MacDonald Laurier Institute
Barriers to care persist but access to MAiD keeps expanding

From the Macdonald Laurier Institute
By Ramona Coelho
Our government has allowed the incredible power of certain lobby groups to control the public discourse and policies around MAiD and its expansion, prioritizing access to MAiD over the safety of Canadians.
My family medicine practice serves predominantly low-income and marginalized patients, including refugees, those who have been in our prison system or are facing charges, and many with disabilities and mental health issues. My patients experience high barriers to care and support and face social isolation and all kinds of discrimination. Observing the impacts of this has left me deeply concerned about our government’s priorities.
When the federal government introduced MAiD (a medical procedure that causes death) to those not at imminent risk of dying, I was appalled to learn that my patients, who are frequently blocked from care as a result of hurdles created by our government and systems, could potentially be offered an expedient death provided by the government.
In 2016, assisted suicide and euthanasia were first legalized in Canada and the term medical assistance in dying (MAiD) was created. Originally MAiD was presented as an exceptional lethal procedure for ending the lives of consenting adults who were experiencing intolerable suffering and were near death. The legislation required that patients meet certain criteria, including having a “grievous and irremediable” medical condition, such as organ failure or cancer, and a “reasonably foreseeable natural death.”
But the Canadian discourse around MAiD rapidly shifted to facilitating access and there has been a broadening of the number and criteria of those who qualify for MAiD. In 2021, Bill C-7 came into effect and removed some of the safeguards within the original pathway, now called Track 1, and created a new, second track, Track 2, for adults with physical disabilities[1] who are not dying. Furthermore, there is a planned expansion, though the timing is currently being debated in Parliament, for patients whose only medical condition is mental illness. Parliamentary recommendations in 2023 included future expansion to children and to incapable adults who signed advance directives for euthanasia.
Currently, those in Track 1 with a “reasonably foreseeable natural death” can potentially have their life ended the same day as the initial request if all the criteria are met and practitioners are available.
For those in Track 2, those not dying, death by lethal injection is set at a minimum of 90 days after the completion of the first MAiD assessment. To qualify for this track, a patient must also have a “grievous and irremediable” condition and experience intolerable psychological or physical suffering. Suffering is treated as purely subjective with no requirement for further validation. There is also no legal requirement for standard treatment options to be accessible or tried, only that a patient be informed that they exist. This means that a patient who says they are suffering intolerably could access MAiD having declined treatments that would remediate their condition. This could be because the treatment is inaccessible, or unaffordable, or if the patient declines therapy.
The Canadian Association of MAiD Assessors and Providers (CAMAP) has received 3.3 million dollars in funding from Health Canada to educate clinicians assessing and providing for those who have requested the service. So although the existing Track 1 and Track 2 pathways have different safeguards, in aiming to allow those near death to have access to MAiD quickly and with no barriers, CAMAP has created a guidance document that suggests clinicians can be flexible as to whether someone fits Track 1’s reasonably foreseeable natural death, since the law does not require that the person be terminally ill or likely to die within 6 or 12 months. It also states that a person may meet the reasonably foreseeable criterion if they’ve demonstrated a clear and serious intent to take steps to “make their natural death happen soon, or to cause their death to be predictable.” This could come about from a refusal to take antibiotics for an infection, stopping oxygen therapy, or refusing to eat and drink.
This means that people with disabilities can state their intention to or make themselves sick enough to qualify as having a reasonably foreseeable natural death, as is currently happening with adults who are not dying and yet are having their lives ended within days of their first MAiD assessment. In one case, a man had a mild stroke and received MAiD shortly after, even though he wasn’t terminally ill. The reason? He was approved for track 1 as he was temporarily eating less. This was due to following a cautious meal plan ordered by the treating team which was intended to prevent choking and aspiration risks.
Currently, some places in Canada have MAiD rates that are the highest in the world. By the end of 2022, there had been almost 45,000 MAiD deaths across Canada since legalization—more than 13,000 of which took place in 2022 with 463 of those individuals accessing MAiD through Track 2. Estimates based on provincial reporting approximate 16,000 deaths in 2023. Health Canada and MAiD expansionists have tried to reassure the public that the overwhelming number of MAiD deaths have been mostly Track 1 deaths (implying they were dying anyway) but we do not know how many of those persons were “fast-tracked” and may have had many decades of life left to live and the potential to recover with time and care.
The CAMAP guidance document that seems to circumvent Track 2 safeguards is just the beginning of many serious problems with MAiD legislation and practice in Canada.
Patient safeguards for MAiD are lacking
Other jurisdictions in the world where MAiD practices are legalized, such as New Zealand and Victoria, Australia, frown on or prohibit raising death as a treatment option. This is due to the power imbalance that exists between physician and patient, coupled with the patients’ assumption that the provider will only suggest the best options for their health. Raising MAiD unsolicited could cause undue pressure to choose death. Yet Health Canada’s 2023 Model Practice Standard for Medical Assistance in Dying recommends that MAiD should be raised to all who might qualify if the practitioner suspects it aligns with a patient’s values and preferences.
The model practice standard’s approach to “conscientious objection” is equally troubling. Health care providers who object to providing MAiD, even in specific cases, are considered conscientious objectors. A physician who is concerned that MAiD is not a patient’s best option is supposed to ignore their conscience or professional opinion and simply refer the patient on so they can seek access to a MAiD death.
This is further echoed in a CAMAP video training session where experts explain that patients might be driven to MAiD by unmet psycho-social needs. The expert leading the session responds to a trainee’s concerns: “If withdrawing is about protecting your conscience, you have [an] absolute right to do so.” But he adds: “You’ll then have to refer the person on to somebody else, who may hopefully fulfill the request in the end.” This demonstrates precisely how effective referrals can funnel patients toward death despite legitimate professional concerns and obligations that should have instead led to the process being stopped or paused.
In response to this legislation, many from the disability community have advocated for safe spaces where MAiD can’t pose a risk to their lives. The Disability Filibuster, a national grassroots disability community, stated in an open letter that its members have raised fears about seeking health care where death could be offered to them and if at their lowest, they might agree.
The disability community is not being alarmist in this concern. Health care providers often rate the quality of life of those with disabilities as poor despite those patients rating their own quality of life as the same as aged-matched healthy individuals. Put differently, many physicians might consider that patients with disabilities are better off dead, consciously or unconsciously, which might lead them to suggest MAiD.
Besides the problems of mandatory referral and raising MAiD unsolicited, there is another important factor to consider. Persons with physical disabilities systemically lack much of the essential care they need to live and consequently suffer higher rates of isolation, poverty, and marginalization, all of which can make death their most accessible option. The Canadian government commissioned a University of Guelph study, published in 2021, in which the researchers noted that some persons with disabilities were encouraged to explore the MAiD option—even though they had not been contemplating doing so—because of a lack of resources that would enable them to live. Those with disabilities can be approved for MAiD based on their disability, but it is their psycho-social suffering that can drive their requests.
The United Nations Special Rapporteur on the rights of persons with disabilities, the Independent Expert on the enjoyment of all human rights by older persons, and the Special Rapporteur on extreme poverty and human rights have all warned the Canadian government that the current MAiD framework could lead to human rights violations. Their concerns are validated by the numerous fact-checked stories about MAiD abuses that are emerging in Canada. These should give us pause. For example, Sathya Dhara Kovac, 44, ended her life through the MAiD program. She lived with a degenerative disease and her condition was worsening, but she wanted to live but lacked the home care resources to do so. “Ultimately it was not a genetic disease that took me out, it was a system,” Kovac wrote in an obituary to loved ones. All Canadians have a right to humane living conditions, to be treated with respect and dignity, and to receive appropriate timely medical care. Considering the living conditions and lack of care that as a society we allow persons with disabilities to have, choices to die might be understandable for those like Sathya. But we should ask ourselves if choices, made under inhumane conditions, are made freely if driven by structural coercion.
Disturbingly, there are MAiD assessors and providers who seem to be ok with proving MAiD under such inhumane conditions. One such provider testified at a parliamentary committee on MAiD that if someone had to wait a long time for a service that would remediate their suffering, she would still consider that waiting to be irremediable suffering and grant them MAiD in the interim. Therefore, it is not surprising that patients with unaddressed psycho-social suffering are being given MAiD by assessors like her.
When it was considering Bill C-7, the federal government asked the Parliamentary Budget Officer to estimate cost savings to our health care system of the legalization of MAiD. The office did this by looking at the comparative cost savings of MAiD versus palliative care at the end of life. Through this impoverished lens of valuation, it is clear that the cost savings will be even greater when, by many years, we prematurely end the lives of people who have higher care needs, especially when we factor in social services, disability benefits, equipment, and other costs on top of the direct savings to health care budgets. But this is not how we should create budgets or measure outcomes. Our socialized health care system is meant to serve those with disabilities, not consider them a cost to the system.
The Canadian government is currently deciding on the timing for its further roll-out of MAiD, this time for mental illness and with no legislative changes to the current safeguards. This expansion is alarming given what we know is happening already to disabled Canadians under the existing MAiD regime. The Canadian Association of Chairs of Psychiatry wrote a letter in 2022—and some testified more recently in Parliament—that we are not ready for this development. They have warned that there is no evidence to guide decisions about who with mental illness would not get better. The evidence suggests that for every 5 people whose lives would be ended based on the sole medical condition of mental illness, 2 or 3 would have recovered. We expect to have much higher numbers qualifying for MAiD on the grounds of mental illness in Canada than in other jurisdictions that allow assisted death for this reason, since barriers to care and unmitigated psycho-social suffering do not have to be rectified in this country (as they do elsewhere) before being granted MAiD.
Our government has allowed the incredible power and influence of certain lobby groups and their members to control the public discourse and policies around MAiD and its expansion, prioritizing access to MAiD over the safety of Canadians. Besides the current discussion about when to legalize MAiD for mental illness, the parliamentary committee has also recommended expansion to children and MAiD by advance directives. With eligibility for MAiD continuing to broaden, we are not giving priority to serving those most in need, but instead seem intent on rapidly expanding a path to end their lives.
[1] Disabilities is an umbrella term that includes impairment, chronic illness and/or other conditions.
Dr. Ramona Coelho is a family physician in London, Ontario. Her practice largely serves marginalized patients.

![]()
By Stephen Nagy for Inside Policy
Beijing understands what many Canadians still resist: that our greatest national virtues, including our desire to be an “honest broker” on the world stage, have become our most exploitable weaknesses.
On December 1, 2018, RCMP officers arrested Huawei CFO Meng Wanzhou at Vancouver International Airport. As Canadians know well, within days, China seized two Canadians, Michael Kovrig and Michael Spavor, on fabricated espionage charges. For 1,019 days, they endured arbitrary detention while Canada faced an impossible choice of abandoning the rule-of-law or watching its citizens suffer in Chinese prisons.
This was hostage diplomacy. But more insidiously, it was also the opening move in a broader campaign against Canada, guided by the ancient Chinese proverb “借刀杀人” (Jiè dāo shā rén), or “Kill with a borrowed knife.” Beijing’s strategy, like the proverb, exploits others to do its bidding while remaining at arm’s length. In this case, it seeks to exploit Canadian vulnerabilities such as our resource-dependent economy, our multicultural identity, our loosely governed Arctic territories, and our naïve belief that we can balance relationships with all major powers – even when those powers are in direct conflict with one another.
With its “borrowed knife” campaign, Beijing understands what many Canadians still resist: that our greatest national virtues, including our desire to be an “honest broker” on the world stage, have become our most exploitable weaknesses.
The Weaponization of Canadian Niceness
Canadian foreign policy rests on the Pearsonian tradition. It is the belief that our lack of imperial history and (now irrelevant) middle-power status uniquely positions us as neutral mediators. We pride ourselves on sending peacekeepers, not warfighters. We build bridges through dialogue and compromise.
Beijing exploited this subjective, imagined identity. When Canada arrested Meng pursuant to our extradition treaty with the United States, Chinese state media framed it as Canada “choosing sides” and betraying its honest broker role. This narrative trapped Canadian political culture. Our mythology says we transcend conflicts through enlightened multilateralism. But the modern world increasingly demands choosing sides.
When former Prime Minister Jean Chrétien and former Ambassador John McCallum advocated releasing Meng to free the “Two Michaels,” they weren’t acting as Chinese agents. They were expressing a genuinely Canadian impulse that conflict resolves through compromise. Yet this “Canadian solution” was precisely what Beijing sought, abandoning legal principles under pressure.
China’s economic coercion has followed a similar logic. When Beijing blocked Canadian canola, pork, and beef exports – targeting worth $2.7 billion worth of Prairie agricultural products – the timing was transparently political. However, China maintained the fiction of “quality concerns,” making it extremely difficult for Canada to challenge the restrictions via the World Trade Organization. At the same time, Prairie farmers pressured Ottawa to accommodate Beijing.
The borrowed knife was Canadian democratic debate itself, turned against Canadian interests. Beijing didn’t need to directly change policy, it mobilized Canadian farmers, business lobbies, and opposition politicians to do it instead.
The Arctic: Where Mythology Meets Reality
No dimension better illustrates China’s strategy than the Arctic. Canada claims sovereignty over vast northern territories while fielding six icebreakers to Russia’s forty. We conduct summer sovereignty operations that leave territories ungoverned for nine months annually. Chinese state-owned enterprises invest in Arctic mining, Chinese research vessels map Canadian waters, and Beijing now calls itself a “near-Arctic state,” a term appearing nowhere in international law.
This campaign weaponizes the gap between Canadian mythology and capacity. When China proposes infrastructure investment, our reflex is “economic opportunity.” When Chinese researchers request Arctic access, our instinct is accommodation because we’re co-operative multilateralists. Each accommodation establishes precedent, each precedent normalizes Chinese presence, and each normalized presence constrains future Canadian options.
Climate change accelerates these dynamics. As ice melts, the Northwest Passage becomes navigable. Canada insists these are internal waters. China maintains they’re international straits allowing passage. The scenario exposes Canada’s dilemma perfectly. Does Ottawa escalate against our second-largest trading partner over waters we cannot patrol, or accept Chinese transits as fait accompli? Either choice represents failure.
The Diaspora Dilemma
Canada’s multiculturalism represents perhaps our deepest national pride. The Chinese Communist Party has systematically weaponized this openness through United Front Work Department operations, an ostensibly independent community organization that provides genuine services while advancing Beijing’s agenda including: monitoring dissidents, mobilizing Chinese-Canadians for CCP-approved candidates, organizing counter-protests against Tibetan and Uyghur activists, and creating environments where criticism of Beijing risks community ostracism and threats to relatives in China.
The establishment of illegal Chinese police stations in Toronto and Vancouver represents this operation’s logical endpoint. These “overseas service centres” conducted intimidation operations, pressured targets to return to China, and maintained surveillance on diaspora communities.
Canada’s response illuminates our vulnerability. When investigations exposed how Chinese organized crime groups, operating with apparent CCP protection, laundered billions through Vancouver real estate while financing fentanyl trafficking, initial reactions accused investigators of anti-Chinese bias. When CSIS warned that MPs might be compromised, debate focused on whether the warning represented racial profiling rather than whether compromise occurred.
Beijing engineered this trap brilliantly. Legitimate criticism of CCP operations becomes conflated with anti-Chinese racism. Our commitment to multiculturalism gets inverted into paralysis when a foreign government exploits ethnic networks for political warfare. The borrowed knife is Canadian anti-racism, wielded against Canadian sovereignty and this leaves nearly two million Chinese-Canadians under a cloud of suspicion while actual operations continue with limited interference.

What Resistance Requires
Resisting comprehensive pressure demands abandoning comfortable myths and making hard choices.
First, recognize that 21st-century middle-power independence is increasingly fictional. The global order is re-polarizing. Canada cannot maintain equidistant relationships with Washington and Beijing during strategic competition. We can trade with China, but not pretend shared rhetoric outweighs fundamental disagreements about sovereignty and human rights. The Pearsonian honest-broker role is obsolete when major powers want you to choose sides.
Second, invest in sovereignty capacity, not just claims. Sovereignty is exercised or forfeited. This requires sustained investment in military forces, intelligence services, law enforcement, and Arctic infrastructure. It means higher defence spending, more robust counterintelligence, and stricter foreign investment screening, traditionally un-Canadian approaches, which is precisely why we need them.
Third, build coalitions with countries facing similar pressures. Australia, Japan, South Korea, Lithuania, and others have faced comparable campaigns. When China simultaneously blocks Canadian canola, Australian wine, and Lithuanian dairy, that’s not separate trade disputes but a pattern requiring coordinated democratic response. The borrowed knife only works when we’re isolated.
Fourth, Ottawa must do much more to protect diaspora communities while confronting foreign operations. Effective policy must shut down United Front operations and illegal police stations while ensuring actions don’t stigmatize communities. Success requires clear communication that we’re targeting a foreign government’s operations, not an ethnic community.
Finally, we must accept the necessity of selective economic diversification. Critical infrastructure, sensitive technologies, and strategic resources cannot be integrated with an authoritarian state weaponizing interdependence. This means higher costs and reduced export opportunities – but maximum efficiency sometimes conflicts with strategic resilience. Canada can achieve this objective with a synergistic relationship with the US and other allies and partners that understand the tangential link between economic security and national security.
Conclusion
Canada’s myths, that we transcend conflicts, that multiculturalism creates only strength, that resource wealth brings pure prosperity and positivity, coupled with our deep vein of light-but-arrogant anti-Americanism, have become exploitable weaknesses. Beijing systematically tested each myth and used the gap between self-conception and reality as leverage.
The borrowed knife strategy works because we keep handing over the knife. Our openness becomes the vector for interference. Our trade dependence becomes the lever for coercion. Our niceness prevents us from recognizing we’re under attack.
Resistance doesn’t require abandoning Canadian values. It requires understanding that defending them demands costs we’ve historically refused to pay. The Chinese “Middle Kingdom” that tells the world it has had 5,000 years of peaceful history has entered a world that doesn’t reward peaceability, it exploits it. The question is whether we’ll recognize the borrowed knife for what it is and put it down before we bleed out from self-inflicted wounds.
Stephen R. Nagy is a professor of politics and international studies at the International Christian University in Tokyo and a senior fellow and China Project lead at the Macdonald-Laurier Institute (MLI). The title for his forthcoming monograph is “Japan as a Middle Power State: Navigating Ideological and Systemic Divides.”

![]()
By Stephen Nagy for Inside Policy
For several decades, China has pursued a sophisticated campaign to fracture the world’s most integrated defense partnership—that between Canada and the United States.
Beijing’s strategy goes beyond typical diplomatic pressure: it systematically exploits every Canada-US disagreement, transforming routine alliance friction into seemingly irreconcilable divisions. This has become a degree of magnitude easier under US President Donald Trump, with his mercurial policy shifts towards Ottawa. The revelations about Chinese interference in Canadian elections from the Security and Intelligence Threats to Elections (SITE) Task Force – a body comprised of Canadian government and security officials which monitors elections threats – illuminate only one dimension of this comprehensive assault on North American solidarity.
Beijing’s strategic logic is to divide and conquer. By portraying Canada as sacrificing sovereignty for American interests while simultaneously painting legitimate Canadian security concerns as US-driven paranoia, Beijing paralyzes Ottawa’s decision-making and undermines continental defense cooperation.
The 2018 arrest of Huawei CFO Meng Wanzhou crystallized China’s approach. When Canada honored its extradition treaty with the US by detaining Meng at the Vancouver airport, Beijing immediately framed this routine legal cooperation as evidence of Canadian subservience. Chinese state media didn’t simply criticize the arrest, they specifically portrayed Canada as “a pathetic clown” and “running dog of the US.”
Within nine days, China retaliated by detaining Michael Kovrig and Michael Spavor, holding them for 1,019 days. But Beijing’s messaging revealed its true objective. Chinese diplomats repeatedly demanded Canada “correct its mistake” by defying the U.S. extradition request. Ambassador Lu Shaye explicitly stated Canada could resolve the crisis by demonstrating “independence” from Washington.
The economic pressure followed the same pattern. China banned canola imports from two major Canadian companies in March 2019, citing “pests” but Chinese officials privately linked the ban to the Meng case. When targeting Canadian meat exports, Beijing’s timing again coincided with moments of US-Canada cooperation on Huawei restrictions.
China’s wedge strategy extends beyond retaliation to proactive exploitation of bilateral tensions. During the Keystone XL pipeline disputes, Chinese state media amplified Canadian grievances while offering Beijing as an “alternative partner” for energy exports. When the Biden administration cancelled the pipeline in 2021, Chinese diplomats and media immediately highlighted American “betrayal” of Canadian interests.
Similarly, during US-Canada disputes over softwood lumber tariffs and Buy American provisions, Chinese officials consistently present themselves as more reliable economic partners. The message is always the same: American protectionism harms Canadian workers, while China offers stable market access conveniently omitting Beijing’s own coercive trade practices.
On defense, China exploits Canadian concerns about Arctic sovereignty vis-à-vis the United States. When Washington challenges Canada’s claims over the Northwest Passage, Chinese media amplify these disagreements while positioning Beijing as respecting Canadian Arctic sovereignty – even as China declares itself a “near-Arctic state” and seeks military access to the region.
Recent intelligence revelations confirm China’s systematic attempts to influence Canadian politics specifically to create US-Canada friction. According to CSIS documents, Chinese intelligence assessed that a Liberal minority government would be less likely to follow Washington’s harder line on China. Beijing’s interference operations during the 2019 and 2021 elections specifically targeted Conservative candidates perceived as pro-American on China policy.
The Chinese United Front Work Department cultivates Canadian political and business figures through seemingly innocent organizations. A 2020 National Security and Intelligence Committee report found these groups specifically encouraged narratives about American “bullying” of Canada and promoted “made-in-Canada” foreign policies that coincidentally aligned with Chinese interests.
Chinese diplomats regularly exploit Canadian media to amplify anti-American sentiments. During USMCA negotiations, Chinese officials gave exclusive interviews to Canadian outlets sympathizing with “American strong-arm tactics.” When Canada considered banning Huawei from 5G networks, Chinese embassy officials published op-eds in Canadian newspapers warning against following “US tech hegemony.”
China’s wedge strategy carries profound implications for NORAD and continental defense. By creating friction between Ottawa and Washington, Beijing undermines the trust essential for integrated aerospace warning and maritime domain awareness. Chinese military academics have explicitly written about exploiting contradictions in US-Canada defense relations to complicate American force projection.
The stakes are rising as Arctic ice melts. China’s 2018 Arctic strategy specifically mentions differences between Arctic states as creating opportunities for Chinese involvement. Every US-Canada disagreement over Arctic waters provides Beijing openings to position itself as a stakeholder in North American approaches.
Canada and the United States must recognize that their occasional disagreements, normal in any alliance, are systematically weaponized by Beijing. In light of this, at least four responses are essential.
First, Canada and the United States should establish a joint commission on foreign interference that specifically monitors and publicly exposes attempts to exploit bilateral tensions. When China amplifies US-Canada disagreements, coordinated responses can demonstrate alliance resilience rather than division.
Second, create alliance resilience mechanisms that automatically trigger consultations when third parties attempt to exploit bilateral disputes. The Two Michaels crisis revealed how Beijing uses hostage-taking to pressure alliance relationships. A joint response protocol could reduce such leverage.
Third, strengthen Track II dialogues between Canadian and American civil society, business, and academic communities. These networks can maintain relationship continuity even during governmental tensions, reducing Beijing’s ability to exploit temporary political friction.
Fourth, develop coordinated strategic communications that acknowledge legitimate bilateral differences while emphasizing shared values and interests. Honest discussion of disagreements, paired with clear statements about alliance solidarity, can inoculate against external manipulation.
Canada faces the delicate balance of maintaining sovereign decision-making while recognizing that Beijing systematically exploits any daylight between Ottawa and Washington. This isn’t about choosing between independence and alliance. It’s about understanding how Canada’s adversaries weaponize that false choice.
The empirical evidence is clear. From the Meng affair to election interference, from trade coercion to Arctic maneuvering, China consistently pursues the same objective: transforming America from Canada’s closest ally into a source of resentment and suspicion. Every success in this strategy weakens not just bilateral ties but the entire democratic alliance system.
As the Chinese saying goes, 笑里藏刀—a dagger hidden behind a smile. While professing respect for Canadian sovereignty and offering economic partnerships, Beijing wages sophisticated political warfare designed to isolate democratic allies from each other. Recognizing this strategy is the first step toward defeating it. The strength of North American democracy lies not in the absence of disagreements but in the ability to resolve them without external exploitation. In an era of systemic rivalry, the US-Canada partnership must evolve from unconscious integration to conscious solidarity – as different nations with sovereign interests, but united in defending democratic values against authoritarian manipulation.
Stephen Nagy is a professor of politics and international studies at the International Christian University in Tokyo, and a senior fellow at the Macdonald Laurier Institute. The tentative title for his forthcoming monograph is “Navigating U.S. China Strategic Competition: Japan as an International Adapter Middle Power.”


Wisdom of Our Elders: The Contempt for Memory in Canadian Indigenous Policy

Liberal bill “targets Christians” by removing religious exemption in hate-speech law

Egypt, Iran ‘completely reject’ World Cup ‘Pride Match’ plan

Canada’s free speech record is cracking under pressure
-
National2 days ago
Canada’s free speech record is cracking under pressure
-
 Energy1 day ago
Energy1 day agoTanker ban politics leading to a reckoning for B.C.
-
 Energy1 day ago
Energy1 day agoMeet REEF — the massive new export engine Canadians have never heard of
-
 Business2 days ago
Business2 days agoTaxpayers Federation calls on politicians to reject funding for new Ottawa Senators arena
-
 Fraser Institute1 day ago
Fraser Institute1 day agoClaims about ‘unmarked graves’ don’t withstand scrutiny
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoOttawa’s New Hate Law Goes Too Far
-
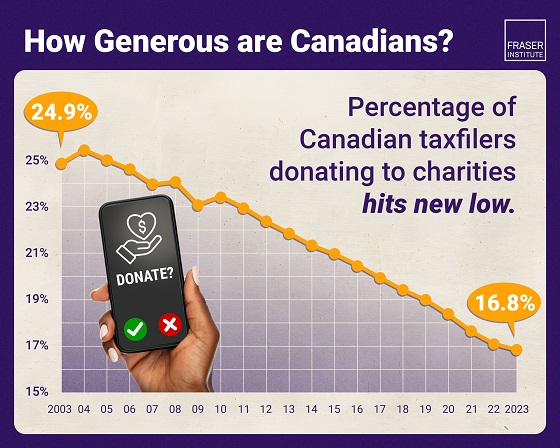 Business2 days ago
Business2 days agoAlbertans give most on average but Canadian generosity hits lowest point in 20 years
-
Business1 day ago
Too nice to fight, Canada’s vulnerability in the age of authoritarian coercion