processing plays an important role in the sector, generating millions in annual economic impact and creating thousands of jobs. Alberta continues to be an attractive place for agricultural investment due to its agricultural resources, one of the lowest tax rates in North America, a business-friendly environment and a robust transportation network to connect with international markets.
Quick facts
- Since 2023, there are 16 applicants to the Agri-Processing Investment Tax Credit for projects worth about $1.6 billion total in new investment in Alberta’s agri-processing sector.
- To date, 13 projects have received conditional approval under the program.
- Each applicant must submit progress reports, then apply for a tax credit certificate when the project is complete.
- Beretta Farms has expanded the Lacombe facility by 10,000 square feet to include new warehousing, cooler space and an office building.
- This project has the potential to increase production capacity by 50 per cent, thereby facilitating entry into more European markets.
Related information
From Premier Danielle Smith and Alberta.ca/Next
Let’s talk about an Alberta Pension Plan for a minute.
With our young Alberta workforce paying billions more into the CPP each year than our seniors get back in benefits, it’s time to ask whether we stay with the status quo or create our own Alberta Pension Plan that would guarantee as good or better benefits for seniors and lower premiums for workers.
I want to hear your perspective on this idea and please check out the video. Get the facts. Join the conversation.
Visit Alberta.ca/next

RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Blind to the Left: Canada’s Counter-Extremism Failure Leaves Neo-Marxist and Islamist Threats Unchecked

Why it’s time to repeal the oil tanker ban on B.C.’s north coast
Alberta Provincial Police – New chief of Independent Agency Police Service
-
 Energy1 day ago
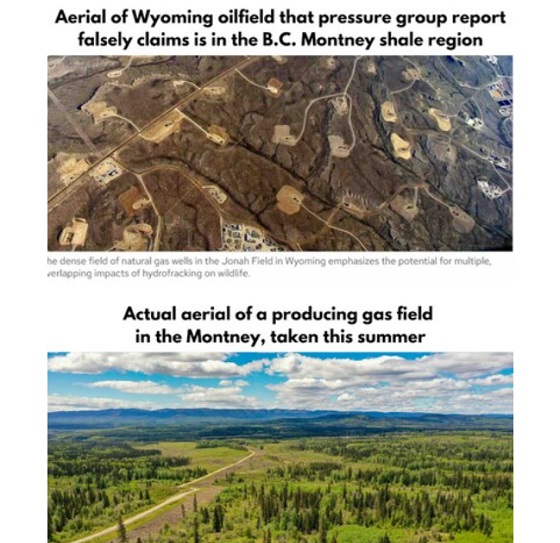
Energy1 day agoB.C. Residents File Competition Bureau Complaint Against David Suzuki Foundation for Use of False Imagery in Anti-Energy Campaigns
-
 Alberta2 days ago
Alberta2 days agoAlberta uncorks new rules for liquor and cannabis
-
 COVID-191 day ago
COVID-191 day agoCourt compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts
-
 Crime2 days ago
Crime2 days agoProject Sleeping Giant: Inside the Chinese Mercantile Machine Linking Beijing’s Underground Banks and the Sinaloa Cartel
-
 C2C Journal23 hours ago
C2C Journal23 hours agoCanada Desperately Needs a Baby Bump
-
 International1 day ago
International1 day agoTrump transportation secretary tells governors to remove ‘rainbow crosswalks’
-
Alberta1 day ago
Alberta Next: Alberta Pension Plan
-
Agriculture10 hours ago
Lacombe meat processor scores $1.2 million dollar provincial tax credit to help expansion