Addictions
Alberta and opioids II: Marshall Smith’s ambitious campaign

Marshall Smith. Photo: PW

Click here to subscribe to The Paul Wells Newsletter.
Alberta’s system builder
The Alberta model, made in BC
“I, as you know, have been everywhere in this field, from eating out of garbage cans to this office,” Marshall Smith said. “So I have a deep respect for everybody who works along that continuum.”
We were sitting in the office at the Alberta Legislature reserved for chiefs of staff to Alberta premiers. That’s Smith’s current job. Premier Danielle Smith was probably nearby, though I didn’t see her on this trip. On a shelf behind Marshall Smith were two coffee mugs of different design, each bearing the inscription WAKE UP. SAVE LIVES. REPEAT.
Thank you for reading Paul Wells. This post is public so feel free to share it.
Anyway, Marshall Smith (all future uses of “Smith” in this post will refer to him, unless I specify the premier) was talking about the continuum from dumpsters to the centre of power. “Where you work on that continuum obviously colours the way that you enter this conversation,” he said. “When you are standing on a sidewalk with a person in front of you, the solutions to that person’s problem look very different than what you might do to plan a broader system of care, for a large population of people.”
This was his way of anticipating criticisms he faces as a leading strategist behind Alberta’s emerging strategy for handling a deadly progression in opioid doses. Since he entered Alberta’s government as a more junior staffer in the government of former premier Jason Kenney in 2019, Smith has been working to put a much greater emphasis on recovery from addiction than on “harm reduction,” whose valuable goal is to keep drug users alive whether they recover or not. This makes him a bête noire among harm-reduction advocates. (You can read a mild critique of his efforts here; or a real scorcher here).
What Smith was saying was, in effect, If you work on the street, you’re going to be all about harm reduction, and I respect that. But he is working on drug policy for a whole province, and perhaps beyond, so he needs a broader perspective. “I’m a system builder. So I don’t have the luxury of just focusing on one particular substance. I have to worry about the whole population. I have to worry about the disease burden of addiction and drug use more broadly.”
He sees much to worry about. “Over the last 30 years in Canada, successive governments have failed miserably to anticipate and adequately address the type of services — both from a capital investment and an operating investment — to help people do this.” By “this,” he means escaping addiction. “We have not cared about people with mental health and addiction issues. And we had the ability to not care because up until the last six or seven years, the evidence of them was hidden away.”
Smith first started thinking about this when he was in British Columbia, where he began his recovery from a history of drug use. In 2018, at the BC Centre for Substance Use, Smith co-wrote a report with Dr. Evan Wood that called for a large new investment in facilities and programs to help people recover from addiction. The report is no longer on the BCCSU website, but you can download a copy here.
“It was a 39-point strategy to transform the system in British Columbia,” Smith recalled. “The government of British Columbia wasn’t interested in that strategy. They wanted to go a particular direction.
“So that report is now known as the Alberta model.”
I’m leaving the paywall off these stories because I want them to be widely shared and discussed. But the reason I’m able to report and present big stories like this, with the travel and expenses that involves, is because many of my readers choose to become paying subscribers. If you want to support my work and get full access to everything I write, here’s the button.

Marshall Smith in the dining hall of the Lakeview Recovery Community, opening in July. Photo: PW
In its first page, the Wood/Smith report said “British Columbia has long suffered because of the lack of an effective system to support individuals in and pursuing recovery from substance use disorders.” The system’s “overwhelming focus” was on keeping people alive rather than helping them get better. Wood and Smith wanted that to change.
The need for major new investments in addiction recovery was essentially uncontroversial in B.C. Indeed governments there still periodically announce they are making such investments. But Smith was perpetually unsatisfied with the scale of that commitment.
A year after BC’s new NDP government could-shouldered his report, Smith began working in the UCP government of Alberta’s then-new premier, Jason Kenney.
“Obviously we started off very modestly,” Smith said. “I worked in an office down in the basement. Mental health and addiction wasn’t a big deal. It really was very much a group of cubicles.”
Today, Alberta’s department of mental health and addiction is the seventh-largest ministry in the provincial government.
“The ROSC transformation that is going on in Alberta is massive. It is one of the most massive whole-of-government system transformations that I’ve seen,” Smith said. The premier chairs a ROSC committee of cabinet with seven ministers.
I guess I’d better unpack that acronym. ROSC stands for “recovery-oriented system of care,” a term that appeared in the 2018 report Smith co-wrote.
So you get the premier and her ministers of mental health and addiction, Indigenous relations, advanced education, health, community and social services, public safety and the attorney general meeting regularly to coordinate recovery policy. The premier’s chief of staff is on the file constantly. As I mentioned on Monday, he devoted a full day to explaining this broad effort to me.
“We spend enormous amounts of time and energy,” Smith said. “All of us live and breathe this. Anybody out there that thinks that we’re just, from a conservative perspective, just cavalierly doing this, that just couldn’t be more untrue. We we are in this completely and totally. We monitor almost everything that goes on in the system.”
What are they working on? Smith said the “recovery” part of that “recovery-oriented system of care” jargon-ball gets most of the attention, because it draws attention to the contrast between harm-reduction and abstinence-based recovery models. But Smith is a wonk, and if anything he is more interested in the “system of care” part. His goal is to ensure that every interaction an opioid user has with the modern government apparatus is designed to encourage recovery from dependency. Since people who use drugs tend to bump up against the state a lot, Alberta’s emerging system has a lot of moving parts. The goal is to hook the parts up more effectively.
One of the other men in Smith’s office, Dr. Nathaniel Day, chimed in. He’s been the lead strategist on substance use at Alberta Health Services. He’s an important Smith collaborator.
“Across Canada,” he said, “the system of care for people with addiction has been fragmented, poorly thought out — convenient.” He meant services had generally only been provided when, and where, it was easy for government to provide them. “If you look at opioid dependency treatment, if you lived in a suburban or rural community, it didn’t matter that you had an opioid use disorder. Tough. We had no services for you.”
Day designed the Virtual Opioid Dependency Program, which provides online consultations to patients anywhere in Alberta, and if needed, prescriptions to medications that can be filled at local pharmacies. For patients without coverage, the medication is free and if their local pharmacist has it in stock, available on the day of the call.
“We went in and said, enough is enough,” Day said. “What would be good enough for you and your family? And how do we take that to everybody?”
Which medication? “In this province, we’re huge fans of gold-standard opioid-replacement medications, and we use it a lot,” Smith said. “We have Sublocade, which is something that other provinces don’t have because it’s very expensive. It’s the injectable version of Suboxone. It’s a subcutaneous injection, it goes under the skin, it lasts for 30 days, where the oral is 24-hour. So that’s a thousand bucks a shot, and we pay for that.”
An obvious point about this is that these so-called opioid agonist treatments, or OATs, are big-time harm reduction. They greatly reduce both withdrawal symptoms and highs. One question that I still have, after watching everything Smith and the Alberta government are doing on drug recovery, is whether other provinces could afford to match it.
Running into those institutions
VODP is useful for people who are able to reach out for help from home. But other potential beneficiaries are distracted, or in distress. Very often they run into the police.
“So we took that technology” — the virtual access to physicians and treatment — “and we gave it to the 34 police agencies that we have in the province,” Smith said.
“We said to the officers, ‘If you encounter somebody who has an opioid-use disorder, you can get them started on opioid-use medication. You can, officer. Here’s the phone number to call. Put them on. We make the arrangements. They go to the pharmacy, right then and there. If they’re on the street, that can be done right in the back of a police car.
“If they are in custody at the cell block and they go into the cell block, we have put paramedics in every cell block in Alberta. So the first thing that happens to somebody when they’re arrested and they go into into municipal cells, they’re met by a paramedic that says, ‘Let’s talk about your substance use. Are you an opioid user? We can offer you immediate treatment right now. Right here. Would you like to do that?’ Through our police programs, we’re probably up to like 4,000 people who have taken us up on that.”
That’s what you can get done in a police cruiser or a holding pen. Lots of people go much further into the correctional system than that. So does Smith’s system of care.
“[Alberta’s] focus on corrections and police right now, admittedly, is the opposite of what some other jurisdictions are focusing on,” Smith said. If anything this was an understatement. A major argument for decriminalization and safe supply is that the last thing a drug user needs is the stigma of a criminal record. Other jurisdictions, Smith said, “are running away from those institutions when they should be running into those institutions.
“I’ll give you a very direct example why.
“We know, from the 2017 coroner’s report in Alberta that 40 percent of the people who died [of opioid-related causes] were in custody in the year prior to their death. That’s a really important piece of information, because it tells me I have a big chunk of population there that — if I can get at them, and if we can change the way that they experience this process — we can make a big dent in these numbers.”
A lot of people in the correctional system have substance-use disorder, even if that’s not what they’re in for. “We said, ‘Let’s really do a different way of thinking on this,’” Smith said. “Even though Corrections is a public-safety agency, we want the Ministry of Mental Health and Addiction to take over all Corrections health care.”
Perhaps four in five detainees, he said, “have alcoholism, addiction and mental-health issues. They’re all pooled up in one place and they’re not doing anything. They’ve got nothing but time on their hands. And I don’t have to build a new building? You’re kidding me! This is fantastic! Why wouldn’t I just put therapists in? So we now have treatment programs inside correctional centers.”
Of course a lot of places do programs for inmates. “But what they’re going to show you when you unpack that is, ‘Well, we give them this workbook,’” Smith said. “What they’re not doing is the deep transformative, therapy work that is necessary. And honestly, Paul, our Therapeutic Living Units are probably the best treatment programs we have in Alberta.”
With that, we piled into Smith’s SUV — Smith, Day and the third member of Smith’s team that day, a physician and consultant named Dr. Paul Sobey. A half-hour later we arrived at the Fort Saskatchewan Correctional Centre, northeast of Edmonton.
Here we visited the Therapeutic Living Unit, a full-time addiction-recovery program for 21 women who are housed separately from the general inmate population. That’s about 10% of the total population of women at Fort Saskatchewan. The program opened in February. Participants, who must apply, run through a 12-hour daily program of activity: morning check-in meetings, physical exercise, twice-daily smudge ceremonies reflecting the large Indigenous population in the correctional system, frequent meetings of Alcoholics Anonymous and Narcotics Anonymous as well as the more recently developed SMART Recovery system. Participants are rarely alone during daylight hours. The program is designed to last for months, which struck me as an unusually long time for a recovery program.
Four of the program’s participants sat on a sofa and talked about their experience in the program. “I’ve been wondering and wondering if a program like this was going to happen,” one said.
“It’s like an answered prayer, honestly,” said another. “So I would just encourage you to keep opening places like this.”
That’s the plan. “We’ve got 12 correctional centers in Alberta,” Smith told me before our road trip. “Our goal is to have Therapeutic Living Units [in all of them]. There will come a time where we have whole correctional centers that are working on this model, right? This requires massive intervention, not tinkering around the edges. This is generational change in the way that we do corrections in Alberta.”
Connections
All of the four young women we heard from said they’re nervous about what happens when they get out of detention. Old acquaintances can encourage a return to old habits. Which is part of the reason why Alberta is also building a network of live-in Recovery Communities, long-term residential rehab programs to reinforce the lessons learned in the TLUs — or to help other people begin recovery if they didn’t arrive via the correctional system.
Once the system is fully built in 2027, “every correctional centre will have a sister Recovery Community,” Smith said. “That’s why we’re building 11 of them around the province. Five of them are on First Nations, in partnership with the First Nations.”
Here’s where the system starts to look like a system. After all, in the broadest outlines nothing’s new here. People in prisons have long received addiction counselling, and the Alberta government and various private groups have long run rehabs. But for the longest time, these assorted parts of the system could barely talk to one another. So the chances of a seamless transition from the correctional system to recovery care were lousy. They’re still not great, because the system is still being built, but the goal is a seamless network of care.
“Services in 2018, 2019 were very disconnected,” Warren Driechel, the Edmonton Police Service deputy chief we met the other day, told me. The bureaucratic runaround that we all have to face can be brutal on people with high needs and impaired function. Say you want to get on AISH, an income-support program for people with a medical condition. To do that, you need a doctor’s appointment. To get one, you need identification. To get ID, you need an address.
Public officials are working to provide services that match that complexity.
In January 2021, the EPS launched a “HELP Unit” to refer people to social services instead of just arresting them.
In September 2023, the police replaced the old holding cells where intoxicated people could dry out and then get dumped back on the street with an Integrated Care Centre where they could connect with social services that operate right in the centre.
And in January 2024, after many of the tent encampments were dismantled, a new Navigation and Support Centre became the city’s hub for providing medical, legal and bureaucratic help for people who have often been bereft.
The Nav Centre has nine shelter beds in the back where people can rest, if needed, while on-site staff and volunteers process their files. (Pets are welcome, unlike in some of the city’s shelters.) The centre has the province’s only on-site Service Alberta photo-ID station. On the day I visited, the Nav Centre assisted 50 people, with 24 visiting the desk run by the Hope Mission, 10 being helped by staff from Radius Health, 12 by the provincial department of mental health and addiction.
 |
Everything old is new
Our final stop was the Lakeview Recovery Community outside Gunn, northwest of Edmonton. When it opens in July, it’ll be the third or fourth in a network of such long-term residential programs. Lethbridge and Red Deer have been open for a while. The goal is to have 11 centres up and running across the province by 2027. Smith hopes that once the full network of centres is open, long wait times in Red Deer and Lethbridge will shrink, perhaps to the point where some beds will be available on-demand.
Each recovery community has its quirks. Lakeview will be for men only. Five of the centres will be on Indigenous land. The minimum stay will be four months, with some residents staying for up to a year. That’s a long stint for a rehab; in some private rehabs, it’s unusual to stay for even a month. In theory every day you spend with a combination of counselling, group therapy, twelve-step programs and medical care will increase your chances of success. No resident will pay for their stay at any recovery community. It’s covered by the government.
Work crews have been renovating the Lakeview site since 2022. It’s an impressive place, roomy and bright, with rooms where residents can meet visiting family, a huge kitchen where residents will learn cooking skills, and a dispensary for opioid agonist treatment. Residents will share bungalows while they’re in the program, five or six to a house.
 |
But it didn’t just come into existence. What’s now Lakeview began its existence as the McCullough Centre for homeless World War II veterans. It had been operating for years as an addiction rehab centre when Jason Kenney’s government closed it in 2021. When the government announced the site’s eventual reopening barely a year later, observers were baffled. Closing the centre fit a narrative about a government that put the bottom line over Albertans’ wellbeing. Refurbishing and reopening it was.. harder to explain. Fitting it into a network of nearly a dozen such centres that will, themselves, be better connected to street-level services and to the corrections system… well, we’ll see, won’t we?
I’m conscious of ending this installment in my series on opioids in Alberta on an ambivalent note. I simply don’t know how this will turn out. My first article, earlier this week, was about the scale of the challenge. This one is about the scale of the response. It’s impressive. It’s getting attention across the country. Sobey, the physician who was the third member of our little party as we toured the region’s facilities, has a consulting firm whose aim is to design recovery-oriented systems of care to any government that wants to start the conversation. His phone pinged with an inquiry from another provincial government while we were visiting the Fort Saskatchewan prison. These ideas may come soon to a province near you.
What we don’t know yet is whether they’ll work, or how well. In the third and final installment in this series, I’ll discuss a few reasons to reserve judgment.
But what Alberta is trying is, in many ways, not heretical. Nobody thinks it’s great design to leave desperate people to wander helplessly thorugh a piecemeal hodge-podge of social services and treatment options, with police and corrections hovering over it all as an aloof menace. Smith, his boss the premier, and several government departments are trying to build a better system.
There is room for many devils in the details. But if federalism is supposed to be a laboratory for testing different approaches to thorny problems, Alberta is testing this approach ambitiously. Watching Marshall Smith, I found myself wondering what other intractable governance problems could benefit from the sustained attention of an empowered senior staffer, a supportive head of government, and ministers and public servants working in close coordination.
For the full Paul Wells experience, upgrade your subscription.


First responders say it is not overdoses that leave them feeling burned out—it is the endless cycle of calls they cannot meaningfully resolve
The soap bottle just missed his head.
Standing in the doorway of a cluttered Halifax apartment, Derek, a primary care paramedic, watched it smash against the wall.
Derek was there because the woman who threw it had called 911 again — she did so nearly every day. She said she had chest pain. But when she saw the green patch on his uniform, she erupted. Green meant he could not give her what she wanted: fentanyl.
She screamed at him to call “the red tags” — advanced care paramedics authorized to administer opioids. With none available, Derek declared the scene unsafe and left. Later that night, she called again. This time, a red-patched unit was available. She got her dose.
Derek says he was not angry at the woman, but at the system that left her trapped in addiction — and him powerless to help.
First responders across Canada say it is not overdoses that leave them feeling burned out — it is the endless cycle of calls they cannot meaningfully resolve. Understaffed, overburdened and dispatched into crises they are not equipped to fix, many feel morally and emotionally drained.
“We’re sending our first responders to try and manage what should otherwise be dealt with at structural and systemic levels,” said Nicholas Carleton, a University of Regina researcher who studies the mental health of public safety personnel.
Canadian Affairs agreed to use pseudonyms for the two frontline workers referenced in this story. Canadian Affairs also spoke with nine other first responders who agreed to speak only on background. All of these sources cited concerns about workplace retaliation for speaking out.
Moral injury
Canada’s opioid crisis is pushing frontline workers such as paramedics to the brink.
A 2024 study of 350 Quebec paramedics shows one in three have seriously considered suicide. Globally, ambulance workers have among the highest suicide rates of public service personnel.
Between 2017 and 2024, Canadian paramedics responded to nearly 240,000 suspected opioid overdoses. More than 50,000 of those were fatal.
Yet many paramedics say overdose calls are not the hardest part of the job.
“When they do come up, they’re pretty easy calls,” said Derek. Naloxone, a drug that reverses overdoses, is readily available. “I can actually fix the problem,” he said. “[It’s a] bit of instant gratification, honestly.”
What drains him are the calls they cannot fix: mental health crises, child neglect and abuse, homelessness.
“The ER has a [cardiac catheterization] lab that can do surgery in minutes to fix a heart attack. But there’s nowhere I can bring the mental health patients.
“So they call. And they call. And they call.”
Thomas, a primary care paramedic in Eastern Ontario, echoes that frustration.
“The ER isn’t a good place to treat addiction,” he said. “They need intensive, long-term psychological inpatient treatment and a healthy environment and support system — first responders cannot offer that.”
That powerlessness erodes trust. Paramedics say patients with addictions often become aggressive, or stop seeking help altogether.
“We have a terrible relationship with the people in our community struggling with addiction,” Thomas said. “They know they will sit in an ER bed for a few hours while being in withdrawals and then be discharged with a waitlist or no follow-up.”
Carleton, of the University of Regina, says that reviving people repeatedly without improvement decreases morale.
“You’re resuscitating someone time and time again,” said Carleton, who is also director of the Psychological Trauma and Stress Systems Lab, a federal unit dedicated to mental health research for public safety personnel. “That can lead to compassion fatigue … and moral injury.”
Katy Kamkar, a clinical psychologist focused on first responder mental health, says moral injury arises when workers are trapped in ethically impossible situations — saving a life while knowing that person will be back in the same state tomorrow.
“Burnout is … emotional exhaustion, depersonalization, and reduced personal accomplishment,” she said in an emailed statement. “High call volumes, lack of support or follow-up care for patients, and/or bureaucratic constraints … can increase the risk of reduced empathy, absenteeism and increased turnover.”
Kamkar says moral injury affects all branches of public safety, not just paramedics. Firefighters, who are often the first to arrive on the scene, face trauma from overdose deaths. Police report distress enforcing laws that criminalize suffering.
Understaffed and overburdened
Staffing shortages are another major stressor.
“First responders were amazing during the pandemic, but it also caused a lot of fatigue, and a lot of people left our business because of stress and violence,” said Marc-André Périard, vice president of the Paramedic Chiefs of Canada.
Nearly half of emergency medical services workers experience daily “Code Blacks,” where there are no ambulances available. Vacancy rates are climbing across emergency services. The federal government predicts paramedic shortages will persist over the coming decade, alongside moderate shortages of police and firefighters.
Unsafe work conditions are another concern. Responders enter chaotic scenes where bystanders — often fellow drug users — mistake them for police. Paramedics can face hostility from patients they just saved, says Périard.
“People are upset that they’ve been taken out of their high [when Naloxone is administered] and not realizing how close to dying they were,” he said.
Thomas says safety is undermined by vague, inconsistently enforced policies. And efforts to collect meaningful data can be hampered by a work culture that punishes reporting workplace dangers.
“If you report violence, it can come back to haunt you in performance reviews” he said.
Some hesitate to wait for police before entering volatile scenes, fearing delayed response times.
“[What] would help mitigate violence is to have management support their staff directly in … waiting for police before arriving at the scene, support paramedics in leaving an unsafe scene … and for police and the Crown to pursue cases of violence against health-care workers,” Thomas said.
“Right now, the onus is on us … [but once you enter], leaving a scene is considered patient abandonment,” he said.
Upstream solutions
Carleton says paramedics’ ability to refer patients to addiction and mental health referral networks varies widely based on their location. These networks rely on inconsistent local staffing, creating a patchwork system where people easily fall through the cracks.
“[Any] referral system butts up really quickly against the challenges our health-care system is facing,” he said. “Those infrastructures simply don’t exist at the size and scale that we need.”
Périard agrees. “There’s a lot of investment in safe injection sites, but not as much [resources] put into help[ing] these people deal with their addictions,” he said.
Until that changes, the cycle will continue.
On May 8, Alberta renewed a $1.5 million grant to support first responders’ mental health. Carleton welcomes the funding, but says it risks being futile without also addressing understaffing, excessive workloads and unsafe conditions.
“I applaud Alberta’s investment. But there need to be guardrails and protections in place, because some programs should be quickly dismissed as ineffective — but they aren’t always,” he said.
Carleton’s research found that fewer than 10 mental health programs marketed to Canadian governments — out of 300 in total — are backed up by evidence showing their effectiveness.
In his view, the answer is not complicated — but enormous.
“We’ve got to get way further upstream,” he said.
“We’re rapidly approaching more and more crisis-level challenges… with fewer and fewer [first responders], and we’re asking them to do more and more.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
News release from Alberta RCMP
Virtual Opioid Dependency Program serves vulnerable population in Red Deer
Since April 2024, your Alberta RCMP’s Community Safety and Well-being Branch (CSWB) has been piloting the Virtual Opioid Dependency Program (VODP) program in Red Deer to assist those facing opioid dependency with initial-stage intervention services. VODP is a collaboration with the Government of Alberta, Recovery Alberta, and the Alberta RCMP, and was created to help address opioid addiction across the province.
Red Deer’s VODP consists of two teams, each consisting of a police officer and a paramedic. These teams cover the communities of Red Deer, Innisfail, Blackfalds and Sylvan Lake. The goal of the program is to have frontline points of contact that can assist opioid users by getting them access to treatment, counselling, and life-saving medication.
The Alberta RCMP’s role in VODP:
- Conducting outreach in the community, on foot, by vehicle, and even UTV, and interacting with vulnerable persons and talking with them about treatment options and making VODP referrals.
- Attending calls for service in which opioid use may be a factor, such as drug poisonings, open drug use in public, social diversion calls, etc.
- Administering medication such as Suboxone and Sublocade to opioid users who are arrested and lodged in RCMP cells and voluntarily wish to participate in VODP; these medications help with withdrawal symptoms and are the primary method for treating opioid addiction. Individuals may be provided ongoing treatment while in police custody or incarceration.
- Collaborating with agencies in the treatment and addiction space to work together on client care. Red Deer’s VODP chairs a quarterly Vulnerable Populations Working Group meeting consisting of a number of local stakeholders who come together to address both client and community needs.
While accountability for criminal actions is necessary, the Alberta RCMP recognizes that opioid addiction is part of larger social and health issues that require long-term supports. Often people facing addictions are among offenders who land in a cycle of criminality. As first responders, our officers are frequently in contact with these individuals. We are ideally placed to help connect those individuals with the VODP. The Alberta RCMP helps those individuals who wish to participate in the VODP by ensuring that they have access to necessary resources and receive the medical care they need, even while they are in police custody.
Since its start, the Red Deer program has made nearly 2,500 referrals and touchpoints with individuals, discussing VODP participation and treatment options. Some successes of the program include:
- In October 2024, Red Deer VODP assessed a 35-year-old male who was arrested and in police custody. The individual was put in contact with medical care and was prescribed and administered Suboxone. The team members did not have any contact with the male again until April 2025 when the individual visited the detachment to thank the team for treating him with care and dignity while in cells, and for getting him access to treatment. The individual stated he had been sober since, saying the treatment saved his life.
- In May 2025, the VODP team worked with a 14-year-old female who was arrested on warrants and lodged in RCMP cells. She had run away from home and was located downtown using opioids. The team spoke to the girl about treatment, was referred to VODP, and was administered Sublocade to treat her addiction. During follow-up, the team received positive feedback from both the family and the attending care providers.
The VODP provides same-day medication starts, opioid treatment transition services, and ongoing opioid dependency care to people anywhere in Alberta who are living with opioid addiction. Visit vodp.ca to learn more.
“This collaboration between Alberta’s Government, Recovery Alberta and the RCMP is a powerful example of how partnerships between health and public safety can change lives. The Virtual Opioid Dependency Program can be the first step in a person’s journey to recovery,” says Alberta’s Minister of Mental Health and Addiction Rick Wilson. “By connecting people to treatment when and where they need it most, we are helping build more paths to recovery and to a healthier Alberta.”
“Part of the Alberta RCMP’s CSWB mandate is the enhancement of public safety through community partnerships,” says Supt. Holly Glassford, Detachment Commander of Red Deer RCMP. “Through VODP, we are committed to building upon community partnerships with social and health agencies, so that we can increase accessibility to supports in our city and reduce crime in Red Deer. Together we are creating a stronger, safer Alberta.”

COWBOY UP! Pierre Poilievre Promises to Fight for Oil and Gas, a Stronger Military and the Interests of Western Canada

Court compels RCMP and TD Bank to hand over records related to freezing of peaceful protestor’s bank accounts

Canada’s euthanasia regime is already killing the disabled. It’s about to get worse
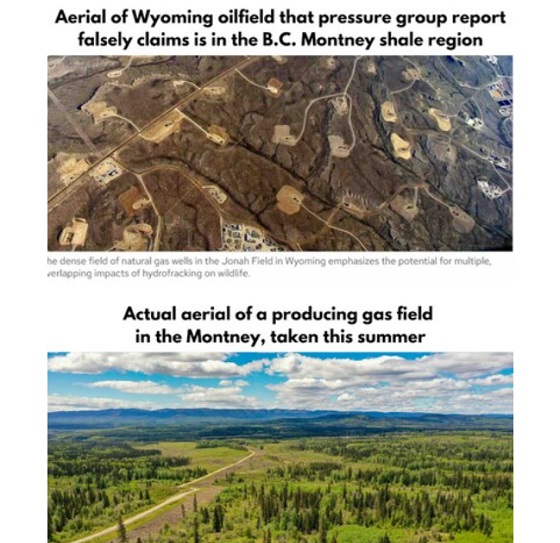
B.C. Residents File Competition Bureau Complaint Against David Suzuki Foundation for Use of False Imagery in Anti-Energy Campaigns
-
Alberta2 days ago
COWBOY UP! Pierre Poilievre Promises to Fight for Oil and Gas, a Stronger Military and the Interests of Western Canada
-
MAiD1 day ago
Canada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Crime2 days ago
Crime2 days agoEyebrows Raise as Karoline Leavitt Answers Tough Questions About Epstein
-
 Alberta2 days ago
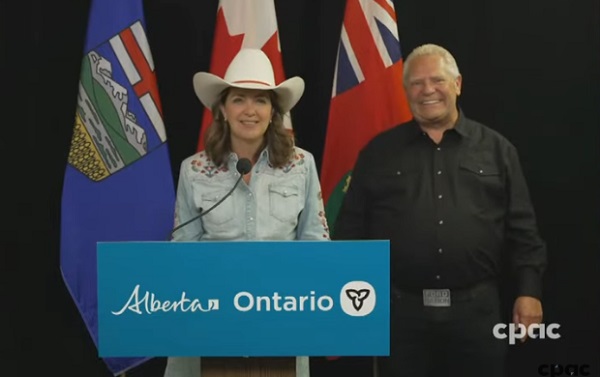
Alberta2 days agoAlberta and Ontario sign agreements to drive oil and gas pipelines, energy corridors, and repeal investment blocking federal policies
-
 Fraser Institute24 hours ago
Fraser Institute24 hours agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million from 2016 to 2024
-
 Censorship Industrial Complex13 hours ago
Censorship Industrial Complex13 hours agoCanadian pro-freedom group sounds alarm over Liberal plans to revive internet censorship bill
-
 Daily Caller1 day ago
Daily Caller1 day ago‘I Know How These People Operate’: Fmr CIA Officer Calls BS On FBI’s New Epstein Intel
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV